

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Self-monitoring of blood glucose (SMBG) is a fundamental tool of diabetes management in especially multiple daily insulin injection-treated type 1 diabetes mellitus (T1DM) individuals. Intensive diabetes management in order to maintain optimal glycemic control was identified as reducing the development and progression of chronic complication in T1DM patients [123]. SMBG plays the numerous beneficial roles in predicting insulin demand, notifying hypoglycemia, providing stable glucose variability, etc.
Several studies have documented that higher frequency of daily SMBG are associated with lower glycosylated hemoglobin (HbA1c) levels in pediatric T1DM [45678910]. On the other hand, association studies were rare in particular ethnicities and geographic area like Asia with a low background incidence of T1DM. To date, no study has reported the association with SMBG measurement and HbA1c values among Korean adolescents with T1DM. Furthermore, it has been published that the mean HbA1c level in Korean pediatric T1DM is higher compared with those in Western Pacific and Asian countries [11]. During adolescence, diabetes care and glucose control become more difficult than the other-age group. Adolescents with T1DM have a tendency to lack of adherence to diabetes management and poor glycemic control [1213].
The aim of this study was to investigate the relationship of SMBG to glycemic control among Korean adolescents with T1DM. The factors affecting SMBG frequency were evaluated with a structured questionnaire in order to achieve their adequate glycemic control.
METHODS
Subjects
This study was conducted between March 2015 and February 2016 on adolescents with TIDM aged 13 to 18 years who visited at one tertiary hospital in Korea (n=73). The exclusion criteria were individuals with underlying disorders such as malignancy (n=1), chronic kidney disease (n=1), mental retardation (n=3), using real-time continuous glucose monitoring or flash glucose monitoring (n=1), and recent history of new-onset of T1DM (n=6) within the previous 1 year. The study was approved by the Institutional Review Board of Inha University Hospital (IUH-IRB 15-1454). Written informed consents were obtained from all participants and their legal guardians. All procedures were performed in accordance with the Declaration of Helsinki.
Methods
Total 61 subjects were enrolled for the study. This study was performed using a structured one-time questionnaire survey and a retrospective review of medical records. The questionnaires comprised of three categories about related factors to SMBG frequency were completed by individuals or their parents. Evaluated factors were included behaviors of diabetes self-care (e.g., the frequency and pattern of daily SMBG, whether the patient kept a blood glucose diary, and the individual's understanding about diabetes), family-related factors (e.g., family structure, parents' marital status, the main caregiver, a family history of diabetes, and family supports), and school-related factors (e.g., obstacles to measure of SMBG, the frequency and places of SMBG per day in the school setting during 6 months before enrollment). In addition, the questionnaire for school-related factors contained the following inquiry: Who has helped you to manage your illness? Who is aware of your illness? Who has informed others about your illness? Where have you been conducted SMBG at school?
The following data were obtained from the medical records: age, gender, height, weight, body mass index (BMI), duration of illness, HbA1c, C-peptide level, insulin regimen, total daily insulin dosage (TDD, dose/kg), presence of diabetes-related complications, and frequency of admission for poor metabolic control of T1DM. HbA1c levels were based on the results of the test at the time of survey.
Statistical methods
Descriptive statistics were indicated as the mean±standard deviation, or ratio. Comparisons of relevant factors between groups divided by the SMBG frequency were assessed by using the Student t-test or the chi-square test. The correlation between the SMBG frequency and HbA1c was analyzed using simple linear regression analysis. Multiple logistic regression analysis using the frequency of SMBG as a dummy variable was performed to assess achievement of the target HbA1c level (7.5%) according to daily frequency of SMBG and frequency in the school setting. The results were reported as the odds ratios (ORs) and 95% confidence intervals (CIs) with adjustment for variables. Multiple linear regression analysis was conducted to assess the association between school-related factors and SMBG testing performance in the school setting. The results were shown with regression coefficients, 95% CIs, and P values after adjusting for variables (diabetes mellitus [DM] family history, daily insulin dosage). IBM SPSS version 19 (IBM Co., Armonk, NY, USA) was used for statistical analysis.
