

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Underactive bladder (UAB) has not yet been formally defined but has been suggested to be a clinical manifestation of detrusor underactivity characterized by a weak, poorly sustained urinary stream and high postvoid residual urine volume (PVRU) [1]. Although voiding lower urinary tract symptoms (LUTS) constitute the major discomfort of UAB, storage LUTS such as frequency, nocturia, and incontinence are often present. Many authors have used their own working definitions for detrusor underactivity or UAB while conducting basic and clinical research. In this review, for simplicity of description, the term UAB will be used to represent each of the relevant working definitions of detrusor underactivity or UAB in the references.
UAB is basically an emptying failure resulting from insufficient generation of adequate intravesical pressure to void. The bladder performs the main role in generating intravesical pressure and is generally regarded as the target organ in the management of UAB. However, it should be noted that many other pathologies in the voiding reflex arc or bladder outlet can contribute to the development of UAB, which may be other potential targets for management [2].
Regardless of the cause of UAB in each patient, the management strategy should focus on improving the patient's quality of life and delaying the development of possible complications, such as recurrent urinary tract infections, bladder stones, and upper urinary tract damage leading to chronic renal failure [3]. Although the natural history of UAB is still not fully understood, observation may be an acceptable management option for patients with tolerable LUTS and little risk of upper urinary tract damage. The low-pressure bladder in some UAB patients may protect the upper urinary tract from self-inflicted pressure damage. In a long-term follow-up study of untreated UAB (69 male patients), 84% remained untreated after a mean follow-up of 13.6 years [4]. No significant clinical changes were reported over the follow-up periods.
So far, no generally accepted guidelines are available on the management of UAB. As an effective and safe add-on therapy, scheduled voiding and double voiding may be recommended to avoid overdistension and decrease PVRU [3]. However, manual external bladder compression (Credé maneuver) or abdominal straining (Valsalva maneuver) are not recommended owing to the risk of developing high intravesical pressure and upper tract damage. Moreover, these maneuvers can elicit a reflex sphincter contraction with the result of increasing outlet resistance [56].
If the patient's overall clinical condition indicates risk of progression or worsening of intolerable LUTS, therapeutic intervention including catheterization or pharmacological or surgical management options should be considered. Many management options have been developed to enhance bladder emptying in each step of the voiding process. Traditional approaches focus on the bladder, the final target organ in the process, to increase detrusor contractility by stimulating neurotransmitter secretion or adding more detrusor power. Modulation of the neural circuit involving the voiding reflex and central nervous system (CNS) facilitates a coordinated detrusor contraction. Also, decreasing outlet resistance by medication or surgery can work in a select group of UAB patients.
PHARMACOLOGICAL THERAPY
1. Parasympathomimetics
The first strategy for UAB pharmacotherapy is to increase detrusor contractility. Since detrusor contraction is mediated by parasympathetic innervation, enhancement of parasympathetic activity would be expected to increase detrusor contraction. Parasympathomimetics are substances to stimulate the parasympathetic nervous system in the body. Parasympathomimetics can act either directly by stimulating the muscarinic receptors or indirectly by inhibiting cholinesterase and thus promoting acetylcholine release [7].
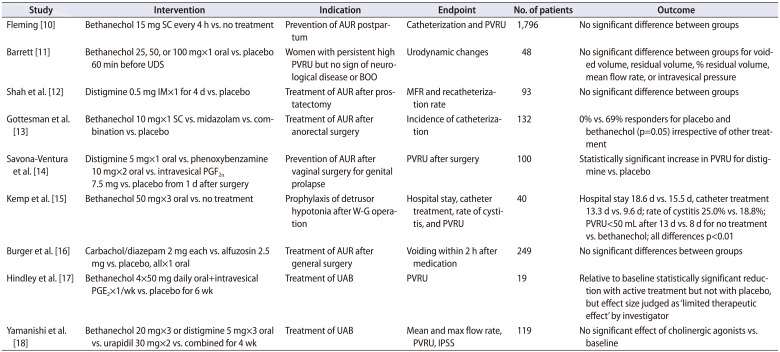
Bethanechol chloride is a parasympathomimetic choline carbamate that selectively stimulates muscarinic receptors with little effect on nicotinic receptors. Distigmine bromide is an acetylcholinesterase inhibitor that inhibits the acetylcholinesterase enzyme from deactivating acetylcholine, thereby increasing both the level and duration of action of acetylcholine in neuromuscular junctions. Considering their inherent pharmacological activity, both agents may well enhance detrusor contractility and have been widely used for UAB management for decades. However, clinical data show conflicting results (Table 1).
