

 PDF
PDF Citation
Citation Print
Print



Introduction
Postoperative pain control is essential for fast functional recovery through early rehabilitation, early return to daily life, and the welfare of patients after orthopedic limb surgery. Compared with intravenous patient-controlled analgesia (PCA), patient-controlled epidural analgesia (PCEA) enables effective pain control, fast intestinal motility recovery, and shortened hospital stay [1]. However, PCEA may result in several side effects due to the combined use of both local anesthetic and opioids [234]. Among the side effects, postoperative nausea and vomiting (PONV) occurs frequently and has a major negative impact on patient satisfaction. PONV can be caused by either the surgery or the anesthesia itself, but it can also be caused by the opioid contained in the PCEA [235].
Dexamethasone is known to reduce the incidences of PONV in children and adults [6]. Tarantino et al. [7] reported that the use of dexamethasone is effective in reducing nausea and vomiting by 28% after thyroidectomy. It was also effective in preventing nausea and vomiting associated with epidural opioid in patients undergoing open gynecologic surgery [4]. However, the use of dexamethasone may result in a reduction in glycemic control capability, increased wound infection or delayed wound healing, gastritis, and avascular necrosis [8].
Serotonin 5-hydroxytryptamine type 3 (5-HT3) receptor antagonists have been commonly used to prevent chemotherapy-induced nausea and vomiting, as well as PONV [910]. Compared with older 5-HT3 receptor antagonists, palonosetron has been widely used in recent years because of its advantages such as no QTc prolongation and longer half-life. However, there is little information about the use of palonosetron as prophylaxis against nausea and vomiting induced by PCEA containing opioids.
Therefore, the purpose of this study was to compare the effects of palonosetron and dexamethasone on PONV in patients undergoing total joint arthroplasty and receiving PCEA. The primary outcome was the overall incidence of PONV during the first 48 h postoperatively. Secondary outcomes were the incidence of PONV at 2, 24, and 48 h, the severity of nausea, use of rescue anti-emetics, pain scores, and side effects.
Materials and Methods
Institutional Review Board approval and written informed consent were obtained for this randomized, double-blind study. A total of 100 patients aged 20 to 80 years with an American Society of Anesthesiologists physical status of 1 to 3 who were scheduled to undergo total hip or knee arthroplasty and who wished to receive PCEA for postoperative pain control were recruited. Exclusion criteria were contraindication to regional anesthesia (coagulation disorders and infection at the injection site), pregnancy, administration of anti-emetics or steroids within 24 h before surgery, liver or kidney disease, neuropsychiatric disorders, and hypersensitivity to local anesthetic.
Using a computer-generated sequence of random numbers and sealed envelopes, patients were assigned to either the palonosetron group (group P) or dexamethasone group (group D). All envelopes were opened after induction of anesthesia by an attending nurse who was not involved in the study. The patients, anesthesiologists who performed the blocks, surgeons, and research assistants collecting outcome data were blinded to group allocation.
After arriving at the operating room, the patients were monitored continuously for blood pressure, heart rate, electrocardiogram, and peripheral oxygen saturation. Before induction, the patients received glycopyrrolate 0.2 mg and midazolam 2 mg intravenously.
In both groups, patients received combined spinal–epidural anesthesia with subarachnoid administration of 8 mg of 0.5% hyperbaric bupivacaine at the L3–4 or L4–5 intervertebral space with the patient in the lateral decubitus position. Then, using an 18 G Tuohy needle, the epidural space was confirmed by the method of loss of resistance using 1.5–2 ml air at the same level. A catheter was passed cephalad 3 cm past the needle tip and fixed after checking that no blood or cerebrospinal fluid was aspirated. Sensory blockade was targeted for over T12 and it was tested by a pin-prick test every 5 minutes for up to 15 minutes after the injection. If the sensory block was insufficient, 5 ml of 0.75% ropivacaine was injected through the epidural catheter as supplementation.
