

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare cause of pulmonary hypertension that presents as obstructive pulmonary artery remodeling with organized and fibrotic changes as a consequence of acute pulmonary thromboembolism (PTE). CTEPH develops in about five individuals per million annually and in 0.56% to 6.1% of individuals after acute thromboembolism.1)2)3)4) By definition, CTEPH occurs within the first two years after the initial symptomatic PTE event, and it usually occurs three to six months after this event. However, cases are frequently not associated with a previous history of acute PTE. Chronic thromboembolic disease (CTED) is a similar entity that can be diagnosed regardless of pulmonary hypertension.5) Because of the poor functional status and chronicity of CTEPH, the classic and curative strategy of open pulmonary endarterectomy (PEA) cannot be applied in some patients with lesions involving distal vessels.1) Balloon pulmonary angioplasty (BPA) or percutaneous transluminal pulmonary angioplasty (PTPA) were recently introduced by groups in Europe and Japan for use in these inoperable cases, which has led to significant improvement in functional and hemodynamic status in patients with CTEPH.6)7) In South Korea, there are recent reports of early outcomes after BPA and multidisciplinary approaches in patients with CTEPH.8)9)
PATHOPHYSIOLOGY OF CHRONIC THROMBOEMBOLIC PULMONARY HYPERTENSION
Pathophysiologically, thrombotic occlusion of the pulmonary artery results in high pulmonary vascular resistance that causes right heart overload and failure of right heart that eventually impacts normal activity. Risk factors for the development of CTEPH include recurrent embolic events, initial high pulmonary artery pressure at diagnosis, hemostatic risk factors such as antiphospholipid antibody syndrome, lupus disease, and other medical conditions.1)4) Guidelines for diagnosis of CTEPH recommend the presence of sustained thrombotic burden even after three months of anticoagulation to discriminate subacute disease from CTEPH.5) This diagnostic approach is based on the pathophysiology of the disease; however, these diagnostic criteria are not clinically applicable for all cases of CTEPH.
In contrast to acute thrombi, surgical specimens of patients with CTEPH showed complex patterns which are more organized, fibrotic and it attached firmly to the wall of the pulmonary artery and largely consist of collagen, elastin, inflammatory cells, and recanalization vessels. The exact mechanism of these organized and fibrotic changes are not yet fully known. However, initial inadequate and inappropriate anticoagulation affects this process of chronicity, as do underlying autoimmune disease, hematological abnormalities, or hypercoagulable tendencies.10) Organized and fibrotic occlusion of the pulmonary artery causes macrovascular obstruction and vasoconstriction, which can provoke sustained remodeling of vasculature even after normalization of pulmonary artery pressure with treatment.11) Remodeled small vessels are pathologically similar to idiopathic pulmonary arterial hypertension and demonstrate compatible structural changes as right-sided heart overload.
DIAGNOSIS
Baseline evaluations usually include cardiopulmonary exercise testing with oximetry and maximal oxygen uptake, six minute walk test, ventilation/perfusion lung scanning, computed tomography (CT) pulmonary angiogram, and echocardiographic assessment of right heart function. These test results are crucial for initial decisions and follow-up. According to the 2015 European guidelines, diagnosis of CTEPH begins by assessing symptoms and signs and obtaining echocardiography.5) If there is high or intermediate probability, a ventilation/perfusion lung scan is required to detect areas of malperfusion.12)13) The gold standard and final confirmation of CTEPH is selective angiogram with right heart catheterization. CT pulmonary angiography does not provide sufficient information because perfusion is dependent on visualizing small vessels. CT is usually used when deciding on the operability of CTEPH by assessing major vessel involvement. Contrary to other entities of pulmonary hypertension, patients that are properly diagnosed with CTEPH can dramatically improve after correction of the causative thrombotic barrier. A differential diagnosis of CTEPH should be considered, including peripheral pulmonary stenosis or pulmonary vasculitis causing pulmonary artery stenosis, such as Takayasu disease.