A systemic review by Barendrecht et al. [8] concluded that the evidence does not support the use of parasympathomimetics to treat UAB, specifically when potential adverse effects are taken into account. The potential adverse effects include nausea, vomiting, diarrhea, gastrointestinal cramps, bronchospasms, salivation, sweating, headache, flushing, visual accommodation defect, and the rare but potentially lethal complication of cardiac arrest [9]. Because of the risk of potential adverse effects, clinicians tend to be reluctant to increase the dose of parasympathomimetics, which may contribute to unsatisfactory clinical efficacy. Along with the low-dose issue, a state of complete myogenic failure of the detrusor could be another probable reason for nonresponsiveness.
Riedl et al. [19] showed that electromotive administration of intravesical bethanechol was helpful for identifying a bethanechol-effective subgroup. The test consisted of an intravesical instillation of 20-mg bethanechol in 150 mL of 0.3% sodium chloride with and without a 20-mA current applied via an electrode catheter. In another study, the bladder electrical perception threshold was suggested to identify UAB patients likely to respond to bethanechol [20]. Increased bladder sensitivity as determined by an electrical perception threshold test indicates enhanced bladder emptying with subcutaneous injection of bethanechol.
2. Alpha-adrenergic blockers
Chronic bladder outlet obstruction (BOO) has been suggested as a risk factor for UAB. It has been well documented that experimental chronic BOO causes irreversible damage to the detrusor resulting in detrusor underactivity [2122]. Especially in elderly patients with a large prostate, BOO may play a main role in the development of UAB. Alpha-adrenergic blockers (ABs) have been widely used to relieve BOO and enhance bladder emptying in patients with neurogenic lower urinary tract dysfunction those with benign prostatic hyperplasia. Improvement of pelvic ischemia may contribute to the pharmacological effect of ABs in voiding dysfunction [23242526].
However, it is still unclear whether the clinical benefit of ABs for UAB comes from modulating the bladder itself or from a hidden component of BOO. Chang et al. [27] reported the efficacy of ABs in female patients with voiding difficulty and a subnormal maximal flow rate (MFR). After 6 weeks of therapy with 0.2-mg tamsulosin, a good therapeutic response, defined as achieving more than a 50% decrease in voiding symptom score and more than a 30% increase in MFR, was observed in 35.1% of the patients. In the subgroup analysis based on urodynamic study (UDS), a good therapeutic response was observed in 39.4% of patients with BOO and 32.7% of patients with UAB [27].
Combination therapy with cholinomimetics and ABs was shown to be more effective than monotherapy in patients with UAB [18]. The patients were assigned to 3 groups: a cholinomimetics group taking bethanechol chloride (60 mg/d) or distigmine bromide (15 mg/d); an AB group taking urapidil (60 mg/d); and a combination group taking both medications. After 4 weeks, International Prostate Symptom Score (IPSS) and PVRU were significantly decreased in the AB group and the combination group while they remained unchanged in the cholinomimetics group. The average and maximum flow rates significantly increased only in the combination group. PVRU decreased significantly in the AB group (p=0.0043) and the combination group (p=0.0008).
The efficacy of ABs has not yet been clearly demonstrated and the level of evidence remains weak. However, selective ABs may contribute to enhancing voiding efficiency and decreasing possible upper urinary tract damage. ABs may well be considered as an acceptable initial therapy in patients with UAB and chronic retention.
3. Prostaglandin E2
Prostaglandin E2 (PGE2) is a naturally occurring prostaglandin which functions as a direct vasodilator and smooth muscle relaxer. It also inhibits the release of noradrenaline from sympathetic nerve terminals. Experimental studies have shown that PGE2 can stimulate detrusor contraction directly, enhance the efficacy of other contraction-mediating transmitters, and potentiate afferent transmissions [28].