RESULTS
Patient characteristics
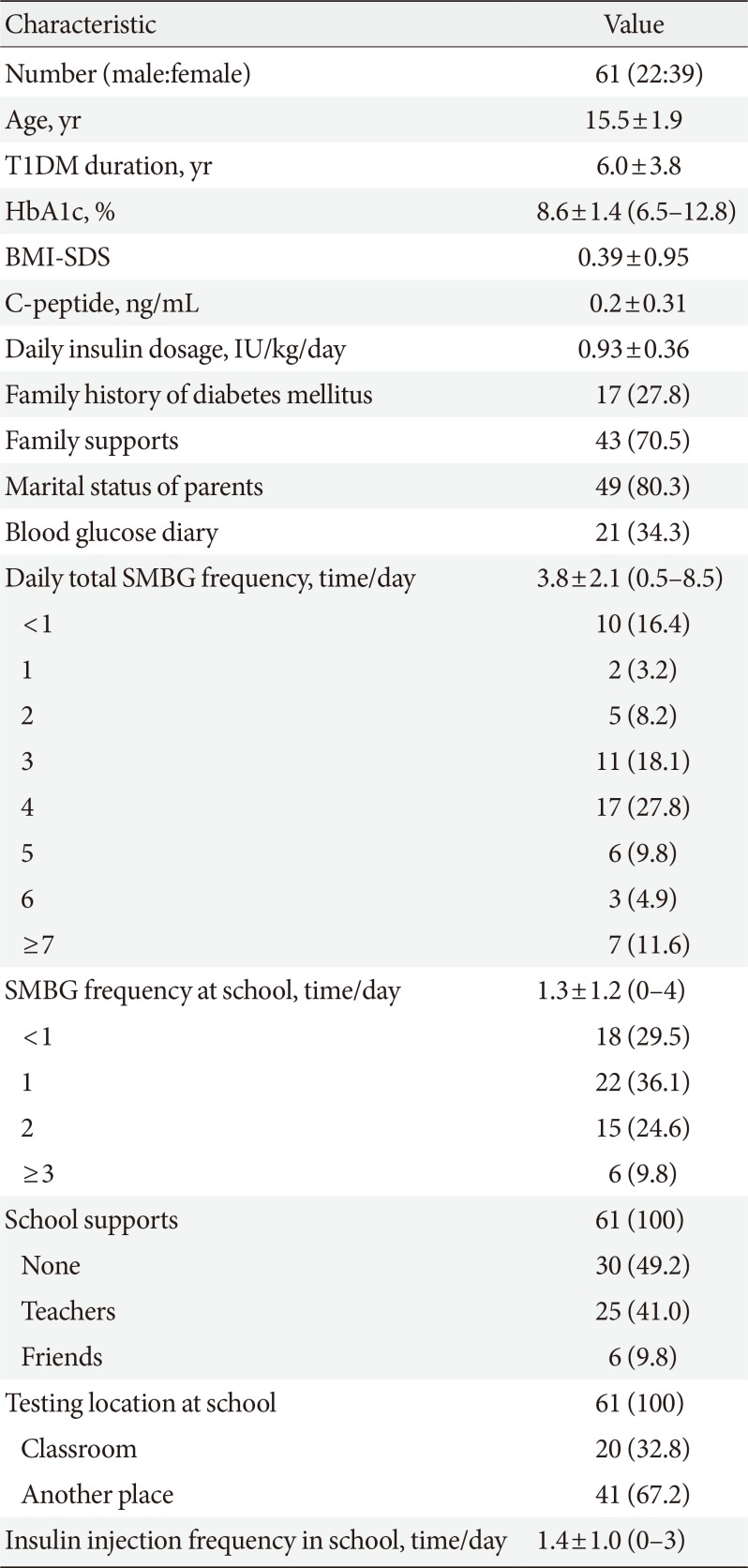
Of the 61 participants, 36% were male (n=22) and the mean age was 15.5±1.9 years. All subjects have received multiple daily insulin-injection regimens without insulin pump. There was no one using real-time continuous glucose monitoring or flash glucose monitoring. The mean diabetes duration was 6.0±3.8 years while the mean BMI-standard deviation score was 0.39±0.95. The mean TDD was 0.93±0.36 IU/kg and the mean C-peptide level was 0.26±0.31 ng/mL. The mean HbA1c was 8.6%±1.4%, and the average daily SMBG was 3.8±2.1 times in adolescent with T1DM (Table 1).
