

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Selenium (Se) is an integral component of selenocysteine, a major structural amino-acid of selenoproteins [1]. In addition to its anti-oxidant and anti-inflammatory effects, Se is also involved in the synthesis of DNA and thyroid hormone [1]. The cytoprotective properties of selenoproteins have garnered much interest leading to the discovery of selenoenzymes such as glutathione peroxidase (GPx), thioredoxin reductase (TrxR), and iodothyronine deiodinases (IDDs) [2]. GPx, which is one of the most well-studied selenoprotein family members, functions as a part of a defense mechanism to protect polyunsaturated fatty acids from the damaging effects of free radicals and inhibits the production of proinflammatory cytokines, reactive oxygen species, and reactive nitrogen species [3].
Due to the anti-oxidative and anti-inflammatory properties of Se, numerous studies have assessed the relationship between Se levels and conditions commonly known to be associated with increased oxidative stress and inflammation such as cardiovascular and neurodegenerative diseases, diabetes mellitus (DM), and cancer [456]. The association between Se and DM is one of the most vigorously investigated [78]. Studies have mainly been conducted based on the assumption that Se may be protective against DM [9]. Oxidative stress and inflammation have been reported to be involved in the onset and progression of diabetes [1011]. Consistent with these findings, supplementation of antioxidants including Se has been shown to delay the onset of DM [6]. Moreover, data from isolated rat adipocytes show that Se in the form of selenate can act as an insulin mimetic [1213]. Several cell and animal studies have suggested that Se plays a crucial role in controlling glucose homeostasis [14151617]. Moreover, epidemiological studies have evaluated the effects of Se on DM, but the conclusions have been conflicting [181920212223]. Some studies report that Se is positively associated with DM [181920] while others indicate a negative or no association [212223]. Although there has been a meta-analysis including five observational studies [7], many additional studies have been published since then [18192425]. Hence, an updated meta-analysis to review the recent data is warranted to understand better and clarify the role of Se in DM. Therefore, we performed an updated meta-analysis by a comprehensive investigation of the literature with conflicting conclusions.
METHODS
Search strategy
The literature search was performed in accordance with the general principles recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Supplementary Table 1). Two independent investigators (S.M. and J.K.) searched the PubMed and Embase databases and selected articles using a combination of terms “diabetes mellitus” and “selenium.” Only articles published in English, before June 30, 2018, were included.
Study selection
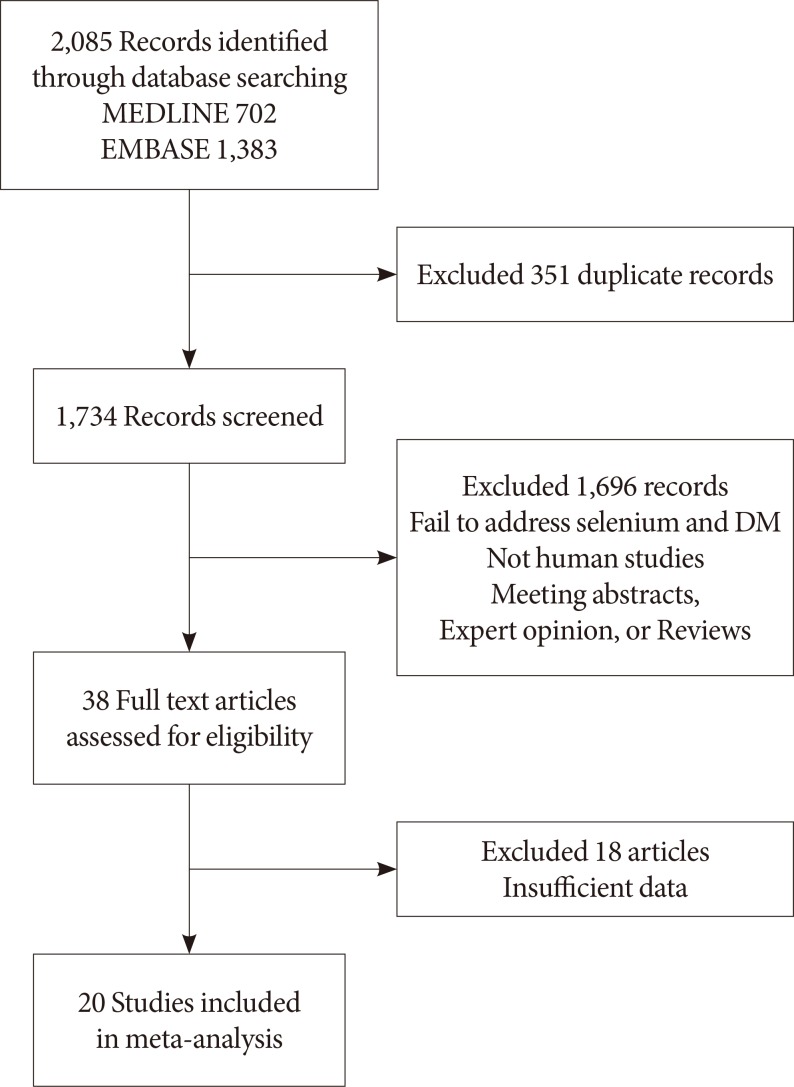
