

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dipeptidyl peptidase-4 (DPP-4) inhibitors have emerged as a new treatment option for patients with type 2 diabetes. DPP-4 inhibition increases the level of active incretin hormones, such as glucagon-like peptide-1 (GLP-1) and gastric inhibitory polypeptide. These hormones stimulate insulin secretion by direct action on GLP-1 receptors in β-cells and by indirect glucose-dependent neuronal stimulation in the gut [1].
Type 2 diabetes mellitus is a progressive disease characterized by decreased insulin secretion and increased insulin resistance [2]. When glycemic control is poor with dual oral hypoglycemic agents (OHAs), insulin injection or triple combination therapy with other OHAs should be considered [3]. However, some patients are reluctant to start insulin therapy because of psychological antipathy such as misperceptions about worsening of the disease, injection fear [4], or weight gain. DPP-4 inhibitors could be another therapeutic option for sub-stituting insulin therapy in addition to ongoing submaximal sulfonylurea and metformin combination therapy for patients with uncontrolled hyperglycemia [567].
There seems to be individual variability in the response to DPP-4 inhibitors. In some patients, DPP-4 inhibitors have shown more prominent effects in lowering glycemia indicators such as the glycosylated hemoglobin (HbA1c) level. Previous studies have analyzed the predictors of a clinical response to DPP-4 inhibitors [8910111213], but the predictors suggested by these studies were somewhat inconsistent, and these studies did not analyze the effects of combination therapy with sulfonylurea and DPP-4 inhibitors.
The risk of hypoglycemia should be considered when a DPP-4 inhibitor is added to a sulfonylurea-based regimen. The issue of sulfonylurea dose reduction has been raised when using DPP-4 inhibitors and sulfonylurea together [1415]. In 2010, the Japan Association for Diabetes Education and Care released a guideline for reducing the dose of three major sulfonylureas when adding a DPP-4 inhibitor to prevent hypoglycemia [16]. However, it is unclear which patients are true candidates for sulfonylurea dose reduction when given DPP-4 inhibitor combination therapy.
In this study we evaluated the efficacy of triple combination therapy that added a DPP-4 inhibitor to sulfonylurea and metformin combined therapy. We analyzed the clinical predictors of a rapid response to a DPP-4 inhibitor when newly added to ongoing OHA combination therapy. We also analyzed the characteristics of those patients who experienced hypoglycemia, and we identified the characteristics of patients needing a reduction in sulfonylurea dose when given the DPP-4 inhibitor-OHA combination therapy.
METHODS
Study participants
In this retrospective observational study, we included those patients with type 2 diabetes who were seen in the diabetes out-patient clinic at Seoul National University Bundang Hospital (SNUBH) from March 2009 to October 2011. The eligible subjects were 918 patients aged 21 to 89 years who were prescribed a DPP-4 inhibitor in addition to the sulfonylurea and metformin combination. Patients were excluded if they had a history of type 1 diabetes, a serious medical illness, insulin use, or poor compliance because of mental illness. Patients who changed the medication to a different type of sulfonylurea or DPP-4 inhibitor or who added another type of OHA were also excluded. Among 894 patients, 87 were lost to follow-up. Hypoglycemic episodes were reported in the medical records with or without a measured glucose level. Patients with severe hypoglycemia were identified from the records of emergency room visits or the necessity for medical assistance. The laboratory data, use of medication, sulfonylurea dose reduction, and episodes of hypoglycemia were retrieved from the electronic medical records. Finally, 807 patients who were prescribed sitagliptin (n=518) or vildagliptin (n=289) were included and reviewed up to 52 weeks after the addition of the DPP-4 inhibitor.
To evaluate the response of the DPP-4 inhibitor added to sulfonylurea, we divided the patients into two groups based on the change in HbA1c levels for the initial 3 months; those who showed ≥25% reduction in HbA1c within 12 weeks were defined as rapid responders, and the others were defined as non-rapid responders. Previous clinical trials [1417] reported HbA1c reductions of -0.55% to -2.07%, which were greater with a higher baseline HbA1c. Rapid declines in HbA1c were also shown within the first 6 to 12 weeks in these studies. Hence, we calculated the change in HbA1c levels within 12 weeks in these studies and set the criteria of 25% above the range of -4.4% to -23.5% of the baseline HbA1c level.