Andersson et al. [29] reported that intravesical PGE2 induces a significant increase in intravesical pressure and a decrease in maximum urethral closing pressure. In a prospective study of 36 patients with UAB, 72% showed improvement in detrusor function after intravesical PGE2 administration [30]. A prolonged benefit was observed in 39%, especially in patients with an intact sacral reflex arc, in patients with urodynamic evidence of a pathologically enlarged bladder, and in patients without outflow obstruction.
However, in a prospectively randomized double-blind study of 28 patients with urinary retention after anterior colporrhaphy, intravesical PGE2 on postoperative days 6 and 7 showed no significant effect on PVRU compared with placebo [31]. Combination therapy of intravesical PGE2 and oral bethanechol chloride showed limited benefit compared with the placebo combination [17]. Before treatment, the median PVRU was 426 mL for those receiving both drugs; this decreased to 325 mL after 6 weeks (p<0.015). In the placebo combination group, respective values were 576 and 538 mL (p=0.09). Only 4 of 9 patients in the active combination group reported symptomatic improvement and were able to reduce the frequency of clean intermittent catheterization.
Even though there was evidence of a pharmacological effect, PGE2 had a limited therapeutic effect compared with placebo in clinical trials. Therefore, intravesical PGE2 would not be recommend as a routine treatment, but may be considered as an additive therapeutic regimen in UAB patients performing clean intermittent catheterization or those with an indwelling catheter.
4. Acotiamide
Acotiamide is an oral, first-in-class prokinetic drug that modulates upper gastrointestinal motility to alleviate abdominal symptoms resulting from hypomotility and delayed gastric emptying [32]. The pharmacological action of acotiamide exerts an antagonistic effect on muscarinic receptors to inhibit the negative feedback system by blocking the muscarinic auto receptors that regulate acetylcholine release. Hence, acotiamide enhances parasympathetic activity by increasing acetylcholine release as well as by inhibiting acetylcholinesterase activity.
Sugimoto et al. [33] conducted a small pilot study of 19 UAB patients treated with oral acotiamide. After 2 weeks of acotiamide hydrochloride hydrate at a dose of 100 mg 3 times daily, the drug was generally well tolerated with little adverse effect. PVRU showed a significant decrease from 161.4±90.0 mL at baseline to 116.3±63.1 mL at the end of the study (p=0.006). To further determine the clinical efficacy of acotiamide, a prospective randomized controlled study would be warranted in the near future.
SURGICAL MANAGEMENT
1. Electrical stimulation/neuromodulation
Transurethral intravesical electrical stimulation (IVES) may activate specific mechanoreceptors and the intramural motor system in the detrusor, which sequentially leads to local muscle contractions. These contractions stimulate afferent pathways, the CNS, and efferent pathways, which make more coordinated and enhanced detrusor contractions. Theoretically, IVES can be applied in patients with an incomplete spinal cord lesion.
IVES has a long history of use in bladder rehabilitation to facilitate voiding and decrease PVRU in the management of neurogenic bladder associated with meningomyelocele [34]. Primus et al. [35] reported that detrusor contraction was achieved in 39%, bladder sensation in 75%, and catheter-free status in 54% of patients after IVES. Lombardi et al. [36] reported the efficacy of IVES in patients with incomplete spinal cord lesion with chronic neurogenic nonobstructive urinary retention. Significant predictive parameters for IVES success were a timespan of less than 2 years from the onset of spinal cord lesion and the presence of first sensation of bladder filling at baseline [36]. The relevant study results so far suggest that the clinical efficacy of IVES is rather short-term and tends to decrease with time [3637].
Sacral nerve modulation (SNM) modulates pelvic/perineal afferent pathways, which increase parasympathetic activity in the bladder while inhibiting the sympathetic urethral and somatic sphincter components in guarding the reflex to relax outlet [37]. Therefore, an intact neural circuit for the voiding reflex is mandatory to achieve clinical efficacy from SNM.
