

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Metabolic syndrome is considered one of the most serious health problems worldwide due to its high prevalence and cardiovascular consequences [123]. The current criteria for the diagnosis of metabolic syndrome consist of five components (increase in waist circumference, triglyceride [TG] level, blood pressure, and fasting glucose level and decrease in high density lipoprotein cholesterol [HDL-C] level) [4], where each component is considered as a marker of different diseases, such as obesity, hyperlipidemia, hypertension, type 2 diabetes mellitus, and dyslipidemia. During the pre-clinical stages, the prediction of and early interventions for metabolic syndrome is important. Metabolic stress due to nutrition excess may induce endoplasmic reticulum, oxidative, and mitochondrial stresses [5]. All these stresses play detrimental roles via positive feedback, which ultimately leads to obesity, insulin resistance, and type 2 diabetes mellitus [56789]. Therefore, humoral factors released from the liver, adipose tissue, or muscle due to metabolic stress could be a possible predictive serum marker of incident metabolic syndrome.
Angiopoietin-like 6 (ANGPTL6) promotes angiogenesis [10] and epidermal proliferation [11]. ANGPTL6 is a hepatokine that remains as an orphan ligand, which does not bind to the angiopoietin receptors. Recent studies have shown that ANGPTL6 has a beneficial effect on the metabolism. ANGPTL6-deficient mice showed marked obesity and insulin resistance with attenuated systemic energy expenditure even when fed a normal diet [12]. Conversely, a mouse model with a gain-of-function of ANGPTL6 was protected from diet-induced obesity with enhanced insulin sensitivity and energy expenditure. ANGPTL6 increased the capillary density in the muscle tissue [12] and suppressed gluconeogenesis in the hepatocytes [13]. Based on these findings, ANGPTL6 has been introduced as a novel therapeutic target against obesity and type 2 diabetes mellitus [14].
Recently, the serum ANGPTL6 levels of healthy individuals and patients with different metabolic diseases were assessed. Intriguingly, the serum ANGPTL6 levels were high in individuals who diagnosed with preeclampsia [15], polycystic ovary syndrome [16], and type 2 diabetes mellitus [1718]. Moreover, the serum ANGPTL6 levels of patients with metabolic syndrome was high [19]. However, not all of the changes in the disease conditions are consistent with beneficial metabolic effects. Whether cross-sectional studies could be used to identify the chronological relationship between origin and outcome has not yet been determined. In other words, these paradoxical ANGPTL6 upregulations could be complex. They could denote a resistance to their own actions, a compensation to metabolic stress, simply a correlation-only phenomenon, or have different actions on human physiology.
To better understand the relationship between serum ANGPTL6 levels and new-onset metabolic syndrome, we conducted a prospective study on a rural cohort in Korea. We also investigated the predictive value of serum ANGPTL6 levels in participants who are at high risk of incident metabolic syndrome. Herein, we report that the serum ANGPTL6 levels were already elevated before developing new-onset metabolic syndrome. Moreover, serum ANGPTL6 levels could be an independent predictive marker of metabolic syndrome.
METHODS
Study participants
The study protocol was approved by the Institutional Review Board of Wonju Severance Christian Hospital (IRB No. CR-105024), and a written informed consent was obtained from all the participants. We used serum samples and data from the Korean Genome and Epidemiology Study on Atherosclerosis Risk of Rural Areas in the Korean General Population, which is a prospective cohort study on all adults aged 40 to 70 years living in the rural areas of Wonju and Pyeongchang [20]. We randomly selected 221 out of 5,178 participants who were not diagnosed with metabolic syndrome at baseline, and the details about the study participants were previously described [21]. We defined metabolic syndrome according to the harmonized definition [4] which is denoted by the presence of at least three of the following components: (1) abdominal obesity [22] (waist circumference ≥90 cm for male and ≥85 cm for female); (2) high TG level (≥150 mg/dL [1.69 mmol/L]); (3) low HDL-C level (<40 mg/dL [1.04 mmol/L] for male or <50 mg/dL [1.29 mmol/L] for female); (4) high blood pressure (systolic blood pressure ≥130 mm Hg, diastolic blood pressure ≥85 mm Hg, or intake of antihypertensive agents); and (5) high fasting glucose level (≥100 mg/dL or previous diagnosis of type 2 diabetes mellitus).
