

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With age, men experience decreases in important health indicators like muscle amount, physical activity, and sexual drive. Furthermore, lower urinary tract symptoms (LUTS) are highly prevalent in males, and it has been clearly shown that the prevalence of LUTS increases with age [1]. The incidence of erectile dysfunction (ED) also increases with age, as does the incidence of cardiovascular disease risk factors, such as hypertension, obesity, and diabetes.
Additionally, ED has a significant negative impact on quality of life (QoL). Satisfaction with sexual life and the existence of LUTS severely affect men's QoL and plague middle-aged men's health [2]. Numerous studies have assessed QoL in men with LUTS, benign prostatic hyperplasia (BPH), and ED, but an estimation of middle-aged men's health in comparison to other comprehensive clinical parameters has not been reported previously in Korea.
Questionnaires are one of the most commonly used techniques for collecting health-related information in clinical studies because of their ease and simplicity [3]. The International Prostate Symptom Score (IPSS) questionnaire is used worldwide to measure LUTS [1]. To evaluate various voiding symptoms, perineal or suprapubic pain, and sexual disturbance, The National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) is used to assess chronic prostatitis (CP)/chronic pelvic pain syndrome [4]. The androgen deficiency in aging males (ADAM), premature ejaculation diagnostic tool (PEDT), and Internal Index of Erectile Function-5 (IIEF-5) questionnaires are used worldwide to evaluate men's sex lives [5]. By using these five questionnaires to evaluate detailed clinical problems, we proposed to research several factors affecting middle-aged men's general health.
We evaluated the relationship of various clinical parameters that are related to men's general health and the symptom scores of five widely used questionnaires for detecting men's health problems. We determined the predictive abilities of two obesity indexes and other clinical parameters for screening for LUTS and sexual dysfunction in middle-aged men. We believe that this study may not only provide a clearer figure of the suffering caused in middle-aged men's QoL, but also widen the public's understanding of middle-aged men's general health.
MATERIALS AND METHODS
1. Study design
Between March and September 2013, a total of 1910 healthy Korean men aged 40 to 59 years who participated in a health examination were included. The subjects grew up in various cities and were recruited from our institution. All men underwent detailed clinical evaluations by use of the IPSS, NIH-CPSI, ADAM, IIEF-5, and PEDT questionnaires. Anthropometric measurements, including height, weight, and waist circumference, were determined. Blood and urine samples were obtained for serum prostate-specific antigen (PSA) and testosterone measurement between 0700 and 0900. The estimated glomerular filtration rate (eGFR) was calculated and metabolic syndrome (MetS) was evaluated. The eGFR was calculated by using the abbreviated four-variable Modification of Diet in Renal Disease equation [6]:
MetS was defined by using the criteria established by the National Cholesterol Education Program-Adult Treatment Panel III published in 2005 [7]. MetS was diagnosed when at least three of the following criteria were present: (1) waist circumference greater than 90 cm or body mass index (BMI) higher than 25 kg/m2, (2) systolic blood pressure 130 mmHg or greater or diastolic blood pressure 85 mmHg or greater or use of antihypertensive medication, (3) fasting blood sugar greater than 110 mg/dL or self-reported diabetes medication use, (4) triglyceride greater than 150 mg/dL, and (5) high-density lipoprotein cholesterol less than 45 mg/dL or use of lipid medication [7]. Thereafter, all of the participants underwent a digital rectal examination (DRE) to screen for prostate enlargement or nodules suggesting prostate cancer. Next, transrectal ultrasound (TRUS) was performed and ultrasonographic inspection of the prostate was performed in each subject by using a 3.5-MHz transducer (Voluson 730, General Electronic, Milwaukee, WI, USA).
Prostate volume was measured by using the prostate ellipsoid formula, multiplying the largest anteroposterior (height, H), transverse (width, W), and cephalocaudal (length, L) prostate diameters by 0.524 (HxWxLxII/6) by using TRUS [8]. BMI was calculated as the weight (kg) divided by the square of the height (m), and waist-to-hip ratio (WHR) was determined as the waist circumference divided by the hip circumference [9]. Waist circumference was measured by placing a tape measure snugly at the horizontal level between the subcostal margin and pelvic brim [10]. Exclusion criteria included presence of pyuria (white blood cells>5 on urinalysis), the presence of neurogenic bladder dysfunction, confirmed prostate cancer, a history of recurrent urinary tract infections or bladder stones, or any other history of lower urinary tract disorder influencing urination. In addition, individuals who used medications affecting prostate growth, such as anti-androgens and 5-α-reductase inhibitors, or who had abnormal findings on the DRE were excluded from the study.