The mean numbers of SMBG performance during the school day was 1.3±1.2 times per day. While total 10 participants (16.4%) reported less than one SMBG checks per day, 18 subjects (29.5%) checked blood glucose less than one time per day in schools. About half of participants (n=31) was provided with school supports from teachers or friends for glycemic control including SMBG measurements. Only 9.8% (n=6) of all subjects received assistance from friends, and 32.8% performed their SMBG in classrooms during the school day (Table 1). On average, the subjects performed 1.4±1.0 insulin injection per day at school.
Comparison of related factors in T1DM adolescents according to daily frequency of SMBG and frequency during the school day
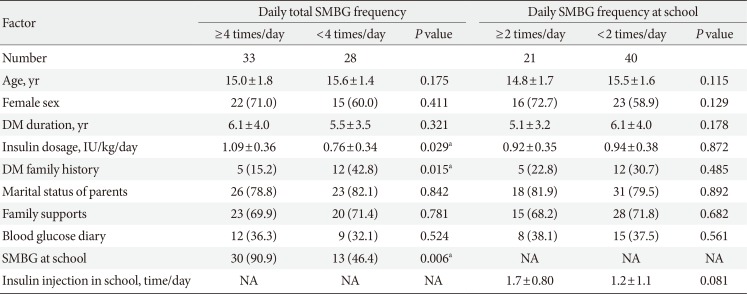
According to the guidelines of International Society of Pediatric and Adolescent Diabetes (ISPAD), SMBG frequency is recommended more than or equal to four times per day [1415]. Since middle and high school students in Korea spend an average of 10 hours (8 to 14 hours) a day at school, half out of required daily SMBG numbers in students with T1DM is supposed to be carried out at the school setting. Subjects were divided into two groups, each of whom performed SMBG more than or equal to four times and less than four times, depending on the number of daily SMBG testing. Subjects in a group that performed SMBG ≥4 times/day showed significantly higher TDD, higher SMBG frequency at school and lower DM family history compared to subjects in other group with less than four times of daily SMBG (Table 2). On the other hand, there was no significant factors between two groups, which more than or equal to two times a day of SMBG or less than two times a day of SMBG during the school day (Table 2).