TREATMENT MODALITY OF CHRONIC THROMBOEMBOLIC PULMONARY HYPERTENSION
PEA is the treatment of choice in patients with CTEPH. One-third of CTEPH cases are inoperable due to co-morbidities or distal lesions, which are signs of poor prognosis. Percutaneous pulmonary artery procedures can be used in patients who cannot undergo PEA due to comorbid conditions or distal disease localization, and this procedure is now being introduced in many parts of the world. In addition to inoperability, bridging therapy is also needed for cases that are technically operable but have unacceptable risk-benefit or residual symptomatic pulmonary hypertension following surgical removal.1)
BALLOON PULMONARY ANGIOPLASTY FOR CHRONIC THROMBOEMBOLIC PULMONARY HYPERTENSION
First procedure
The first case series of balloon pulmonary angioplasty in patients with CTEPH was published in 2001.6) Feinstein et al.6) reported 18 patients with 47 procedure sessions and an average of 2.6 procedures per patients. They showed remarkable improvement in hemodynamic parameters and functional capacity; however, 11 of 18 cases were complicated by reperfusion pulmonary edema, and some patients required mechanical ventilation and died. Consecutive outcomes of BPA were rarely reported, and the 2009 European guidelines for pulmonary hypertension did not comment on angioplasty for CTEPH.13)
Current trends in balloon pulmonary angioplasty and practice guideline recommendations
After early reports of BPA, Matsubara et al.7) tried to reduce complications of BPA and reported better outcomes for CTEPH after 2012. Of the 255 patients who underwent the initial BPA procedures, 76 had reperfusion pulmonary edema, 4 of which required mechanical ventilation and one mortality was reported. After this report, they continued to try to improve the safety of BPA. First, they used low profile balloon angioplasty with a 2.0 mm diameter for patients with high mean pulmonary pressure over 40 mmHg. After several sessions of BPA for as many lesions as possible, progressively larger balloons were used for residual and selected lesions. They attained better hemodynamic outcomes and functional capacity compared to their initial report. By this methodology, complications were significantly reduced and BPA could be considered an alternative strategy for inoperable, disabled CTEPH cases. Until now BPA as for CTEPH is class IIb recommendation by 2015 guideline, it is accepted as more favorable strategy according to current expert opinion.5)11)15)16)
Recent clinical multicenter registry data in Japan showed more promising improvements in functional classes and echocardiographic parameters. A total of 308 patients (246 women; mean age 61 years) were included in this retrospective registry; patients underwent 1,408 sessions of BPA at seven institutes. Over 80% of patients showed hemodynamic improvement in which mean PAP decreased from 43.2±11.0 to 24.3±6.4 mmHg after final BPA and to 22.5±5.4 mmHg at outpatient follow-up.14) A multidisciplinary team (MDT) approach is crucial for diagnosis and treatment of CTEPH in an experienced center. Recommendations stipulate that over 50 cases of PEA and 100 sessions of BPA should be performed per year at experienced centers.15) A recent report showed that MDT approach for CTEPH has a significant influence on diagnosis, workup, and decisions regarding therapeutic modality such as PEA or BPA.9) In the post-MDT era, the implementation rates of RHC (10.8% vs. 97.6%, p<0.001) and PEA (32.4% vs. 59.5%, p<0.005) were significantly increased in conjunction with the initiation of BPA procedures.