Data collection
The methods applied for anthropometric and biochemical measurements were carried out as previously described [20]. Briefly, the participants provided their medical history, completed a lifestyle questionnaire, and underwent a health examination. Muscle, body fat, and visceral fat contents were measured via bioelectrical impedance analysis using the InBody Body Composition Analyzer (InBody, Seoul, Korea). Venous blood samples were obtained to measure TG, HDL-C, low density lipoprotein cholesterol (LDL-C), glucose, insulin, glycosylated hemoglobin (HbA1c), aspartate transaminase, alanine transaminase, gamma-glutamyl transferase, and C-reactive protein (CRP) levels before and after the follow-up. The baseline serum ANGPTL6 levels were assessed with an enzyme-linked immunosorbent assay kit (Adipogen Life Science, San Diego, CA, USA) using serum aliquots stored at −80℃ according to manufacturer's instruction. The inter- and intra-assay coefficient of variation of ANGPTL6 measurement were 10.08% and 5.45%, respectively.
Statistical analysis
All analyses were performed using the IBM SPSS Statistics version 23 (IBM Corp., Armonk, NY, USA). P values <0.05 were considered statistically significant. To assess the independent associations between baseline ANGPTL6 levels and incident metabolic syndrome, multivariate logistic regression analyses using three models with progressive degrees of adjustment were performed. Analysis using the first model was conducted with adjustments for age, sex, and baseline number of metabolic syndrome components. Then, after adjusting for the baseline body mass index (BMI), LDL-C level, smoking status, and regular exercise, the second model was analyzed. Finally, we adjusted for the baseline homeostasis model assessment of insulin resistance (HOMA-IR) and CRP level. The results were expressed as odds ratios (ORs) with 95% confidence intervals (CIs). To evaluate the predictive value of ANGPTL6 on incident metabolic syndrome, the receiver operating characteristic (ROC) curves in the models of the components of metabolic syndrome with or without serum ANGPTL6 levels at baseline were plotted. Areas under the ROC curves were compared using the nonparametric method [23].
RESULTS
General characteristics of the study population
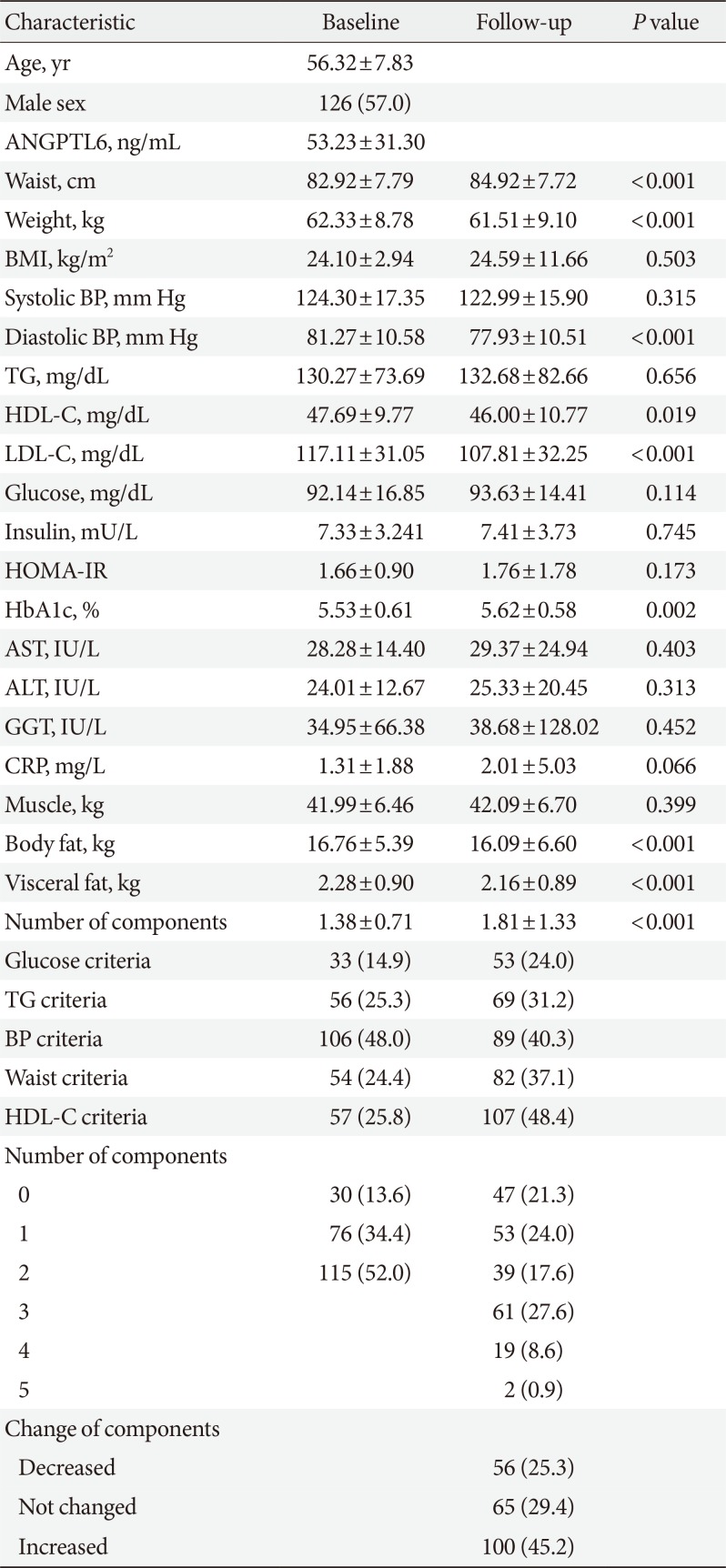
