

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Benign prostatic hyperplasia (BPH) is a pathological term with no universally accepted epidemiologic definition [1]. Lower urinary tract symptoms (LUTS) due to BPH are a common problem, particularly in older men. The prevalence of LUTS/BPH increases with age, affecting more than 70% of men older than 70 years [2]. The socioeconomic burden of BPH is tremendous, costing over $3 billion every year [3]. As life expectancy increases, so does this burden.
The prevalence of BPH or LUTS has been studied in many nationwide surveys from various regions including Europe, the United States, and Korea [45]. However, for the incidence of LUTS, not many reports have been published [678], and no study has reported the incidence of LUTS/BPH previously in Korea. The Health Insurance Review & Assessment (HIRA) service is a nationwide healthcare system in Korea, including health insurance and medical aid, covering all citizens. This nationwide database has the information regarding reimbursement including diagnosis, prescriptions and operations. Therefore, the incidence of LUTS/BPH as well as treatment patterns can be determined from it without follow-up loss.
Herein, we investigated the incidence of LUTS/BPH and treatment patterns for patients who were diagnosed in a year with 3 years of follow-up using a nationwide Korean database. Medication-free rate at 1 year after the surgery was also assessed.
MATERIALS AND METHODS
1. Study population
After the approval of institutional review board (H-1202-065-398), we extracted the data of patients who were diagnosed of BPH in the year of 2008 and their follow-up visits for 3 years from HIRA database. The diagnosis of BPH was defined as 2 or more records of reimbursement with the International Classification of Diseases, 10th revision (ICD-10) diagnosis code of N40.0 used as a primary or secondary diagnosis. The first diagnosis was defined as an index diagnosis and patients with an index diagnosis of 2008 were traced for 3 years. Patients diagnosed with BPH within the previous 12 months before the index diagnosis were excluded. Patients diagnosed with prostate cancer (ICD-10, C61) within the 12 months after the index diagnosis or having claims suggesting a prior prostatic surgery, prostate cancers, inflammatory diseases of the prostate, neurological diseases or conditions that could affect LUTS were also excluded (Table 1).
2. Incidence and treatment pattern
Incidence was calculated as the number of new cases identified in 2008 divided by the number of at-risk individuals. Age, mean and median numbers of office visits and the tier of hospital where the index diagnosis was made were identified.
To determine treatment patterns, patient status was determined every 3 months as medication, no medication, or surgery status. Medication status was defined as having a prescription record for ≥25% of the 3 months. Surgery was assigned as having a record of the following procedures: transurethral resection of the prostate (TURP, R3975), photoselective vaporization of the prostate (PVP, R3976), holmium laser enucleation of prostate (HoLEP, R3977), open prostatectomy (R3950), and thermal therapy (R3516). All the other situations were assigned as no medication status. Medications were categorized as alpha-blockers, 5-alpha reductase inhibitors, or anticholinergics. Alfuzosin, doxazosin, tamsulosin, terazosin, and silodosin were categorized as alpha-blockers. Dutasteride and finasteride were included as 5-alpha reductase inhibitors. Oxybutynin, propiverine, fesoterodine, solifenacin, and tolterodine were categorized as anticholinergics.
For those who underwent surgery once during the 3 years of follow-up, preoperative medication status was assessed 1 month prior to the surgery. For those who were taking medication 1 month prior to the surgery, medication-free rate was calculated 6–36 months postoperatively in 3-month intervals.
3. Statistical analysis
The patient status such as medication, no medication and surgery were assessed as categorical variables. Age in a decade was treated as a categorical variable. Logistic regression analysis was used to calculate odds ratios (ORs). IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA) was used for all analyses, and a p-value <0.05 was considered statistically significant.
RESULTS
1. Incidence of BPH
A total of 386,873 men were identified and included in the BPH cohort of 2008. The incidence of BPH was 2,105 per 100,000 men, and increased with age (Fig. 1A). Mean age was 59.7 years. For index patients who were diagnosed with BPH in 2008, median number of office visits was 7. Median follow-up period was 428 days. Most patients were diagnosed in cities (Fig. 1B) or at clinics (60%) (Fig. 1C).
2. Treatment of BPH
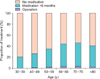
During the 3 years of follow-up, 27.1% of patients received medication for more than 9 months, 17.6% of patients took medication for more than a year. For the surgical treatment, 7,955 patients (2.1%) underwent surgery, including 252 patients who underwent surgery twice or more. The treatment rate increased with age until the age of 70 years (Fig. 2).
The timing of surgical treatment from the index diagnosis is shown in Fig. 3. During the first 3 months, 36.6% of patients underwent surgery. The cumulative incidence of surgical cases increased with time (Fig. 3A). The gradients of cumulative incidence were different between surgical methods (Fig. 3B).
TURP was the most commonly performed surgical procedure, followed by PVP and thermal therapy (Fig. 4). Open prostatectomy accounted for 1% of surgical treatments. As our cohort comprised patients diagnosed with BPH in 2008 and followed up until 2011, HoLEP constituted only 2% of BPH surgeries, as it has only been performed after 2010. Most surgically treated patients were in their 60s and 70s. Although the symptom severity was not assessed, older patients were more likely to receive treatment, with an OR of 1.56 for each additional decade (95% confidence interval, 1.55–1.58; p<0.001).