2. Statistical analysis
T-tests were conducted to compare the differences in men's general health scores according to other parameters, such as PSA, testosterone level, eGFR, and total prostate volume (TPV). Chi-square or Fisher exact test were conducted to compare the differences in mens' general health scores according to MetS, obesity, and central obesity. The results were expressed as mean±standard deviation or proportion values. Univariate and multivariate logistic regression analyses were performed for each group to determine the significance of age, PSA, testosterone, eGFR, and TPV as predictors of men's health problems.
The results were considered statistically significant when p<0.05. Statistical analyses were performed by using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Patient characteristics
Among 1,910 participants, 1,899 patients completed urological and psychiatric evaluations and did not meet the previous exclusion criteria. The median age of the patients was 53 years, and the median values of BMI and WHR were 24.8 kg/m2 and 0.93, respectively. BMI was categorized into two groups: nonobese (<24.8 kg/m2) and obese (≥24.8 kg/m2) because 24.8 kg/m2 was the median value in the healthy volunteers. We also divided the patients into two groups by their WHR, either above or below 0.93, the median value in the healthy volunteers. The data on the patients' ages, serum PSA levels, and testosterone levels and the results of the anthropometric measurements are summarized in Table 1. In addition, the median scores on the IPSS, NIH-CPSI, ADAM, IIEF-5, and PEDT are summarized in Table 1.
2. Differences in men's general health score according to various parameters
We examined men's general health by using several clinical parameters, including obesity-related parameters. To analyze differences in men's general health according to various clinical parameters, we divided the five questionnaire groups into two subgroups each depending on the degree of symptom severity (Table 2).
In this study, moderate to severe LUTS was defined as an IPSS score≥8, and the group with moderate to severe LUTS had relatively greater TPV than did the group with no or mild LUTS (p=0.001). Other clinical parameters were not significantly different between the two groups divided by severity of LUTS.
Moderate to severe NIH-CPSI was defined as a score over 14, and inversely, those men showed a lower prevalence of MetS (p=0.023) than did men in the group with no or mild CPSI. Other clinical parameters, including obesity-related parameters, did not differ significantly between the two groups divided by severity of NIH-CPSI.
To evaluate the sex life of the patients, we divided the subjects by IIEF-5 score. Moderate to severe ED was defined as a score less than 12. In this study, the group with moderate to severe ED showed a relatively higher prevalence of MetS (p=0.012) and central obesity (measured by WHR≥0.93) (p<0.001). There were no statistically significant differences in other clinical parameters between the two groups divided according to the severity of their IIEF-5 scores.
For the two remaining questionnaires, ADAM and PEDT, there were no significant differences between subgroups.
3. Factors influencing LUTS
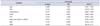
We evaluated the predictive value of several factors for moderate to severe LUTS by looking at IPSS scores over 7. Multiple logistic regression analyses revealed that age and total TPV were independent predictors of moderate to severe LUTS in the multivariate analysis (p=0.001, odds ratio [OR], 1.034; 95% confidence interval [CI], 1.014-1.056; p=0.010, OR, 1.019; 95% CI, 1.004-1.033; respectively) (Table 3)
4. Factors influencing CP symptoms
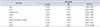
We evaluated the predictive value of several factors for moderate to severe CP-like symptoms by NIH-CPSI scores over 14. As determined by logistic regression analysis, MetS was the only significant negative predictive factor for moderate to severe CPSI scores (p=0.022; OR, 0.747; 95% CI, 0.581-0.959) (Table 4).
5. Factors influencing symptoms related to androgen deprivation in aging males
We evaluated the predictive value of several factors for moderate to severe aging male's symptoms by ADAM scores over 36. Multiple logistic regression analyses revealed that age was the only significant independent predictor for moderate to severe ADAM score (p=0.018; OR, 1.024; 95% CI, 1.004-1.045). There were no significant predictive factors except age (Table 5). Aging definitely causes late-onset hypogonadism.
6. Factors influencing ED
The degree of ED was considered moderate to severe when the score on the IIEF-5 questionnaire was 11 or lower. The logistic regression analysis showed that age and MetS were independent predictive factors for moderate to severe ED in the multivariate analysis (p<0.001, OR, 1.121; 95% CI, 1.087-1.156; p=0.036, OR, 1.323; 95% CI, 1.018-1.720; respectively). WHR had a statistically significant value for predicting moderate to severe ED in the univariate analysis (p=0.016; OR, 47.683; 95% CI, 2.080-1,093.027) (Table 6). Thus, higher age, existence of MetS, and central obesity measured by WHR had predictive ability for ED.
DISCUSSION
Because QoL has improved in recent years, more attention is being paid to diseases that influence QoL rather than to only life-threatening diseases. LUTS, ED, and premature ejaculation are such diseases that affect QoL in elderly men. To further our understanding about the seriousness of middle-aged men's health, we assessed the severity of men's urinary tract symptoms, sexual function, and premature ejaculation by using validated questionnaires.
Over the past decades, many different groups have investigated the influence of obesity on the development of BPH and LUTS with conflicting results. Most of these groups concluded that overall obesity, abdominal obesity, and WHR can increase the risk of BPH and LUTS, at least to some degree [11].