This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital, and it conformed to the provisions of the Declaration of Helsinki (as revised in Edinburgh 2000).
Metabolic and clinical parameters
The patients who achieved the target HbA1c levels of ≤7% and ≤6.5% were assessed at baseline, 12, 24, and 52 weeks. Plasma glucose levels were measured using a Hitachi 747 chemistry analyzer (Hitachi, Tokyo, Japan). HbA1c levels were measured using a Bio-Rad variant II Turbo HPLC analyzer (Bio-Rad, Hercules, CA, USA) at Seoul National University Bundang Hospital, a National Glycohemoglobin Standardization Program level II-certified laboratory. The fasting plasma concentrations of total cholesterol, triglycerides, high density lipoprotein cholesterol, and low density lipoprotein cholesterol were measured using the Hitachi 747 chemistry analyzer. Plasma C-peptide and insulin concentrations were measured by radioimmunoassay (Linco, St. Louis, MO, USA). The homeostasis model assessment (HOMA) was used to assess β-cell function (HOMA-β) and insulin resistance (HOMA-IR) [18]. HOMA-IR was calculated using the formula: fasting insulin (µU/mL)× [fasting glucose (mg/dL)/405]. HOMA-β was calculated using the formula: 20×fasting insulin (µU/mL)/[fasting glucose (mg/dL)-63]. Clinical parameters including age, sex, height, weight, duration of diabetes, and doses of medications were collected from electronic records. Body mass index (BMI) was calculated using the formula: body weight in kg divided by height in meters squared.
Statistical analyses
Statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). We used the Kolmogorov-Smirnov test to verify whether the data were normally distributed. Data are shown as the mean±standard deviation or as number and percentage. Analysis of variance with repeated measurements and paired t-tests were used to analyze the changes in glycemia parameters. Student t-test for continuous data and the chi-square test for categorical data were used to compare rapid responders and non-rapid responders. Student t-test and chi-square test were also used to compare between groups with or without episodes of hypoglycemia. We also performed logistic regression analysis using baseline HbA1c levels, male sex, and duration of diabetes to predict the rapid responders for DPP-4 inhibitor add-on therapy to the sulfonylurea and metformin combination. P values ≤0.05 were considered significant.
RESULTS
Demographics and baseline characteristics
Patient characteristics are shown in Table 1. The mean age was 61.1 years, the mean duration of diabetes was 11.5 years, and 58.6% were men and 41.4% women. The mean baseline HbA1c level was 8.4%, and the baseline fasting plasma glucose (FPG) and 2-hour plasma glucose (2hPG) concentrations were 153.4 and 261.1 mg/dL, respectively. The most frequent sulfonylurea given was glimepiride (88.8% of patients) with a mean dose of 4.1±2.1 mg/day, and the dose of metformin was 1,241.9±483.8 mg/day. Among 807 patients, dose reduction of sulfonylurea was performed in 160 patients, while the others maintained or increased the sulfonylurea dose during the 1-year follow-up after DPP-4 inhibitor add-on. In this study, the dose of sulfo-nylurea was reduced when a patient showed a rapid improvement in HbA1c levels or reported minor or major hypoglycemic symptoms after addition of the DPP-4 inhibitor. Patients with sulfonylurea reduction were more frequently prescribed glimepiride (95.0% vs. 87.3%, P=0.021) or sitagliptin (74.4% vs. 61.7%, P=0.003) and had a lower BMI (25.0±3.5 kg/m2 vs. 25.6±3.4 kg/m2, P=0.045) than the patients without sulfonylurea reduction (data are not shown).