The literature search yielded 2,085 potentially relevant articles, of which 1,734 were screened for further review after excluding duplicate studies. If studies had multiple reports, the latest or the complete article was enrolled. All articles were electronically downloaded and screened for inclusion using a two-step method. After evaluation of the titles and abstracts according to predefined criteria, 1,696 articles were excluded if: (1) the studies had a different topic of interest; (2) there was no information on Se and DM; or (3) the study was published as an abstract, expert opinion, conference article, or review. Subsequently, the full texts of 38 selected articles were reviewed by two independent investigators (S.M. and J.K.), and any disagreement was resolved by a third investigator (J.M.Y.). A total of 20 articles were finally selected for the meta-analysis (Fig. 1).
Assessment of bias risk
Three researchers independently assessed the methodological quality of the included articles using the Newcastle-Ottawa Scale (NOS) for case control studies [26]. Nine items were used to assess the quality, and all articles scored 6 to 8 (Supplementary Table 2). We concluded that the quality of these cross-sectional studies did not affect the quality of our meta-analysis.
Data extraction
The following variables were independently extracted by the two investigators based on the same rules: first author, publication year, country, number of study participants, mean age, number of men and women, characteristics of study participants including coexisting diseases, the mean or median concentration of Se, and number of DM.
Data analyses and statistical methods
We calculated the pooled odds ratio (OR) with 95% confidence intervals (CIs) for the highest and lowest quantiles of Se using the Mantel-Haenszel method. The Higgins' I2 statistic was used to test for heterogeneity. When I2 was ≤50%, the included studies were considered to have little heterogeneity, and a fixed-effects model was used. However, I2 >50% indicated heterogeneity and a random-effects model was used. Subgroup and sensitivity analyses were used to determine the cause of heterogeneity. The potential for publication bias was assessed by funnel plot analysis. To examine the strength of the outcome, we conducted a sensitivity analysis to estimate the effects of the remaining studies without the larger one. All statistical analyses were calculated using the statistical program R (R version 3.1.0, 2014, www.r-project.org).
RESULTS
Characteristics of selected studies
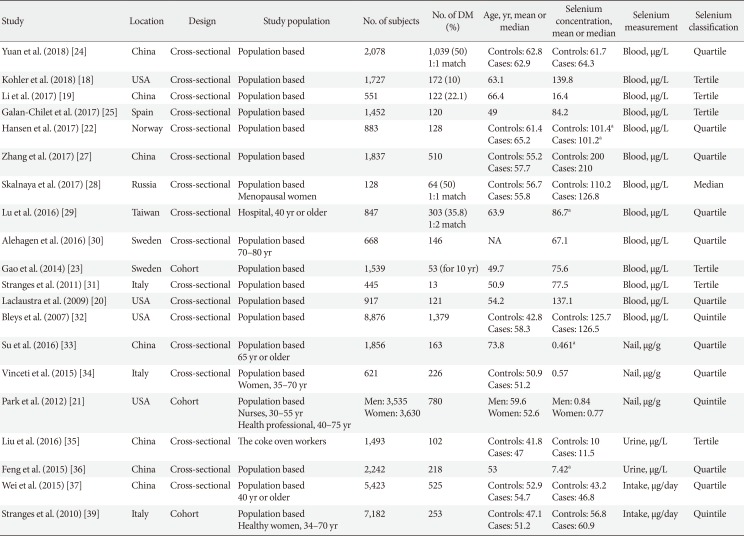
Twenty articles were included in the meta-analysis [1819202122232425272829303132333435363738], and their main characteristics are summarized in Table 1. In total, 47,930 participants were enrolled, and 6,347 of them had DM. Sample sizes of these studies ranged from 128 to 8,876 participants. In these studies, Se concentrations were measured in the blood (n=13), nails (n=3), and urine (n=2). Two studies estimated Se intake from a food diary survey.