Pulmonary angiogram, selection of patients and lesions
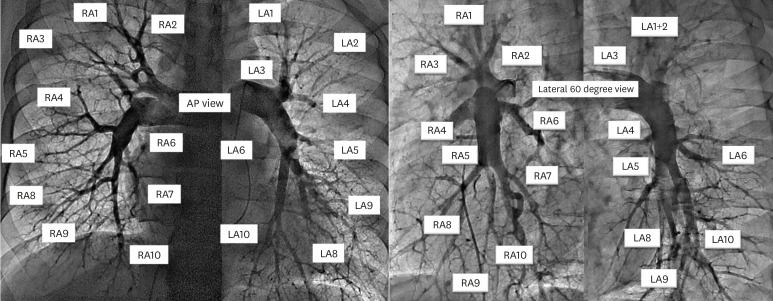
Selective pulmonary angiograms are important when diagnosing CTEPH because CT scans and lung perfusion scans cannot show clear information regarding the status of affected segmental arteries or subsegmental branches. Selective pulmonary angiogram is usually performed via biplane projection by anterior-posterior (AP) and left anterior oblique (LAO) 60-degree view with a usual coronary Judkins-right or multipurpose catheter. Comprehensive anatomy of the pulmonary artery is described in Figure 1 by AP/LAO projection. The Amplatz-left catheter is helpful for the selection of branches at the left upper and lingular segments because of its posterior to anterior projection. Because many branches should be visualized to confirm involvement by CTEPH, contrast media should be diluted with saline, especially for patients with chronic kidney disease.
Figure 1
Basic anatomy of pulmonary artery by angiogram according to projection, either posterior-anterior or left anterior oblique 60 degree.
LA = left pulmonary artery; RA = right pulmonary artery.
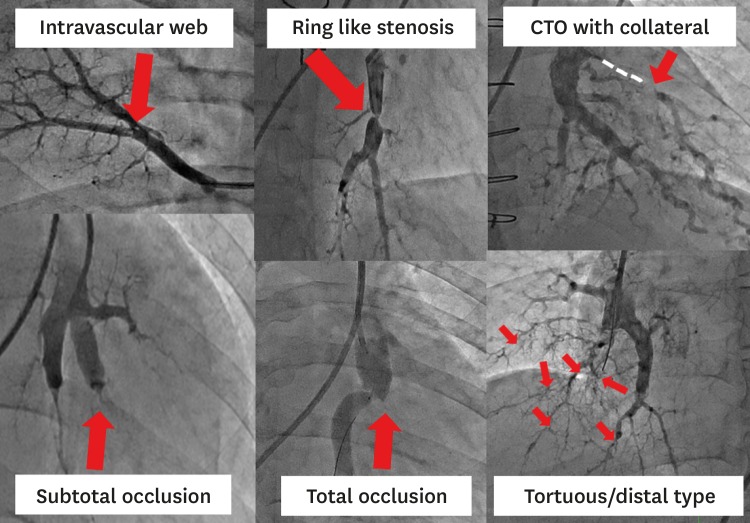
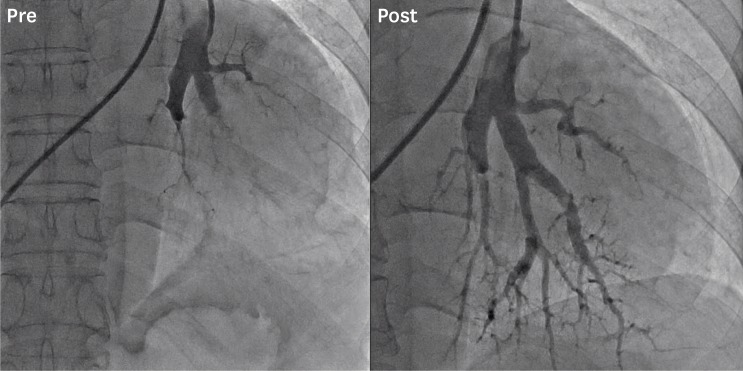
Vascular lesions in patients with CTEPH have various morphology, and some experts have suggested lesion classification according to these characteristics (Figure 2). Lesions were categorized as angiographic morphology, ring-like stenosis, intravascular web, subtotal occlusion with small channel and pouch defect, and total occlusive lesion. Lesions with chronic total occlusion also have collateral circulation from other branches. Some segments of the treated artery showed marked dilation with reduced pulmonary artery pressure after follow-up angiogram (Figure 3). The usual mechanisms of dilation are thought to be due to compression of organized thrombi by ballooning of the multi-channel lumen and formation of neointima that covers the opened luminal surface.16)
Figure 2
Classification of lesion morphology by angiogram. Various morphology types are detected by angiogram in patients with chronic thromboembolic pulmonary hypertension: intravascular web, ring-like, subtotal, and total occlusion types. CTO with collateral circulation or diffuse tortuous/distal type is also observed.