Patients were treated with prophylactic antibiotics 30 min before the beginning of the surgery. The study drugs (palonosetron 0.075 mg for group P and dexamethasone 5 mg for group D, respectively) were administered to the patients in each group prior to the injection of prophylactic antibiotics. The study drug for injection was prepared as 1 ml of clear solution in identical syringes.
Supplemental oxygen was administered throughout the procedure at 6 L/min through a mask. All the patients received an intravenous infusion of dexmedetomidine (loading dose of 0.1 µg/kg/min over 10 min followed by 0.008 µg/kg/min) for sedation throughout the procedure. Doses were adjusted to maintain a bispectral index value between 60 and 70. If the value fell more than 20% compared with the baseline blood pressure, ephedrine 10 mg was given. Every 60 min after the start of surgery, 5 ml of 0.75% ropivacaine was injected through the epidural catheter. On arrival at the postanesthesia care unit, an infusion of 0.2% ropivacaine (100 ml in total) and 1 µg/ml sufentanil (100 ml in total) was started and continued for 48 h (2 ml/h basal; 0.5 ml bolus; 15 min lockout) using an elastomeric infusion pump (Anaplus®, EWHA Meditech, Goyang, Korea).
The incidence of PONV (nausea, retching, and vomiting) and severity of nausea were recorded by direct questioning by research assistants blinded to the study group or recorded by the patients at the time points of 2, 24, and 48 h in reference to symptom occurrence during the prior observation period. Nausea was defined as the subjectively unpleasant sensation associated with awareness of the urge to vomit regardless of its severity. For the purpose of data collection, vomiting included retching (an involuntary attempt to vomit but without expulsion of gastric content) and vomiting (expulsion of gastric content). If nausea or vomiting was documented at any of these time points, it was considered PONV. The severity of nausea was rated from 0 (no nausea) to 10 (worst possible nausea). Rescue anti-emetics (ondansetron 4 mg) were given for PONV upon patient's request or complaint of nausea (severity of nausea ≥ 4) or vomiting and the number of injections was noted. Postoperative pain was assessed using a numerical rating scale (NRS, 0 = no pain; 10 = worst imaginable pain) at 2, 24, and 48 h after surgery. Rescue analgesia with 25 mg of intravenous meperidine to a maximum of 75 mg/24 h was available on demand. Other adverse effects, such as headache, dizziness, drowsiness, pruritus, constipation, wound infection or delayed wound healing, paresthesia, and motor weakness were also recorded.
Statistical analysis
SPSS version 19 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Normality of the data was tested using the Kolmogorov–Smirnov test. Normally distributed continuous variables were presented as means and SD and analyzed using Student's t-test. Non-normally distributed data were presented as median with 25th and 75th percentiles and analyzed using the Mann–Whitney U test. Categorical variables were defined as the number of patients (%) and analyzed using the Chi-square test or Fisher's exact test, as appropriate. A P value < 0.05 was considered statistically significant. Bonferroni correction for multiple repeated measurements was used for analysis of incidence of PONV at any time point, severity of nausea, and pain scores. In this case, a P value < 0.017 (= 0.05/3) was considered significant.
Sample size calculation was based on a previous study, which observed a 40% incidence of PONV in the dexamethasone group after surgery [11]. Assuming a 10% incidence of PONV in the palonosetron group, it was estimated that the sample size should be 40 patients per group using α = 0.05 and β = 0.1 for a two-sided test of difference. We enrolled 50 patients per group to allow for possible dropouts.