Se and DM
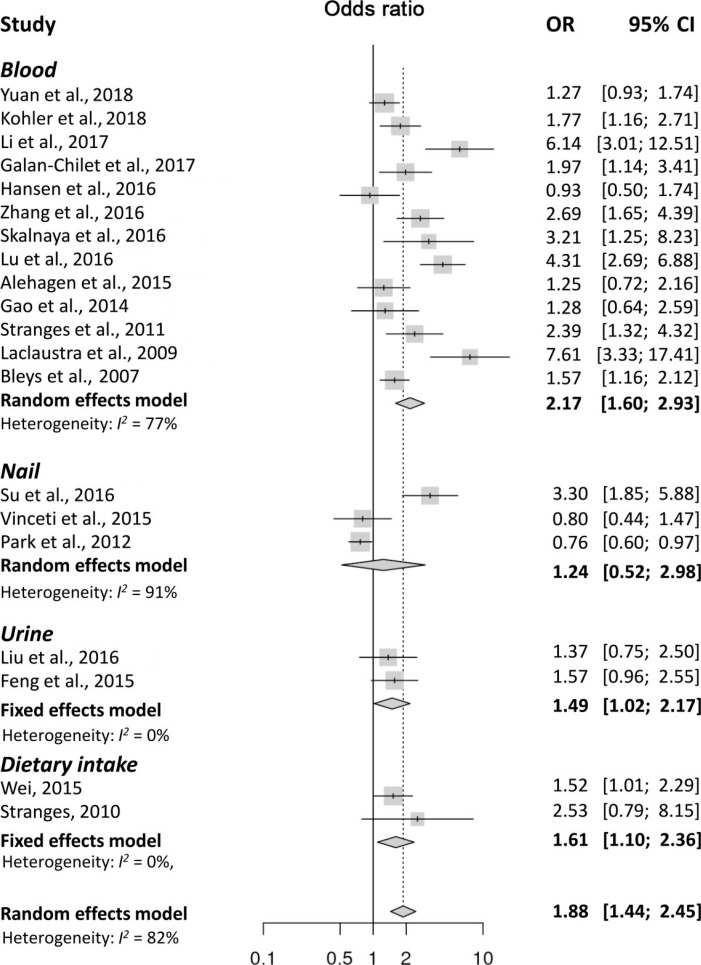
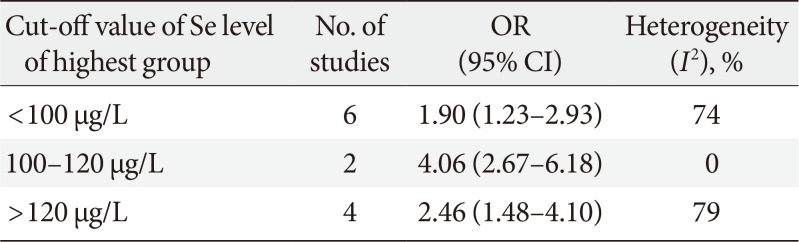
The meta-analysis found that high levels of Se were significantly associated with the presence of DM (OR, 1.88; 95% CI, 1.44 to 2.45). However, there was significant heterogeneity (I2=82%) (Fig. 2), and the funnel plot analysis showed significant publication bias (Supplementary Fig. 1). In the sensitivity analysis, the pooled OR changed little after omitting each study (Supplementary Fig. 2), and the heterogeneity ranged from 1.99 to 2.31, remaining statistically significant. A subgroup analysis based on the methods used for Se measurements, showed a significant association between high Se levels and DM in the studies on blood (OR, 2.17; 95% CI, 1.60 to 2.93; I2=77%), dietary intake (OR, 1.61; 95% CI, 1.10 to 2.36; I2=0%), and urine (OR, 1.49; 95% CI, 1.02 to 2.17; I2=0%). However, studies on Se in the nails failed to show a significant association with DM (OR, 1.24; 95% CI, 0.52 to 2.98; I2=91%). Because a significant heterogeneity was found in studies with blood, we conducted a sensitivity analysis and tested the publication bias. Sensitivity analysis found three outlier studies [343536]. After omitting these studies, the estimated pooled OR was 1.64 (95% CI, 1.34 to 2.02) with no significant heterogeneity (I2=40.3%). Since the funnel plot was asymmetric, publication bias was adjusted using the trim-and fill method by adding two estimated missing studies, which produced significant results (OR, 1.82; 95% CI, 1.31 to 2.53). Because of the heterogeneity in Se levels in each study, we conducted a subgroup analysis based on the mean or median blood Se levels, using 100 µg/L as the cut-off value. The pooled OR was 2.17 (95% CI, 1.37 to 3.44; I2=82%) in studies with mean Se <100 µg/L and 2.17 (95% CI, 1.40 to 3.39; I2=76%) in studies with mean Se ≥100 µg/L. A meta-regression analysis showed no significant effects of the mean Se levels (P=0.91) (Supplementary Fig. 3). The subgroup analysis using cut-off levels of Se of the highest group showed similar results (Table 2).