The types of DPP-4 inhibitors used were sitagliptin for 64.2% of patients and vildagliptin for 35.8% of patients. The dose of the DPP-4 inhibitor was 100 mg/day in 95.7% of patients. Twenty-two patients were prescribed sitagliptin, and 12 patients (4.2%) were prescribed vildagliptin at a dose of 50 mg/day. One patient was prescribed sitagliptin at a dose of 75 mg/day. The mean BMI was 25.5 kg/m2, indicating a tendency toward patients being overweight.
Efficacy of triple combination therapy
The percentages of patients who achieved the target HbA1c ≤7% and ≤6.5% levels were 33.3% (n=269) and 14.0% (n=113) at 12 weeks of DPP-4 inhibitor add-on, respectively (Fig. 1A). These percentages increased slightly at 24 weeks to 35.2% (n=284, HbA1c ≤7%) and 14.5% (n=117, HbA1c ≤6.5%), respectively, and were maintained at 52 weeks (32.3% and 13.4%, respectively). The mean change in HbA1c level from the baseline of 8.4% at 12 weeks was -0.8%±1.2% (P<0.001). The changes in FPG and 2hPG at 12 weeks after the addition of a DPP-4 in-hibitor were -18.0±49.9 and -38.3±87.2 mg/dL, respectively (P<0.001 for each). These reductions in HbA1c, FPG, and 2hPG levels at 12 weeks were maintained at 52 weeks. At 52 weeks, the changes in HbA1c, FPG, and 2hPG from the baseline were -1.0%±1.9%, -13.5±52.1, and -23.1±86.8 mg/dL, respectively.
The changes in glycemia parameters were similar in the sitagliptin-treated group and the vildagliptin-treated group at 12 and 24 weeks (Fig. 1B). The changes in HbA1c and 2hPG levels from baseline to 52 weeks were slightly greater in the si-tagliptin group than in the vildagliptin group: -1.2%±2.2% vs. -0.8%±1.4% for HbA1c (P=0.016) and -33.7±91.1 mg/dL vs. -8.7±79.0 mg/dL for 2hPG (P=0.029). The baseline insulin concentration was 15.2 µU/mL, and the C-peptide concentration was 2.2 ng/mL. HOMA-β and HOMA-IR were 61.1± 41.0 and 2.1±1.2, respectively. Insulin and C-peptide concentrations increased gradually from baseline to 52 weeks after treatment (data not shown). The changes in insulin and C-peptide concentrations from baseline to 52 weeks were 1.1± 7.8 µU/mL (P=0.241) and 0.2±0.8 ng/mL (P=0.252).
Predictors of clinical responses to DPP-4 inhibitors added to sulfonylurea-based regimens
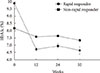
Patients with a reduction in HbA1c of ≥25% within 12 weeks were defined as rapid responders (n=66, 8.2% of enrolled patients). For these patients, the HbA1c levels were 10.1% at baseline and 6.9% at 12 weeks after the addition of DPP-4 inhibitors (P<0.001). Excluding 26 patients with no available HbA1c values at 3 months, the others were defined as non-rapid responders. The 12-week values were less than the target HbA1c of 7.0% (Fig. 2). This rapid improvement in HbA1c was maintained at 7.0% at 24 weeks and at 6.7% at 52 weeks. The other group of patients (non-rapid responders) also showed an improvement in HbA1c levels from 8.2% at baseline to 7.4% at 52 weeks (P<0.001). The duration of diabetes was shorter (8.8 years vs. 11.7 years, P=0.002) in the rapid responders than in the non-rapid responders, and a higher percentage of rapid responders were men (71.2% vs. 56.9%, P=0.027) (Table 2). Baseline HbA1c and FPG levels were higher in rapid responders than in non-rapid responders: 10.1% vs. 8.2% for HbA1c (P<0.001) and 174.3 mg/dL vs. 150.9 mg/dL for FPG (P=0.007), respectively. Baseline C-peptide concentrations and HOMA-IR levels were also higher in rapid responders: 3.0 ng/mL vs. 2.1 ng/mL for C-peptide (P=0.030) and 2.5 vs. 2.1 for HOMA-IR (P=0.044). Fasting insulin concentrations and HOMA-β levels were non-significantly higher in the rapid responders. There were no differences in age, BMI, creatinine concentration, and other parameters between rapid and non-rapid responders. In the logistic regression, higher baseline HbA1c levels and shorter durations of diabetes were independent predictors for the rapid responders with the DPP4 inhibitor add-on, while male sex showed marginal significance (P=0.054) (Table 3).