Results
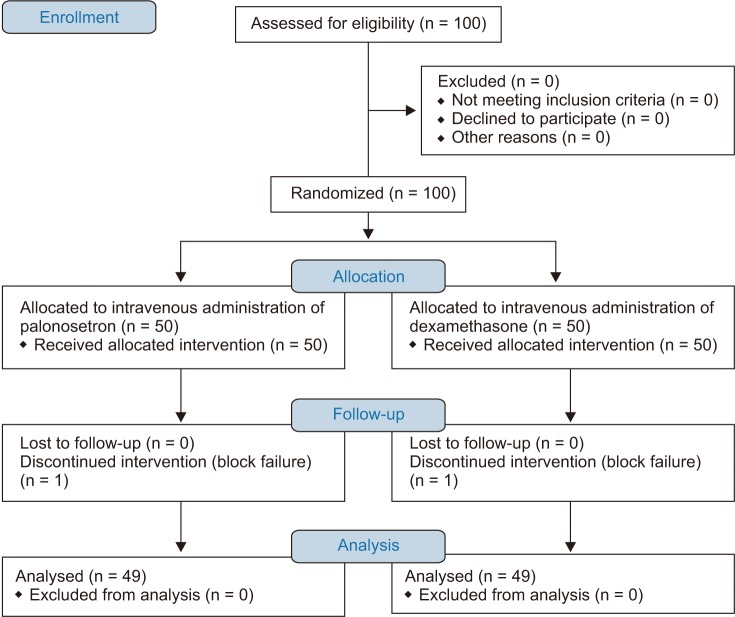
One hundred patients were enrolled in this study. One patient from each group was excluded because of a technical failure of spinal or epidural block. A total of 98 patients were included in the study (Fig. 1). Patient characteristics, Apfel risk score, type of surgery, and duration of the operation were comparable in both groups (Table 1).
The total incidence of PONV was significantly lower in the group P than group D (18.4% vs. 36.7%, P = 0.042, Table 2). However, there were no statistically significant differences in both groups during the 0–2 h, 2–24 h, and 24–48 h periods (Table 2). The severity of postoperative nausea was not significantly different between the two groups at all time intervals after surgery (Table 3). The numbers of patients requiring rescue anti-emetics were not significantly different between the groups (P = 0.372, Table 3).
There was no statistically significant difference in postoperative pain during the study periods (Table 3). In addition, supplemental meperidine consumption was similar between both groups (P = 0.176, Table 3). One patient in each group complained dizziness. There were no significant differences between the two groups considering potential adverse effects.
Discussion
This study demonstrated that palonosetron resulted in a lower total incidence of PONV than dexamethasone in patients receiving PCEA after hip or knee replacement surgery. However, there were no differences in the incidence of PONV at any time point, severity of nausea, use of rescue anti-emetics, pain score, and adverse effects.
PONV is one of a major contributing factor that negatively influences patient satisfaction after surgery. Although a contributor to PONV has not been clearly proven till now, various factors are implicated. The reported risk factors are female sex, history of PONV or motion sickness, non-smokers, young age, general anesthesia, the use of volatile anesthetics and nitrous oxide, opioids, duration of anesthesia, and type of surgery [12]. The mechanism of opioids-induced nausea and vomiting could be explained by several factors, including the increased sensitivity of the vestibular system, direct impact on the chemoreceptor trigger zone, and delayed gastric emptying [13]. Therefore, a necessary drug to prevent such a risk has to be co-administered because PCEA that include opioids may result in an increased risk of PONV.
In this study, the total incidence of PONV was lower in group P than in group D. However, the incidence of PONV at each time period and severity of nausea were not significantly different between the groups. The exact reason for these results is not clear, but it may be explained by a lack of power due to the small sample size in this study.
Dexamethasone is an inexpensive and effective anti-emetic that has been widely used as the drug of choice to prevent chemotherapy-induced nausea and vomiting, as well as PONV that occurs after general anesthesia [6]. In addition, dexamethasone is known to be effective in the prevention of PONV caused by epidural opioid administration for postoperative pain [14]. Although the antiemetic mechanism of dexamethasone is not yet clearly known, it is proposed to be the depletion of GABA (r-aminobutyric acid) storage, decrease in toxins associated with vomiting permeating through the blood brain barrier, inhibition of encephalin release from the brainstem, and synthesis and suppression of release of central serotonin [14]. Lee et al. [15] reported that the minimum effective dose of dexamethasone for the prevention of PONV associated with intravenous PCA containing morphine was 8 mg. Wang et al. [16] evaluated the antiemetic effects of various doses of dexamethasone and recommended 5 mg of dexamethasone as the minimum effective dose for prophylaxis against epidural morphine-related nausea and vomiting in parturients. However, a high dose or long-term use of dexamethasone may cause side effects such as glucose intolerance, wound infection, and delayed wound healing [48]. Therefore, it is necessary to use the minimum effective dose for preventing nausea and vomiting after surgery, and in this study, 5 mg of dexamethasone was chosen.
