

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of diabetes in Korea has increased six- to sevenfold from 1.5 to 9.9% over the past 40 years [1,2]. The number of people with diabetes worldwide is expected to increase 11.4% from 366 million in 2011 to 552 million by 2030, affecting one in 10 adults [3]. The same trend is expected in Korea. This global increase in the prevalence of diabetes will inevitably lead to increases in the prevalence of diabetic microvascular and macrovascular diseases, and consequently, significantly increased health care expenditure [4].
In Korea, type 2 diabetic patients without complications spend about 1,184,563 won annually on health care. Diabetic patients with microvascular disease spend up to 4.7 times as much, patients with macrovascular disease up to 10.7 times as much, and patients with both complications 8.8 times as much as those with no complications. The medical cost of diabetes mellitus covered by the national health insurance corporation is 3.2 trillion won and accounted for 19.2% of all medical costs [5].
Diabetes and its complications have become major causes of morbidity and mortality in Korea [6]. Although diabetes-related mortality has decreased recently from 25.1 per 100,000 persons in 2002 to 19.6 per 100,000 persons in 2009, diabetes is still the fifth-leading cause of death in Korea [6]. The rate of death among patients with diabetes is about twice as high as that among persons without diabetes [7]. The most common cause of death is cardiovascular disease (30.6%), followed by infectious disease (25.3%), cancer (21.9%), congestive heart failure (7.1%), renal disease (4.7%), liver disease (2.7%), and diabetes itself (1.9%) [2].
Despite the seriousness of diabetic complications, 30% to 70% of patients receive inadequate care [8], and only 40% of treated diabetic patients achieve the optimal control, defined as an HbA1c level <7% [8,9]. The serious outcomes from diabetic complications and inadequate glucose control in diabetic patients prompt the need for more aggressive efforts to provide optimal metabolic control.
COMPLICATIONS OF DIABETES MELLITUS
Type 2 diabetes mellitus is associated with a high rate of complications related to cardiovascular disease and diabetic nephropathy, retinopathy, and neuropathy. In 2006, 30.3%, 38.3%, and 44.6% of patients were found to have microvascular complications such as microalbuminuria, retinopathy, and neuropathy, respectively from Korean nationwide survey. The prevalence of macrovascular complications including coronary artery disease, cerebrovascular disease, and peripheral artery disease was 8.7%, 6.7%, and 3.0%, respectively [9]. The prevalence of diabetic foot was 4.4%, and 44.8% of patients with an amputated foot had diabetes mellitus [8,10]. The prevalence of macrovascular complications seems underestimated in these data. In a study of 343 patients with diabetes mellitus, the prevalence of cardiovascular complication was 23.6% [11], and in another study of 406 patients with diabetes, extracranial internal carotid artery stenosis ≥40% was detected in 5.2% of the patients [12]. In addition, the prevalence of macrovascular complication was 10.8% from recent The Korean National Diabetes Program (KNDP) data [13] and there is reference from 2005 Korea National Health and Nutrition Examination Survey (KNHANES) data in Table 1.
MICROVASCULAR COMPLICATIONS
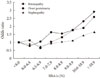
The role of hyperglycemia in the development of microvascular complications of diabetes, such as nephropathy, retinopathy, and neuropathy, is well documented. The incidence of microvascular complications begins to increase at an HbA1c level >7.0% and increases by 30% to 40% per 1% increase in HbA1c level from over 8,000 patients (Fig. 1). Microvascular complications are closely related to age, duration of diabetes, and glycemic control, and this relationship is stronger than that with macrovascular complications [9].
Diabetic retinopathy is the most common microvascular complication of diabetes mellitus, and its prevalence is strongly related to the duration of diabetes. It is the most frequent cause of new cases of blindness among adults aged 20 to 74 years. In Ansung cohort study (prospective, rural, community cohort in Korea), the prevalence of any diabetic retinopathy was 2.9% and the proper cutoff of HbA1C value for detecting any diabetic retinopathy was 6.6% (unpublished data).