Characteristics of patients who experienced hypoglycemia
In the rapid responder group, there were more patients with symptoms of hypoglycemia than in the non-rapid responder group (24.2% vs. 13.4%, P=0.026). The dose of sulfonylurea was reduced more frequently in the rapid responder group than in the non-rapid responder group (33.3% vs. 18.2%, P=0.005).
Among the 918 patients given a DPP-4 inhibitor in addition to sulfonylurea, 117 patients experienced hypoglycemia. Severe hypoglycemia was reported in 17 patients. Among the 17 patients with severe hypoglycemia, 16 were older than 70 years and one was 63 years old with renal impairment. Three of these 17 patients had renal impairment (creatinine >1.4 mg/dL), three had poor oral intake, and three were prescribed an increased dose of sulfonylurea.
Except for HbA1c, several other factors might be related to hypoglycemia (Fig. 3). The patients with hypoglycemic symptoms had a higher percentage of women (53.0% vs. 39.4%, P=0.008), lower body weight (65.2±10.7 kg vs. 68.9±12.3 kg, P=0.003), lower triglyceride levels (134.4±74.1 mg/dL vs. 156.6±105.0 mg/dL, P=0.031), lower FPG levels (138.0±38.7 mg/dL vs. 156.1±48.7 mg/dL, P<0.001), and higher HOMA-β levels (83.3±51.2 vs. 57.5±38.1, P=0.001) than the patients without hypoglycemic symptoms.
DISCUSSION
In this study, we found that the addition of a DPP-4 inhibitor to an ongoing submaximal dose of sulfonylurea and metformin combination in Korean patients with type 2 diabetes was effective in improving glycemia parameters for up to 52 weeks. Based on the previous studies [1417], we identified the characteristics of rapid responders to this triple combination therapy as those showing a decrease in HbA1c levels of ≥25% in the initial 12 weeks of the add-on. Rapid responders were more likely to be men and had a shorter duration of diabetes and higher baseline levels of FPG, HbA1c, C-peptide, and HOMA-IR. More patients in the rapid responder group reported hypoglycemia or required a further reduction in sulfonylurea dose compared with the non-rapid responder group. The patients with hypoglycemia in this study were more likely to be female, with a lower body weight and triglyceride and FPG concentrations and a higher HOMA-β level.
In clinical practice, some patients showed an exceptional response to DPP-4 inhibitors. We wanted to characterize these patients, especially in the context of the DPP-4 inhibitor add-on to the combination of submaximal doses of sulfonylurea and metformin. We were also interested in identifying important clinical parameters that could help predict a rapid response to DPP-4 inhibitors.
Our clinical predictors of a rapid response to the DPP-4 inhibitor added to the sulfonylurea-based regimen were consistent with parameters reported by some studies but differed from those reported by other studies [8910111213]. The inconsistency might be due to a different study design. We included a large numbers of patients of the same ethnicity (n=807) who were prescribed an ongoing sulfonylurea and metformin combination at one diabetes center. In contrast with other studies, BMI and age were not significantly associated with a rapid response to the addition of a DPP-4 inhibitor [89]. The rapid changes in FPG and HbA1c levels and shorter duration of diabetes were more frequent in rapid responders, and this finding is consistent with previous studies [1019].