The association between optimal glycemic control and frequency of SMBG
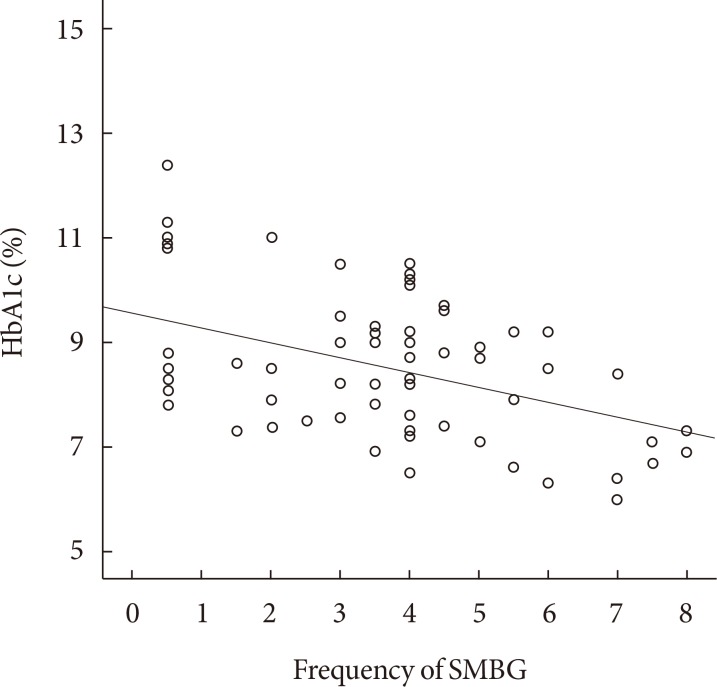
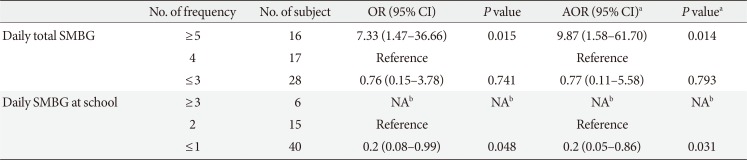
As the frequency of SMBG increased, HbA1c levels declined; the average fall in HbA1c was 0.42%, depending on increase in the number of SMBG per day (Fig. 1). Upon the stepwise multiple logistic regression analysis, the odds of achieving the target HbA1c in participants who performed SMBG ≥5 times per day significantly increased 9.87 folds (95% CI, 1.58 to 61.70; P=0.014) after adjustment for family history of DM and TDD compared with those performed SMBG four times a day (Table 3). In the subjects whose SMBG frequency was less than once a day during the school day, the adjusted odds to reach target HbA1c (<7.5%) significantly decreased to 0.2 folds (95% CI, 0.05 to 0.86; P=0.031). This result showed an 80% reduction in the OR compared to the reference group, which performing two blood glucose measurements in the school setting. All subjects in group of daily SMBG at school ≥3 were in HbA1c <7.5% (Table 3).
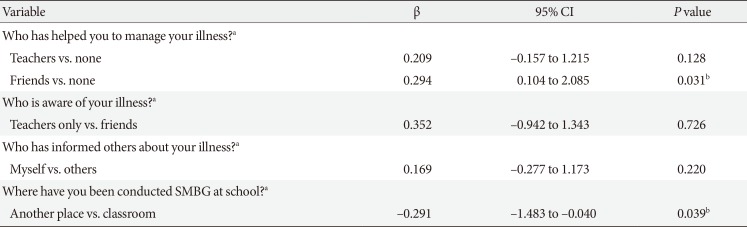
The association between school-related factors and SMBG frequency in the usual school setting
In order to investigate the association of school-related factors on the frequency of SMBG testing at school [16], a multiple linear regression analysis was performed. Subjects who received assistance from friends (β, 0.294; 95% CI, 0.104 to 2.085; P=0.031) and those who performed SMBG in classrooms (β, −0.291; 95% CI, −1.483 to −0.040; P=0.039) showed higher number of SMBG during the school day, as compared with those who did not. However, assistance from teachers was not associated with SMBG frequency in the usual school setting (Table 4).
DISCUSSION
With the introduction of glucometers 40 years ago, SMBG has emerged as the most important tool in glycemic control. The frequency of SMBG could be seen as a surrogate tool for self-care of diabetes. Checking the accurate blood glucose value is the starting point for adjusting insulin dose, physical exercise, and life style [4].