CTO = chronic total occlusion.
Peri-procedural medical therapy including anticoagulation
Patients with CTEPH have a tendency for frequent recurrent thrombosis, and it is crucial to maintain patients on anticoagulants before and after procedures. The usual maintenance medications are vitamin K antagonists. New anticoagulants (novel oral anticoagulant) showed compatible efficacy for acute pulmonary embolism; however, there is no randomized trial regarding novel anticoagulants compared to vitamin K antagonists in CTEPH.17) Anticoagulation should be sustained at international normalized ratio 2.0–3.0 with warfarin. After the first BPA session for both sides of the pulmonary artery, the second and third BPA sessions occur at intervals of one to three months depending on clinical condition. Intravenous heparinization before a procedure should be administrated in minimum amount to adjust the activated coagulation time (ACT) around 250 seconds for preventing device-related thrombosis and should then be added 500 IU regularly as an hour passes. Riociguat, a soluble guanylate cyclase agonist, is the only medical therapy approved for patients with inoperable CTEPH to improve right heart overload 18); however, it is still very expensive and is not covered by medical insurance in South Korea.
Balloon pulmonary angioplasty equipment
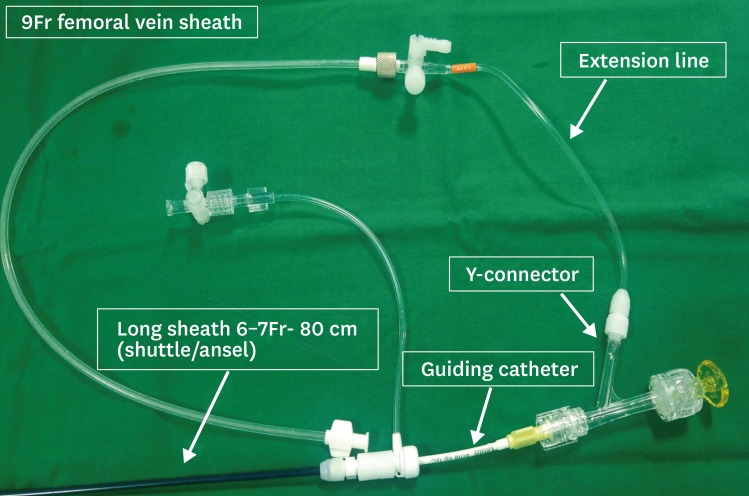
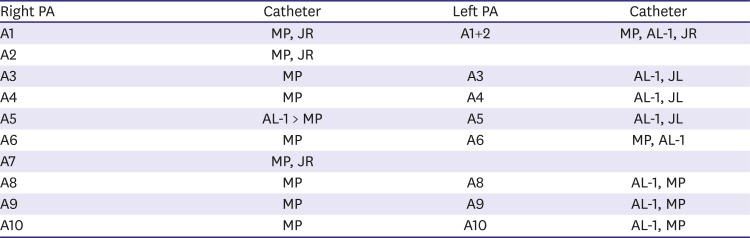
Dual long-sheath and guiding catheters are needed for BPA procedures because the stable position of the long-sheath at the main pulmonary artery provides support to guide catheter movement when selecting each segmental pulmonary artery (Figure 4). Routine 0.014 inch soft peripheral wires are acceptable for the procedure. Although dedicated wires with soft tips were introduced to support balloon passage for BPA, they cannot penetrate some hard and complete occlusive lesions. Hard and high torqueable wires should be used for tough lesions, although they may provoke vascular injury in the fragile pulmonary artery system. Appropriate diagnostic and guiding catheters vary according to the anatomy of individuals. The usual recommended catheters are listed in Table 1. As previously mentioned, balloon angioplasty is usually performed starting with a low profile catheter and progressively upsizing to a larger one according the mean pulmonary artery pressure. The first device chosen for the initial session may be a 2.0×20 mm balloon, and then balloons with up to 6-7 mm diameter can be used in the following sessions depending on lesion size. Experienced centers may start with a larger balloon in the first procedure. Even with this methodology, the complication rate can be low if a delicate procedural approach is used, especially with cases of mild to moderate pulmonary hypertension. Table 2 notes the upper limit of the balloon to external elastic membrane diameter ratio in the second dilation. Pulmonary stenting is not routinely used for angioplasty in CTEPH; however, if there is concomitant pulmonary artery stenosis or lesions that do not respond to large balloons, pulmonary stenting can be added as a salvage method in rare cases. The main target lesion should be in the segmental or subsegmental pulmonary artery. Despite a recognized