The serotonin 5-HT3 receptor antagonist has an antiemetic effect through its competitive binding to the 5-HT3 receptor. Palonosetron is the newest 5-HT3 receptor antagonist, with a greater receptor binding affinity than the older 5-HT3 receptor antagonists and a longer half-life of 40 hours. A recent study [17] showed that a single dose of palonosetron 0.075 mg reduced the incidence of PONV during the first 72 h after surgery. It was more effective in the prevention of PONV than older 5-HT3 receptor antagonists [18]. Furthermore, combination treatment using palonosetron and dexamethasone was more effective in the prevention of PONV compared with dexamethasone only in patients receiving IV PCA after general anesthesia [10]. A recent study reported that palonosetron was more effective in the prevention of PONV than ramosetron after cesarean section under spinal anesthesia [19]. A previous study evaluated older 5-HT3 antagonists for the prophylaxis of PONV in patients receiving PCEA containing an opioid after total knee arthroplasty [20]. Compared with ondansetron, ramosetron was more effective in preventing PONV associated with PCEA. However, few studies have compared palonosetron with dexamethasone in preventing nausea and vomiting associated with continuous administration of epidural opioid.
In this study, there were no differences in pain scores and consumption of supplemental analgesics between the two groups. A previous study reported that the 5-HT3 receptor is involved in the modulation of nociceptive transmission [21]. Lee et al. [22] reported that the pain score in the palonosetron group was lower than that of the control group. In addition, in a previous study on the effects of dexamethasone on pain, administration of dexamethasone resulted in reduced pain score, length of hospital stay, and opioid consumption compared with control after total knee arthroplasty [23]. Conversely, there were no statistically significant differences in the pain scores between dexamethasone and control groups of patients undergoing cesarean section after the administration of epidural morphine [16].
Consistent with previous studies, there were no adverse effects observed in this study, such as dizziness, drowsiness, constipation, headache, and wound infection [101416]. The long-term use of corticosteroids was associated with several side effects, such as increased risk of infection, glucose intolerance, delayed wound healing, superficial ulceration of gastric mucosa, and adrenal suppression, but no hazards were shown with a single dose [16]. Allen et al. [14] reported that there were no side effects, such as delayed wound healing, wound infection, and restlessness, when 2.5–10 mg dexamethasone was administered to parturients receiving epidural morphine. Headache and dizziness are the most common side effects of the 5–HT3 receptor antagonist. However, a previous study reported that there was not significantly difference in the incidence of side effects between the palonosetron and placebo groups [17].
This study has some limitations. First, although we compared two different anti-emetics, combination anti-emetic therapy is recommended for patients at moderate or high risk of PONV [12]. Second, we used ondansetron as rescue anti-emetics in this study. Since it is also a 5-HT3 receptor antagonist, an antiemetic with a different mechanism is more desirable. Third, midazolam and dexmedetomidine were administered to achieve intravenous sedation of patients during sensory block and surgery, respectively. These drugs have an anti-emetic effect [2425]. Fourth, we did not include a placebo control group to evaluate the baseline incidence of PONV. However, it is unethical to withhold anti-emetics in patients at high risk of PONV. Finally, patient satisfaction was not included as an outcome variable in this study. It is an important patient-reported endpoint.
In conclusion, this study demonstrated that intravenous palonosetron reduced the total incidence of PONV in orthopedic patients receiving PCEA compared with dexamethasone.
 XML Download
XML Download