In general, youth with T1DM frequently shows a poor compliance to self-care of diabetes including performance of SMBG [1415]. In light of potential occurrences and progress of chronic diabetic complications during puberty, building healthy lifestyle to achieve proper diabetes management is linked to the healthy adulthood in the future. Pubertal changes make them more likely to form unhealthy lifestyle, while daily insulin requirements increase as a result of physiologic pubertal insulin resistance [17]. Also, parents-T1DM adolescent's relationships are often challenged which can create diabetes care-related family conflict and adversely affect adequate glycemic control. Despite of proven unfavorable aspects during adolescent period, SMBG is necessary for individuals to achieve optimal glycemic control. This study showed that frequent blood glucose monitoring in Korean adolescents with T1DM reflects commitment to diabetes control, which is consistent with the results of several studies on youths in other countries [4579] and Korea [18]. The mean HbA1c reduction was 0.42% for one additional SMBG per day under the SMBG frequency up to 5 per day, this is similar to the results reported by Ziegler et al. [4]. Also, Consensus Guidelines of ISPAD and American Diabetes Association recommended that four or more times per day are generally necessary for pediatric T1DM [1416], which nearly corresponds to the results of this study.
This study showed that Korean T1DM adolescents whom performed SMBG more than or equal to five times daily tended to have significantly target blood glucose levels compared with those who did not. In this study, the mean total frequency of SMBG in Korean T1DM adolescents was 3.8 per day. As compared with the mean frequency of SMBG performed by European (DPV-WISS database) [4] and American adolescents [7], which were 4.4 per day and 5.2 per day respectively, Korean adolescents presented fewer testing frequency. Further, the proportion of adolescents performing SMBG less than once per day was 16.4% (10/61), which is about twice as much as that of Korean adults with T1DM (8.7%) [19]. It is indicated the seriousness of the aspect on blood glucose self-monitoring among T1DM adolescents in Korea.
The most significant factor affecting the daily SMBG frequency in T1DM Korean youth could be the SMBG frequency during the school day. School-life is one of the most important environmental factors among adolescents in Korea because they spend as long as 8 to 14 hours per day at school. In this study, high school students presented a lower overall daily SMBG counts (total daily 3.1 SMBG including 0.9 SMBG at school) than middle school students (total daily 4.6 SMBG including 1.3 SMBG at school), which may be because they spend more time during the school day than middle school students and life patterns are fixed.
Even about 29% of all subjects reported less than one blood glucose measurement per day at the school setting, and the average frequency of SMBG during the school day was only 1.3±1.2 times per day. There might be several possible reasons to explain these results. First of all, adolescents have a tendency to avoid becoming the center concern of attention from their friends and teachers due to diabetes self-care [202122]. The unwillingness of most adolescents to inform friends of their diabetes condition has also been reported, which found that one third of Korean youth with T1DM performed self-insulin injections in school toilet [23]. Secondly, about half (50.9%) of adolescents reported low compliance with SMBG due to lack of time during school life, which can be interpreted as environmental constraints such as short break and inappropriate spatial conditions in school [24]. Environmental factors could be the most important parts affecting SMBG adherence to teenagers. Thirdly, proper diabetes-care system at school has not yet been established in Korea. One-third of Korean health teachers had no any experiences for managing students with diabetes [25].
Several studies in other countries have revealed that students with diabetes should receive appropriate care, including aid provided by trained staffs in school to reduce the risk of short- and long-term complication [2627]. In this study, teachers' help did not influence the frequency of SMBG, which may be due to improper school-intervention system for diabetes care in Korea. The number of SMBG measurements in the school setting was significantly higher for individuals who were helped by their friends and those who measured SMBG in the classrooms. The findings suggest that a supportive school system including peer participation for diabetes-care should be developed [2829]. Family supports of diabetes management did not affect the frequency of daily SMBG, which was consistent with previous studies [2223].
This study has several limitations. Firstly, the number of enrolled participants was insufficient. Secondly, there may have been response biases due to using questionnaires. Thirdly, there was not enough survey into factors that may affect diabetes control, such as annual household income, and parental education level.
However, this is the first study to validate the correlation between the number of daily SMBG and HbA1c levels in Korean adolescents with T1DM, and to investigate the condition that SMBG testing can be properly at school. In conclusion, the daily SMBG frequency was significantly associated with HbA1c levels among T1DM adolescents in Korea. It would be necessary to establish the school environments that can facilitate adequate glycemic control as well as proper SMBG testing during the school day.
 XML Download
XML Download