Diabetic nephropathy is characterized by albuminuria (≥300 mg/day) and a reduced glomerular filtration rate. It is often present at the time of the diagnosis of diabetes after the kidney has been exposed to chronic hyperglycemia during the prediabetic phase. Patients with microalbuminuria who progress to macroalbuminuria (300 mg/24 hr) are likely to progress to end-stage renal disease (ESRD) [14]. Diabetes is a major cause of chronic kidney disease (CKD) and is recognized as the most common cause of ESRD in the USA and Korea. About 40% of United States adults with diagnosed or undiagnosed diabetes had some degree of CKD in the 1999 to 2006 National Health and Nutrition Examination Survey [15]. In Korea, 56.7% of CKD patients and 70.5% of ESRD patients has diabetes [8].
The prevalence of peripheral neuropathy has been estimated at 40.0% to 44.6% [9,10]. At present, there is no specific treatment for the underlying nerve damage other than to improve glycemic control, which may slow the progression modestly. Glycemic control reduces microvascular complication outcomes but cannot reverse neuronal loss [16].
MACROVASCULAR COMPLICATIONS
Type 2 diabetes increases the risk of coronary heart disease by two- to fourfold [17]. The case fatality rate after myocardial infarction is higher in patients with diabetes than in patients without diabetes [18]. The association between diabetes and coronary heart disease is likely to become more important for two reasons. First, the incidence of type 2 diabetes is increasing among both high-risk and low-risk populations. Second, although the rate of death caused by coronary heart disease in the overall population has declined markedly over the past 35 years, this has not been the case among persons with diabetes [7].
Cardiovascular disease is the major cause of morbidity and mortality for individuals with diabetes and is the largest contributor to the direct and indirect costs of diabetes. Older age, high blood pressure, and smoking history are major risk factors for the development of macrovascular complications. A smoking history in males can be both a risk factor and a predictive factor for earlier development of macrovascular complications in Korean patients with type 2 diabetes [19].
Microvascular complications of diabetes increase the risk of cardiovascular events in diabetic patients. Although diabetic retinopathy is not associated with the presence of atherosclerotic plaque, it is associated with increased carotid intima-media thickness, and the increase in intima-media thickness is associated with the presence of plaque, which predisposes patients to cardiovascular disease. Microalbuminuria and a low glomerular filtration rate (<60 mL/min/1.73 m2) increase the risk of major cardiovascular events and death [20,21]. Diabetic polyneuropathy was also independently associated with a high prevalence of cardiovascular disease in type 2 diabetic patients [22]. These data imply that the microvascular complications of diabetes are related indirectly to the macrovascular complications of diabetes, similar in Korea [23].
THE EFFECT OF GLYCEMIC CONTROL ON DIABETIC COMPLICATIONS
Intensive glycemic control has been suggested as an effective treatment for reducing the burden of cardiovascular disease and microvascular complications in people with diabetes. The United Kingdom Prospective Diabetes Study and the Kumamoto study showed that early intensive glycemic control can delay the onset and progression of diabetic retinopathy, nephropathy, and neuropathy compared with conventional treatment [21,24-26]. Intensive glucose control involving gliclazide (modified release) and other drugs as required lowered the HbA1c value to 6.5% and reduced by 10% the relative risk for the combined outcome of major macrovascular and microvascular events, primarily because of a 21% reduction in incidence of nephropathy [27]. In addition, the legacy effect was observed after 10 years of trial in the rate of microvascular complication and myocardial infarction [28]. In the Steno-2 study, the intensive therapy group had a 46% lower risk for all-cause mortality and a 57% lower risk of death from cardiovascular causes. One patient in the intensive therapy group progressed to ESRD compared with 6 patients in the conventional therapy group, and fewer patients in the intensive therapy group required retinal laser therapy [29].