Lombardi et al. [38] compared IVES and SNM in 77 patients with incomplete spinal cord lesion and neurogenic nonobstructive urinary retention. After sequential test stimulation, 29 patients (37.6%) responded to both IVES and first-stage SNM. Whereas all IVES responders returned to the baseline state after 9.6 months of mean follow-up, only 34.5% of the responders became nonresponsive to permanent SNM after 54 months of mean follow-up. Permanent SNM showed a significantly longer clinical benefit than IVES [38]. In another study, 36 of 85 patients (42.4%) classified as responders after first-stage SNM, and 34 patients proceeded to permanent SNM. Eleven inconstant responders who returned to baseline at follow-up responded again with an implant on the contralateral S3 sacral root. Two patients who failed twice responded to an S4 sacral root implant. Only one failure was reported after more than 3 years of follow-up after permanent SNM [39].
In a multicenter, prospective randomized controlled study of patients with idiopathic urinary retention refractory to standard therapy, 68 of 177 patients (38.4%) had more than 50% improvement after first-stage SNM [40]. In 37 patients, permanent SNM proceeded immediately and voluntary voiding was restored in 69% of the patients at 6 months. An additional 14% of patients had a more than 50% reduction in catheterized volume per catheterization. Overall successful results were reported in 83% of the SNM group compared with 9% of the control group at 6 months. Temporary inactivation of the implant resulted in a significant increase in PVRU, and the efficacy of SNM was sustained until 18 months of follow-up.
In 1999, the U.S. Food and Drug Administration (FDA) approved the Medtronic Interstim System for Urinary Control, an implantable electrostimulation device for SNM, for the treatment of urinary retention and refractory overactive bladder. So far, SNM is the only FDA-approved surgical management option for nonobstructive UAB.
2. Surgery to reduce BOO
As stated earlier, chronic BOO may lead to UAB. Surgery to reduce BOO, such as transurethral resection of the prostate (TURP), has been regarded as a viable management option for UAB combined with BOO. Many researchers have reported favorable short-term results of TURP [414243], prostatectomy with laser energy [4344454647], transurethral incision of the bladder neck [4849], or onabotulinumtoxinA injection on the bladder neck [5051] for patients with both BOO and UAB.
However, long-term studies have shown conflicting results on the effectiveness of BOO reduction surgery. Masumori et al. [52] reported that patients showed significantly better IPSS at 12 years after TURP than at baseline, although there was gradual deterioration with time. In patients without BOO, the IPSS deteriorated faster than in those with BOO, while neither UAB nor detrusor overactivity influenced the degree of change in IPSS. The quality of life index remained improved regardless of preoperative UDS findings. Noticeably, two-thirds of patients with UAB without BOO remained satisfied at 12 years. The results may be subject to bias, because only 47% of the initial patients were surviving at the time of the final evaluation [52]. In a 10-year follow-up study, Al-Hayek et al. [53] reported no significant change in the bladder contractility index (BCI) in patients with BOO after TURP. Also, the BCI in patients with untreated UAB showed no significant change. Noticeably, the BCI was higher in untreated patients with BOO than in the TURP group at the time of the final evaluation. Thomas et al. [54] also reported that no significant clinical improvement was observed in patients with UAB at 11 years of follow-up. Moreover, UAB patients with TURP showed significantly higher PVRU than did those without surgery.
A recent meta-analysis showed that the presence of UAB correlated with poorer IPSS and MFR improvement after surgery in patients with benign prostatic hyperplasia and UAB [55]. Although surgery to reduce BOO may be a viable treatment option in men with presumed BOO and reduced detrusor contractility, acontractile bladder usually indicates a poor prognostic sign [56]. In real clinical practice, there seems to be little role of surgery to reduce outlet resistance in patients with UAB but without BOO.
3. Reduction cystoplasty
Chronic urinary retention associated with BOO and/or detrusor underactivity commonly progresses to myogenic decompensation with rather large bladder capacity [57]. In a large decompensated bladder with detrusor underactivity without BOO, decreasing the large bladder capacity may be helpful to enhance emptying.
The theoretical background for reduction cystoplasty lies in the bladder biomechanics based on the Laplace law [58]. When applied to the bladder, the Laplace equation can be described as T=Pves×R/2d, where T is wall tension, P is intravesical pressure, R is the radius of the bladder, and d is wall thickness [59]. The equation indicates a direct relationship between wall tension and bladder diameter. If the bladder diameter is decreased by half after reduction cystoplasty, the wall tension can double under constant intravesical pressure.