The general characteristics of the anthropometric and serum marker profiles of the study participants before and after the follow-up period are shown in Table 1. During an average follow-up period of 2.75 years (interquartile range, 0.76), waist circumference, HbA1c, and the number of metabolic syndrome components significantly increased, whereas weight, diastolic blood pressure, HDL-C level, LDL-C level, body fat mass, and visceral fat mass remarkably decreased. Over the follow-up period, 82 participants (37.1%) presented new-onset metabolic syndrome. In total, 100 participants (45.2%) presented an increased number of metabolic syndrome components, whereas 56 (25.3%) had a reduced number of components.
Baseline serum ANGPTL6 level and incident metabolic syndrome
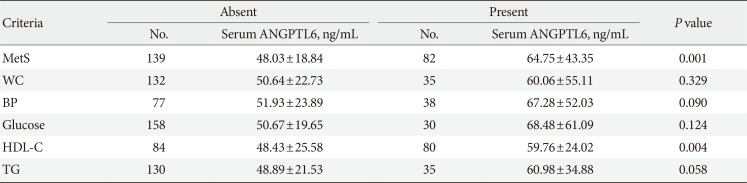
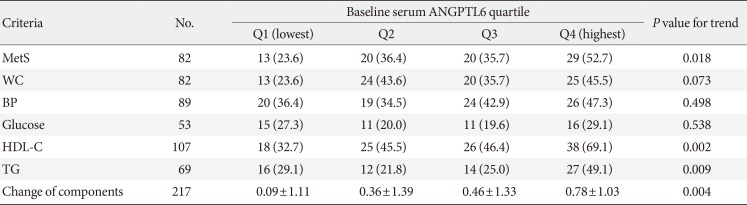
First, we checked whether the baseline serum ANGPTL6 levels were associated with new-onset metabolic syndrome. As shown in Table 2, the participants who developed metabolic syndrome after follow-up already had significantly elevated serum ANGPTL6 levels at baseline (48.03±18.84 ng/mL vs. 64.75±43.35 ng/mL, P=0.001). The participants who recently met the HDL criteria had higher baseline serum ANGPTL6 levels (48.43±25.58 ng/mL vs. 59.76±24.02 ng/mL, P=0.004). Next, the association between the changes in metabolic syndrome components and basal ANGPTL6 levels was analyzed. The participants with increased metabolic syndrome components during follow-up had elevated serum ANGPTL6 levels at baseline (P for trend=0.003) (Table 3). In the post hoc analysis, their ANGPTL6 levels (62.01±40.33 ng/mL) were significantly higher than those with a decreased or the same number of components (46.52±16.59 ng/mL, P=0.008 or 49.92±21.00 ng/mL, P=0.024, respectively). Similar to the participants with incident metabolic syndrome who had increased ANGPTL6 levels at baseline, those with higher basal ANGPTL6 levels showed more frequent onset of metabolic syndrome (P for trend=0.018) (Table 4), particularly based on the HDL and TG criteria (P for trend=0.002 and P for trend=0.009, respectively). During the follow-up, the participants with higher basal ANGPTL6 levels showed an increased number of metabolic syndrome components (P for trend=0.004).