Although there are many benefits of intensive glucose-lowering treatment for preventing macrovascular and microvascular events, it remains uncertain whether these benefits outweigh the risks. Intensive blood glucose control decreases the risk of developing microvascular complications but not macrovascular disease in patients with type 2 diabetes. In the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study, an intensive glucose-lowering regimen reduced rate of 5-year nonfatal myocardial infarctions but was associated with a 22% increase in mortality [30,31]. A recent meta-analysis found that intensive glucose-lowering treatment has limited effect on the rates of all-cause mortality and death from cardiovascular causes. The data are conflicting: a 9% reduction to a 19% increase in all-cause mortality and a 14% reduction to a 43% increase in cardiovascular death rates. The harm associated with severe hypoglycemia might counterbalance the potential benefit of intensive glucose-lowering treatment [32]. The microvascular benefits of intensive therapy should be weighed against the increase in total and cardiovascular disease-related mortality, weight gain, and high risk of severe hypoglycemia [16].
However, multifactorial approaches in high risk patients with diabetes, such as tight glucose regulation and the use of anti-hypertensive medication, aspirin, and lipid-lowering agents, have been shown to reduce the risk of nonfatal cardiovascular disease among patients with type 2 diabetes mellitus and microalbuminuria. In high risk patients with type 2 diabetes, intensive treatment approaches with multiple drug combinations and behavior modification had sustained beneficial effects with respect to vascular complications and on rates of death from any cause and from cardiovascular causes [29].
ADIPOKINE AND DIABETIC COMPLICATIONS: RISK FACTORS FOR DIABETES
Several adipokines are implicated in the metabolic syndrome, coronary heart disease, and insulin resistance. We want to discuss some adipokines, which showed correlation with diabetes and metabolic syndrome in Korea. Lipocalin family proteins, including adipocyte fatty acid-binding protein (A-FABP), lipocalin-2, and retinol-binding protein 4 (RBP4), have been identified recently as adipokines associated with obesity, type 2 diabetes, and the metabolic syndrome. Serum A-FABP is associated with glucose dysregulation, and its level predicts the development of type 2 diabetes and the development of the metabolic syndrome independently of adiposity and insulin resistance [33,34]. Serum A-FABP level is independently associated with carotid atherosclerosis [35]. Serum lipocalin-2 level is significantly elevated in patients with coronary heart disease and is independently associated with coronary heart disease. These findings suggest that serum lipocalin-2 levels may be useful for assessing coronary heart disease risk [36]. Plasma RBP4 concentration is elevated in persons with impaired glucose tolerance and type 2 diabetes [37]. High RBP4 and low plasma adiponectin concentrations are associated with the severity of glucose intolerance in women with previous gestational diabetes mellitus [38].
A low circulating vaspin level correlates with a high fitness level, whereas physical training in untrained individuals increases vaspin serum concentration [39]. Vaspin is also correlated with metabolic syndrome in men and coronary artery stenosis in women [40]. However, another study reported that circulating visfatin may not be a useful clinical biomarker of metabolic status [41].
A relationship between chemerin levels, cardiometabolic parameters, and degree of coronary stenosis has been reported in Korean patients with coronary artery disease [42].
Serum osteocalcin, an osteoblast-specific protein, has several hormonal features and is secreted into the general circulation by osteoblastic cells. Serum osteocalcin and osteoprotegerin levels are associated with glucose metabolism and atherosclerosis parameters in people with type 2 diabetes mellitus [43,44].
Even though there are many studies about adipokines and metabolic diseases, we need large number, prospective studies to see the causality between the candidate adipokines and diabetic complications more clearly.
CONCLUSION
The increasing prevalence of diabetes mellitus and its related complications have contributed to a substantial increase in morbidity and mortality in Korea. However, the proportion of patients with type 2 diabetes achieving adequate glucose control is relatively low. Multifactorial treatment approaches that target hypertension, dyslipidemia, and microalbuminuria, and that provide intensive glycemic control are urgently needed to control diabetes. These comprehensive and integrated health interventions will lead to further improvement in the management of diabetes.

 XML Download
XML Download