Several surgical techniques for reduction cystoplasty have been suggested in the literature: fundus invagination (Stewart technique) [60], detrusor wrap (Zoedler technique) [61], and transection and resection of the superior bladder dome (Klarskov technique) [62]. However, the actual clinical outcomes for these techniques did not parallel the theoretical background. In a long-term follow-up report after reduction cystoplasty, bladder capacity and PVRU tended to increase over time [63]. Although the results were from a small series with mixed pathology and a different surgical approach, more favorable outcomes were reported in patients with hypocontractile detrusor function compared those with an acontractile detrusor [6264].
A criticism of reduction cystoplasty is that it may not increase detrusor contractility but rather only decrease bladder compliance, which may put the patient at risk of upper tract damage and overflow incontinence. Therefore, reduction cystoplasty has limited clinical feasibility in patients with UAB and should be considered very carefully in selected cases with some residual detrusor contractility.
4. Latissimus dorsi detrusor myoplasty
The concept for this surgical approach comes from the idea that voiding efficiency in UAB may be facilitated by wrapping the bladder with striated muscle to increase intravesical pressure. A rectus abdominis wrap was applied in early series but the functional results were unsatisfactory. The movement of the covered rectus failed to generate an effective downward force to compress the bladder. The other problem was the segmental innervation, which denervated most of the rectus after a major dissection [65].
The latissimus dorsi (LD) is a large, flat muscle on the back that is innervated by the thoracodorsal nerve. The muscle is a potential source for breast reconstruction after mastectomy [66] or dynamic cardiomyoplasty [67]. Dynamic cardiomyoplasty consists of wrapping the LD around the heart and electrostimulating the muscle in synchrony with ventricular systole. Latissimus dorsi detrusor myoplasty (LDDM) consists of wrapping the free LD muscle flap around the bladder and making a neurovascular anastomosis to the lowest motor branches of the intercostal nerve and deep inferior epigastric vessels.
On the basis of animal experiments [68], LDDM was first applied in 1998 in 3 patients with acontractile bladder requiring catheterization [69]. UDS at 12 months after LDDM showed restoration of self-voiding in all patients with an acceptable range of MFR (18–26 mL/s) and PVRU (0–90 mL). Contraction of the transplanted muscle was confirmed by ultrasonography and flow-mode computerized tomography [69].
A subsequent study reported that voluntary self-voiding was restored in 14 of 20 acontractile bladder patients (70%) with PVRU less than 100 mL [70]. Another four patients showed voluntary voiding after additional bladder neck incision. Mean postoperative detrusor pressure was 72 cmH2O. Functioning free muscle transplantation, LDDM, restored voluntary voiding in 90% of patients previously on long-term catheterization.
The first worldwide multicenter study of LDDM for acontractile bladder from lower motor neuron lesions showed restoration of voluntary voiding in 17 of 24 patients (71%) with a mean PVRU of 25 mL and a significant increase in the mean BCI [71]. In 3 patients (13%), the number of catheterizations was reduced to 2 to 4 times daily with a mean PVRU of 200 mL [71]. Idiopathic acontractile bladder in elderly patients showed a poor outcome, and it is suggested that special caution be taken in patients with no clear origin of bladder acontractility.
LDDM is an extensive and invasive surgery that requires a multidisciplinary team approach of urologists and plastic reconstructive experts in functional reconstruction. Although the results are based on a rather small number of studies, LDDM shows promise for restoring voluntary voiding especially in motivated young patients who hope to live a life without catheterization.
CONCLUSIONS
The current management of UAB remains unsatisfactory. Normal bladder emptying requires normal sensation, intact CNS control, and normal detrusor neurotransmission and contractility; derangements in any of these processes may result in UAB. The multifactorial nature of UAB pathogenesis complicates the appropriate management for each patient. A specific management strategy that focuses on only one aspect of UAB may not provide adequate therapeutic efficacy. Future research to establish a more clinically relevant definition of UAB will be required to open a new era of UAB management.
 XML Download
XML Download