To assess medication free-rate, patients taking medication at 1 month preoperatively were assessed and traced until 3 years after the surgery (Fig. 5). At 1 month preoperatively, 50.5% of patients were taking medication. Alpha-blocker-containing regimens were the most common type of medication used, followed by 5-alpha reductase inhibitors. Medication-free rate at 1 year after the surgery was 82% on average. To calculate medication-free rate, we excluded HoLEP, because HoLEP had only been used in this cohort after 2010. Medication-free rate was highest for open prostatectomy (90.0%) and lowest for thermal therapy (78.1%). After 1 year, medication-free rate plateaued (average 82.9%), and at 36-month postsurgery, 83.9% of patients were not taking any medication. Among the patients who were taking medications at 36 months after the surgery, alpha-blockers were the most common type of medication used (alpha-blockers, A; 5-alpha reductase inhibitors, B; anticholinergics, C; A 5.2%, AB 3.9%, ABC 0.7%, AC 1.1%), and anticholinergic-containing regimens were maintained in 4.0% of patients, including anticholinergic monotherapy in 2.1% of patients. For those who were taking anticholinergics preoperatively, medication-free rate after 1 year was 73.3%, which was lower than the average, and 11.8% of them had maintained anticholinergics-containing regimens.
DISCUSSION
This study demonstrates the incidence of LUTS/BPH, their treatment patterns, and medication-free rates after the surgery in a 3-year follow-up in a population-based BPH cohort. The overall incidence of LUTS/BPH was found to be 15 cases per 1,000 man-years in the Triumph project from the Netherlands from 1995 to 2000 [6]. This trend was similar in UK, too [7]. Our study showed similar or slightly higher incidence rates compared to those in these studies. Differences in time period, population size, and age distribution could have affected the result.
LUTS is a dynamic condition that can improve or progress [9101112]. A few reports have focused on the longitudinal changes of LUTS in population-based studies [8121314]. In our study, less than one in 5 (17.6%) initially diagnosed patients continued medication for >1 year, which could be partially explained by the dynamic nature of LUTS.
Many previous studies have shown that patients with more profound or bothersome symptoms are more likely to visit clinics and seek medical care [971215]. Men who reported worse symptoms at baseline were four times more likely to be treated compared with those who reported less severe symptoms [7]. In our study, about half of the surgeries were performed during the initial 6 months, which is in line with previous studies.
Parsons et al. [11] reported that when community-dwelling older men having American Urological Association Symptom Index 8 or greater were followed up for 2 years, 4% underwent BPH surgery and 13% started new prescription medication. In the Proscar Long-Term Efficacy and Safety Study, 5% of finasteride-treated patients and 10% of placebotreated patients with moderate-to-severe symptoms with an enlarged prostate underwent BPH surgery during the 4-year follow-up period [16]. Our study included 3-year followup data, and the reported surgery rate was lower compared to that in studies of symptomatic patients. In the Urologic Diseases in America Project, 87,400 prostatectomies for BPH were performed among 8 million visitors who visited urology clinics with a primary or secondary diagnosis of BPH. Our result was 2%, which was higher than this previous result.
As our study was longitudinal, it demonstrated the timing of surgeries during the 3 years of follow-up in a population-based cohort. Alpha-blockers were the most common single category of medication prescribed, and this was concordant with previous studies in Korea [1718]. A certain portion of patients continued medication after BPH surgery. As Han et al. [19] showed that older age, the presence of comorbidities, and preoperative anticholinergic usage could be associated with the continuation of medication after TURP. Although detailed clinical information regarding the voiding status and the size of prostates could not be identified from this data, it is still meaningful considering the scarcity of nationwide data containing information on both prescriptions and surgical treatment.
Persistent LUTS can be a problem after transurethral prostatectomy necessitating medications [2021]. Detrusor underactivity or detrusor overactivity is contributable for this, and is considered to be one of important factors affecting the prognosis after transurethral prostatectomy in patients with BPH. About one third of patients have detrusor overactivity after TURP or PVP [2223]. Detrusor underactivity was not changed by the surgery whereas detrusor overactivity was significantly decreased after the surgery [22]. In our study, medication rate was lower than those inferenced from the literature. Because medication free rate was calculated only for those who were taking medications preoperatively during one month before the surgery, the actual postoperative medication rate can be different from our result.
There are a few limitations of the present study that must be discussed. The database did not include clinical variables; and the diagnosis of BPH was based only on the physician's opinion. The incidence of LUTS may have been underestimated because only patients who had visited the clinic were included in the analysis. In addition, medical management can be underestimated because we assigned the patient's status as surgery if he underwent surgery during that period. Third, the incidence of surgery might be underestimated because we have excluded those diagnosed with acute urinary retention. Lastly, we could not analyze the clinical predictors for surgery and medication as this data lack clinical variables.
CONCLUSIONS
The incidence of LUTS/BPH increases with age until the 7th decade of life. Older patients tend to be medically or surgically managed. About 1/5 of patients were taking medications for more than a year and 2.1% of patients were treated surgically. More than 80% of patients discontinued medications after the surgery, while patients having anticholinergics preoperatively are less likely to. Future studies with clinical variables will be helpful.





 XML Download
XML Download