The mechanism of glycemic improvement amplified by the combination of DPP-4 inhibitor and sulfonylurea is thought to reflect intensified insulin secretion by the pancreatic β-cells, the common target of these drugs [20]. Exchange protein activated by cAMP 2 (Epac2) is activated by sulfonylurea and incretin hormone [2122], which increases insulin secretion and synergistic improvement in hyperglycemia and β-cell capacity [23]. Those who showed rapid response to a DPP-4 inhibitor in this study had a higher C-peptide level and a shorter duration of diabetes at baseline. We propose that their improved β-cell capacity might be related to the synergistic potentiation for insulin secretion with the sulfonylurea and DPP-4 inhibitor combination.
In this study population, 35% of the patients with poor glycemic control under a near-maximum dose of metformin and sulfonylurea reached a target HbA1c level of 7.0% in 12 weeks after the add-on DPP-4 inhibitor as triple therapy, and this effect was maintained for up to 52 weeks. A previous randomized, parallel-group study has shown the efficacy and safety of sitagliptin in 229 patients taking metformin and sulfonylurea [14] in which there was a 0.89% reduction in the HbA1c level to 8.3% from the baseline to 24 weeks [14]. Our group has reported previously that adding a DPP-4 inhibitor to an insulin-based regimen was more effective than a 25% increase in insulin dose [24]. In clinical practice, some patients are resistant to starting insulin therapy. Our results suggested that adding a DPP-4 inhibitor to ongoing submaximal doses of sulfonylurea and metformin as a triple combination therapy may be preferable to switching to insulin therapy, even for patients with a high HbA1c level with a long duration of diabetes.
Hypoglycemia is the most important obstacle in treating patients with diabetes. Therefore, we also wanted to identify the clinical characteristics of patients prone to hypoglycemia when given a DPP-4 inhibitor as part of triple therapy. Being female, having a lower BMI, lower triglyceride and FPG concentrations, and a higher HOMA-β level were significantly associated with hypoglycemia in patients receiving the triple therapy. In patients with preserved β-cell function, the potentiated insulin release stimulated by the addition of a DPP-4 inhibitor increased the percentage of patients reporting hypoglycemia. Lower FPG and triglyceride levels are related to lower hepatic glucose production in the fasting state and increase the risk of hypoglycemia. Consistent with two previous Korean studies [1012], we found no relationship between BMI and the response to a DPP-4 inhibitor; however, in our study, lower body weight was related to more frequent hypoglycemia. A reduction in the dose of sulfonylurea should be considered in elderly patients, especially those with decreased renal function and poor oral intake, when a DPP-4 inhibitor is added.
This study had limitations. This was a retrospective study, although it included a large number of patients. Minor hypoglycemia was self-reported by patients, and not all incidents were accompanied by a documented glucose level. The enrolled subjects were all Koreans with a long duration of diabetes and uncontrolled glycemic status. In addition, the patient profiles in this study differed from those of previous studies. The mean duration of diabetes was 11.5 years in our patients, and they had uncontrolled hyperglycemia while under treatment with high doses of sulfonylurea and metformin. Thus, the data from this study may not be generalizable to all ethnic groups or types of patients.
Our data suggested that reducing the dose of sulfonylurea did not reduce the efficacy of triple therapy in providing glycemic control even in patients with a longer duration of diabetes and uncontrolled hyperglycemia. Dose reduction could be considered in patients with low FPG concentrations, preserved β-cell function, and a favorable lipid profile.
In conclusion, this study has provided evidence of the efficacy of DPP-4 inhibitor add-on therapy for patients taking a sulfonylurea and metformin combination at near-maximum dose. The triple combination therapy may be preferable for some patients, even for those using the maximum dose of sulfonylurea and metformin combination, instead of switching to an insulin-based regimen. A reduction in sulfonylurea dose could be recommended when starting the DPP-4 inhibitor add-on with a sulfonylurea-based regimen in female patients with lower body weight and triglyceride and FPG concentrations and higher HOMA-β levels, especially in elderly patients with deteriorated renal function. In the future, large prospective studies are needed to confirm the clinical predictors of the response to the addition of a DPP-4 inhibitor to the current OHA regimen and the proper target for sulfonylurea reduction to avoid hypoglycemia.





 XML Download
XML Download