Increased ANGPTL6 level as a predictive marker of metabolic syndrome
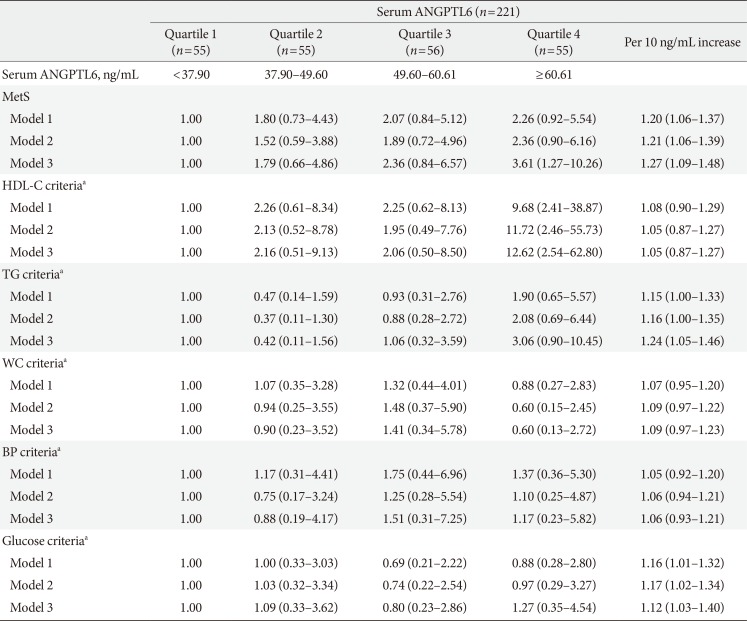
To validate whether ANGPTL6 levels can be used as a predictive factor of new-onset metabolic syndrome, multivariate regression models were used (Table 5). After adjusting for sex, age, baseline number of metabolic syndrome components, BMI, LDL-C level, smoking, regular exercise, HOMA-IR, and CRP level, the OR for developing metabolic syndrome in the highest ANGPTL6 level quartile along with those in the lowest was 3.61 (95% CI, 1.27 to 10.26; P=0.016). The OR for meeting the HDL criteria in the highest ANGPTL6 level quartile along with those in the lowest was 12.62 (95% CI, 2.54 to 62.80; P=0.002). When an analysis was conducted using ANGPTL6 concentrations (per 10 ng/mL increase) instead of quartiles, the participants with higher ANGPTL6 showed increased ORs for the new-onset metabolic syndrome (1.27; 95% CI, 1.09 to 1.48; P=0.002). Among the components, the ORs for the TG and glucose criteria were elevated ([1.24; 95% CI, 1.05 to 1.46; P=0.011] and [1.12; 95% CI, 1.03 to 1.40; P=0.018], respectively).
Additional predictive value of ANGPTL6 on the conventional criteria of metabolic syndrome
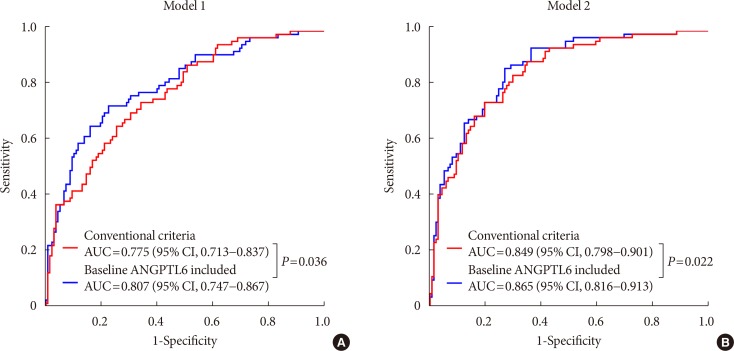
Finally, we checked whether the use of baseline ANGPTL6 levels in addition to the existing components of metabolic syndrome can predict incident metabolic syndrome more precisely (Fig. 1). When using the conventional criteria of metabolic syndrome (HDL-C level, TG level, waist circumference, blood pressure, and glucose levels), the area under the ROC curve for predicting new-onset metabolic syndrome was 0.775 (95% CI, 0.713 to 0.837; P<0.001). After the addition of serum ANGPTL6 levels, the corresponding area under the ROC curve was 0.807 (95% CI, 0.747 to 0.867; P<0.001). The P value for the comparison of the AUC for the models with and without ANGPTL6 was 0.036. When sex and age were normalized, the ANGPTL6 levels still had additional predictive values for metabolic syndrome (0.849 with a 95% CI of 0.798 to 0.901 vs. 0.865 with a 95% CI of 0.816 to 0.913, P=0.022).
DISCUSSION
With the increasing prevalence of obesity, metabolic syndrome is considered as pandemic [1]. Because of the increased risk of cardiovascular disease [2], an early diagnosis of metabolic syndrome during the pre-clinical stage may be useful for prediction and intervention. Several biomarkers, including adiponectin [20], leptin [24], and CRP [25] have been investigated, most of which are adipokines and to correlated with obesity. From an adipocentric point of view [26], increased adiposity is the initial event of metabolic dysregulations in the pathogenesis of metabolic syndrome. Because the Asian population experiences increased adiposity with the same BMI compared to Caucasians [2728], several studies have focused on adipokines as candidate biomarkers of metabolic syndrome. Low HDL-C level is a component of metabolic syndrome that is commonly observed in the Asian population, and is another unique characteristic of this group [293031]. Therefore, similar to adipokines, hepatokines could be good biomarker candidates for Asians. In this context, serum ANGPTL6 levels have a predictive value for the future onset of metabolic syndrome. The baseline serum ANGPTL6 levels were already higher in participants who later developed metabolic syndrome. Furthermore, increased ANGPTL6 levels were a strong predictor of low HDL-C and high TG levels, both of which are the most frequent components of metabolic syndrome in female and male in Korea, respectively [32], along with high blood glucose levels.