DISCUSSION
This meta-analysis of 20 observational studies showed that higher concentrations of Se were significantly associated with the presence of DM. Although significant heterogeneity was detected, the results did not change after adjustment by subgroup analysis, sensitivity analysis, and trim and fill analysis for publication bias.
DM is characterized by peripheral insulin resistance, with defects in insulin-secretion, which can be of varying degrees of severity. Although the mechanisms that underlie insulin resistance and diabetes are not fully understood, several studies point to the role of oxidative stress in the onset and progression of DM [10]. Therefore, Se which has been long touted for its antioxidant properties was believed to prevent the onset of DM by counteracting oxidative stress [9]. Although earlier studies have shown the insulin-mimetic and anti-diabetic effects of Se [1639], recent experimental studies have revealed an unexpected association between high Se intake and insulin resistance or DM [4041424344]. High Se exposure led to insulin resistance in rodents and pigs [45]. Although the mechanism underlying the diabetogenic effects of Se remains unclear, the high Se exposure might affect the expression of key regulators of glycolysis and gluconeogenesis. This action might potentially be mediated by the selenoprotein GPx-1 [45], as demonstrated by studies showing that overexpression of GPx-1 causes insulin resistance [46]. In skeletal muscles of pigs, high Se exposure led to an increase in GPx activity and expression of both forkhead box O1 and peroxisomal proliferator-activated receptor-γ coactivator 1α genes. It also led to a decrease in the expression of the gene for the glycolytic enzyme pyruvate kinase [44].
A number of human studies have been conducted to evaluate the effects of Se on DM, but the conclusions have been inconsistent. Although previous meta-analyses showed a modest association between Se and DM, they included only five observational studies [7]. Therefore, this meta-analysis is noteworthy since it demonstrates an association between Se and the presence of DM based on a number of observational studies in large populations, providing significant epidemiological evidence to support the results of previous experimental studies.
Although our findings suggest that there is a significant association between increased exposure to Se and DM, data from clinical trials of Se supplementation have not been conclusive. The first large randomized trial was the Nutritional Prevention of Cancer (NPC) Trial, in which 200 µg Se per day or a matched placebo was administered to evaluate whether it could reduce the risk of non-melanoma skin cancer. Stranges et al. [47] performed the secondary analyses with the NPC data and showed an increased risk of DM among those in the Se intervention group compared to those in the placebo group. In contrast to the NPC trial, the Se and Vitamin E Cancer Prevention Trial (SELECT), the largest prostate cancer prevention trial with 35,533 participants showed no significant increase in the risk for DM after supplementation with 200 µg/day of Se compared to placebo [48]. However, in a subgroup analysis with the elderly aged >63 years, a significantly increased risk for DM was reported [49]. Mao et al. [8] on the other hand, showed no association between Se supplementation (200 µg/day) and the risk for DM in their meta-analysis with four randomized controlled trial studies.
The considerable strengths of this study are that a number of observational studies with large populations were included, and predefined subgroup analyses could be performed. However, the present study has some limitations. First, since most of the included studies were cross-sectional studies, further prospective studies will be needed to clarify the relationship between Se and the risk for DM. Second, the differences in age, sex ratio and Se concentrations between different studies could induce a bias. In addition, the different methods used for measuring Se levels could also have contributed to the bias. Third, because we compared the highest quantile of Se to the lowest quantile in each study, there might be great heterogeneity among the cases and control groups between different studies.
In conclusion, this meta-analysis demonstrates that high levels of Se are associated with the presence of DM. Although the mechanism remains unclear, our findings could have implications for nutritional supplementation in clinical settings. Further prospective and randomized controlled trials are warranted to elucidate the link between Se and DM better.
 XML Download
XML Download