In our study, to minimize the effect of comorbidity by senility, the age of patients was confined to 40 to 59 years, representing middle-aged men. A total of 1899 healthy Korean men aged 40 to 59 years were included, and the age range was selected because it encompassed the aged most closely associated with prostatitis and ED.
The outcomes of this study included several interesting findings that deserve further explanation. First, we showed that clinical parameters including obesity-related parameters did not differ significantly between the groups divided by IPSS, NIH-CPSI, IIEF-5, ADAM, and PEDT scores, except for TPV and MetS. Our results indicated that the group with moderate to severe LUTS had a relatively greater TPV. Second, the group with moderate to severe NIH-CPSI scores had a lower prevalence of MetS. Third, according to IIEF-5, the group with moderate to severe ED showed a relatively higher prevalence of MetS and central obesity as measured by WHR. Fourth, we showed that age and TPV were associated with more severe LUTS. Fifth, MetS was the only significant negative predictive factor for moderate to severe CPSI scores. We could not find a definite reason for the negative relationship between MetS and CP-like symptoms in our study. However, we suspect that effects of dietary and healthy behaviors could be important issues in this relationship. Bartoletti et al. [12] suggested that CP/chronic pelvic pain syndrome (CPPS) is a multifactorial disease. Cigarette smoking, a high-calorie diet with low fruit and vegetable consumption, constipation, slow digestion, a sexual relationship with more than one partner, and coitus interruptus were more likely in patients with CP/CPPS than in controls [12]. In addition, Zhang et al. [13] reported that higher leisure-time physical activity was associated with a lower risk of CP/CPPS. Patients diagnosed with MetS often give a lot of attention to their eating habits and lifestyle. The significance of behavior-induced CP-like symptom reduction is still unknown. Further studies are needed to better characterize the etiopathogenesis in individuals to define the optimal approach to diagnosis and treatment. Sixth, we revealed that age was the only significant independent predictor for moderate to severe ADAM scores. Finally, we revealed that aging, the existence of MetS, and central obesity measured by WHR had predictive ability for ED. Interestingly, we found no evidence that higher BMI in middle age is associated with an increased risk of LUTS, ED, or other related men's health concerns. In contrast, WHR was strongly and independently related to ED. Overall, there are clear advantages of using WHR; it is convenient and simple to measure and an easy metric in diagnosing not only the sequelae normally associated with MetS, but also voiding dysfunction [10].
WHR may therefore be both useful and important as a measure of success for possible future treatment options for patients with ED. Active reduction of waist circumference via treatment of MetS in addition to treatment of pelvic inflammation and ischemia may lead to durable and material improvement in ED. Other studies have also shown that weight loss significantly improves insulin sensitivity, erectile function, and testosterone levels in men [10].
To our knowledge, this is first study simultaneously assessing several clinical parameters including obesity-related parameters and the five questionnaires for assessing middle-aged men's health. We studied a large number of subjects in a population-based study, and there are few Asian studies in which more than 1,500 subjects were analyzed. This is the first large-scale study of Korean middle-aged men using the five validated questionnaires. The number of patients in this study was large enough to achieve a representation of middle-aged men. Although several studies have shown an association of LUTS and obesity, there are few studies regarding the effects of the five validated questionnaires representing men's urinary symptoms and sexual function according to several clinical parameters [11]. Our data showed median values and several functional status indexes of middle-aged Korean men.
However, our study had several specific limitations. Although the five questionnaires that we used were validated, studies based on questionnaires have limitations in that they do not include basic disease development and limited information can be obtained, particularly regarding diagnostics. Because we only used the five questionnaires to assess LUTS and sexual function, we lacked the detailed medical and social history of the patients. Another limitation of this study was that the data were cross-sectional and did not provide information regarding the temporal cause-effect relationship between the clinical parameters and middle-aged men's general health. The baseline demographics of the men enrolled in this study were not fully inspected or randomized; thus, the baseline comorbidity of each patient may have affected the patients' responses to the questionnaires. Because this study consisted of data from a single institution, there may be a potential selection bias as well. In the future, local population-based studies and randomized controlled trials will be needed. Despite these limitations, it is meaningful that this study showed a relationship of several clinical parameters with middle-aged men's general health in a population-based study.
CONCLUSIONS
Our data showed that TPV is a significant predictor of LUTS, and our results indicated that age and TPV were associated with the severity of LUTS symptoms. MetS was the only significant negative predictive factor for CP-like symptoms. It is suggested that patients with MetS are not prone to CP-like symptoms. Aging definitely causes late-onset hypogonadism. Also, we showed that aging, the existence of MetS, and central obesity measured by WHR had predictive ability for ED. WHR is a convenient and simple measurement, so it may therefore be useful and important as a measure of success for future treatment.




 XML Download
XML Download