Previously, we reported that the serum ANGPTL6 levels were elevated in individuals with metabolic syndrome in a cross-sectional study [19]. In this prospective cohort study, we found that an increased ANGPTL6 level was observed prior to the onset of metabolic syndrome. It is worth noting that a previous study in mice showed increased obesity and insulin resistance in the knockout of ANGPTL6. Transgenic mice with ANGPTL6 overexpression presented a lean phenotype with a higher metabolic rate, indicating the beneficial effects of ANGPTL6 on metabolism [12]. The paradoxical upregulation of ANGPTL6 in studies on metabolic diseases in humans may originate either from compensatory responses to metabolic stress or resistance of ANGPTL6 signaling. However, ANGPTL6 resistance is less likely to occur because ANGPTL6 increases in the pre-clinical period of metabolic syndrome. Instead, we assume that ANGPTL6, as a beneficial hepatokine, is upregulated to mitigate metabolic stress, which is similar to the induction of fibroblast growth factor 21 (FGF21) against mitochondrial stress [33].
We found that elevated ANGPTL6 levels could be an independent predictor of metabolic syndrome. A compensatory increase in ANGPTL6 levels occurs after continuous metabolic stress before the onset of the disease. However, if stress overwhelms the capacity of compensation, the clinical manifestations and pathologic progression of metabolic syndrome are maintained despite the elevated ANGPTL6 levels. ANGPTL6 has a positive correlation to HOMA-IR and leptin [151719]. We recently published that synthesis and secretion of hepatic ANGPTL6 are upregulated in mice fed a high fat diet, which are regressed by regular exercise [34]. Both approaches validate our main hypothesis that increased ANGPTL6 is a defense mechanism to ameliorate metabolic stresses including obesity. A recent report showed elevated ANGPTL6 expression in the pharmacologic or genetic models of impaired mitochondrial oxidative phosphorylation [35]. However, ANGPTL6 remains an orphan ligand, and its receptor has not yet been identified. Therefore, further research must be conducted in order to understand the mechanism of ANGPTL6 regulation by metabolic stress and its pathophysiological implications.
Identifying metabolic stress could be useful for the prediction of the onset of or prognosis of metabolic diseases as well as the evaluation of therapeutic efficacy. We suggest that the serum levels of ANGPTL6 could be a surrogate target for the assessment of pathologic stresses. In terms of its compensatory actions, a specific level of ANGPTL6 may be beneficial to the metabolism. We hypothesized that there may be a J-shape association between ANGPTL6 levels and the ORs of metabolic syndrome, which is a characteristic feature of a hormetic response [36]. Previously, we reported that FGF21, which acts against metabolic stress similarly to ANGPTL6, showed a typical J-shape correlation to metabolic syndrome [21]. However, in this study, ANGPTL6 elicited a more complicated pattern; for example, the OR values of the TG criteria showed a J-shape correlation, whereas those of metabolic syndrome have a linear pattern correlation. This discrepancy could be caused by a small sample size and a relatively short follow-up period, which are the primary limitations of this study. In addition, we could not analyze the differences according to sex because of the small sample size, although female have higher levels of ANGPTL6 than male [19]. The blood sampling was performed at a single time point, which was subjected to variations according to the circadian rhythm of ANGPTL6. These may underestimate the correlation strength, which are indicated by significant 95% CI values and ORs shown in Table 5. Further investigations with a large sample size and a long-term follow-up may elucidate our hypothesis more clearly.
In conclusion, this first prospective cohort study revealed that serum ANGPTL6 levels can be a significant and independent predictive factor of the onset of incident metabolic syndrome and its components, particularly low HDL, high TG, and high glucose levels. This study supports the concept that the upregulation of ANGPTL6 is a compensatory mechanism against metabolic stress and is a candidate biomarker of metabolic syndrome. As ANGPTL6 significantly enhanced the predictive values of incident metabolic syndrome over the conventional components of current diagnosis, further studies may help develop an appropriate risk-scoring method for metabolic syndrome.

 XML Download
XML Download