correlation with pre-BPA mean pulmonary artery pressure over 40 mmHg, the extent and potential severity of reperfusion lung injury warrants anticipation of its occurrence in all patients with BPA. Mean cardiac index did not improve after BPA despite symptomatic improvement and patient survival. Balloon angioplasty began gently with a low profile 2.0 mm balloon for all possible branches. To prevent complications, right and left pulmonary arteries should be treated separately at intervals of 5–7 days. Proper wire positioning and knuckle wire techniques are required to penetrate lesions, and smaller or proportionate balloon size to the vessel is necessary to prevent perforation or bleeding. In cases with hybrid procedures after PEA, at least three months of durations for vascular healing after operation are needed to attain proper outcomes and safety compatible with the conventional procedures.
Figure 4
Sheath and guiding catheter system. Dual long-sheath and guiding catheters are needed in balloon pulmonary angioplasty procedures because the stable position of the long-sheath at the main pulmonary artery provides support to guide catheter movement in selection of each segmental pulmonary artery.

Monitoring before and after treatment, procedure complications and outcomes
Right heart catheterization (RHC) including mean pulmonary artery pressure and pulmonary vascular resistance are routine parameters used to monitor improvements in this procedure. However, changes in cardiac output or index are relatively equivocal because functional improvement in the left heart is relatively independent of right heart unloading. Echocardiography should be regularly monitored because it can impact procedural decisions and visualize structural changes in patients with CTEPH. Usual causes of pulmonary artery injury during BPA are distal vascular injury by guidewires or overdilation of stenotic lesions by mismatched balloon size.19) Although there are no randomized trials of BPA, single center or multicenter registry reports guided by various modalities are useful references for the outcomes and complications of BPA after 2012.7)14)20)21) Complications during procedures occurred in 36.3% (511 in 1408 procedures) of cases and included pulmonary injury (17.8%) and hemoptysis (14.0%).14) Wire or reperfusion-induced hemoptysis can be disastrous, and some cases even required tracheal intubation and extracorporeal membrane oxygenation. However, reperfusion-induced hemoptysis was usually mild and frequently occurred after BPA, especially in patients with high mean pulmonary artery pressure over 40 mmHg. The other minor pulmonary dissection or thrombosis occurred in some series during the procedures.
SUMMARY
BPA is a new alternative treatment option for selected patients with inoperable cases of CTEPH. There were initial reports of potentially life-threatening bleeding complications after initial reperfusion therapy with BPA. However, recently updated procedures and management techniques are relatively safe, and patients with inoperable CTEPH can approach full recovery. A multidisciplinary CTEPH team should be involved in the process of investigating and establishing PEA and BPA for treatment of this chronic disabling condition.
 XML Download
XML Download