

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The anatomical substrate for ventricular tachycardia (VT) most commonly arises in the subendocardial segments of myocardium, particularly in those patients with post-myocardial infarction (MI) scar-related reentry.1) VT circuits, however, are not exclusive to the subendocardium. In fact, up to 15% of post-infarction VT may be limited to or share areas within the subepicardial region.2) Early reports of subepicardial or intramural origin for VT date back to more than 30 years ago.3)4)5) Soon thereafter, electrophysiologists identified the presence of subepicardial VT substrate as an important cause for suboptimal success rates associated with conventional endocardial ablation.6)7) The technique of percutaneous epicardial mapping and ablation was first described 20 years ago by Sosa and colleagues8)9) in patients with Chagas' cardiomyopathy. The same group subsequently demonstrated that epicardial mapping alone did not enhance the success of endocardial ablation and that epicardial ablation, itself, was required to effectively treat patients with epicardial substrates.9)
Prior to the development of epicardial catheter ablation, patients with VT non-amenable to endocardial ablation often required surgical therapies. Over the last 2 decades, epicardial catheter ablation has been further refined and is now established as an effective strategy for epicardial VT ablation at experienced centers for treatment of both ischemic and non-ischemic substrates.1) A survey of 3 tertiary ablation centers in Europe and the U.S. between 2001 and 2007 found that nearly 1 in 5 VT ablations included epicardial mapping and/or catheter ablation.10) This paper aims to review and discuss the indications, techniques, and possible complications of epicardial catheter ablation for VT, as well as future developments in the field.
INDICATIONS FOR EPICARDIAL CATHETER ABLATION OF VENTRICULAR TACHYCARDIA
The efficacy of endocardial VT ablation ranges widely depending on the substrate. In ischemic cardiomyopathy, the success rates range from 49 to 75%.7)11)12)13)14) Patients with non-ischemic cardiomyopathy typically have a higher burden of epicardial scars and a lower success rate associated with an endocardial-only approach.14)15) It is believed that epicardial or intramural reentry circuits are likely responsible for the failure of most endocardial ablations when proper mapping is obtained.
The decision to use an epicardial approach in VT ablation requires consideration of several factors, including: 1) a prior history of unsuccessful endocardial VT ablation; 2) electrocardiographic (ECG) criteria; 3) substrate/scar localization by imaging studies; 4) the likelihood of epicardial VT in the underlying disease state; and 5) intra-procedural mapping.
Electrocardiographic identification of epicardial ventricular tachycardia
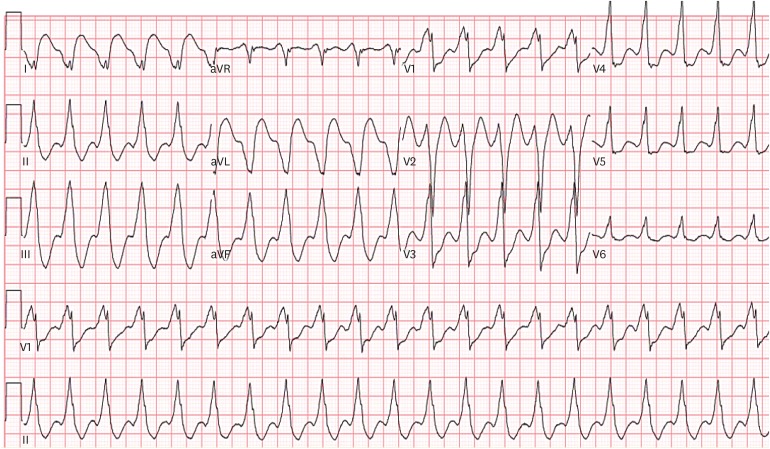
One of the early attempts to define ECG criteria for diagnosis of epicardial VT was performed by Berruezo et al.16) Patients who underwent successful endocardial VT ablation were compared to those who could not be successfully ablated endocardially. The following ECG criteria were predictive of VTs originating from the epicardium (Figure 1): 1) a pseudo-delta wave measured from the earliest ventricular activation to the earliest fast deflection in any precordial lead ≥34 msec (sensitivity, 83%; specificity, 95%); 2) an intrinsicoid deflection measured from the earliest ventricular activation to the peak of the R wave in lead V2 ≥85 msec (sensitivity, 87%; specificity, 90%); and 3) an RS complex duration of ≥121 msec (sensitivity, 76%; specificity, 85%).16) Of note, the average QRS duration was 174±37 msec in the endocardially-ablated group, which was significantly shorter than the mean QRS of 217±24 msec among those who underwent successful epicardial ablation after an initially failed endocardial attempt. Importantly, all patients with QRS duration >211 msec had an epicardial VT origin.17) Unfortunately, in an external validation cohort, none of the aforementioned criteria, including QRS duration, reliably predicted an epicardial VT origin in patients with ischemic VTs.18) Thus, these criteria appear to be more helpful in those with non-ischemic VT.
Figure 1
Electrocardiogram in patient with epicardial VT. Note the pseudo-delta wave seen in V3–V6, with duration of approximately 80 ms; an intrinsicoid deflection measuring 100 ms in V2; and an RS complex in V2 lasting 220 ms. These findings are all suggestive of epicardial VT according to Berruezo's criteria (see text for details).
VT = ventricular tachycardia.
Whereas the criteria proposed by Bazan and colleagues19)20) were established predominantly in patients with ischemic cardiomyopathy, other ECG criteria have been reported for the diagnosis of left ventricular (LV) and right ventricular (RV) epicardial VT in the absence of previous MI. Of note, ECG criteria to distinguish epicardial VT are notably region-specific, with highly variable sensitivities and specificities depending on the anatomical sites of origin.19) Vallès and colleagues21) developed and validated a 4-step algorithm to identify an epicardial VT origin arising from the basal superior and lateral LV in patients with non-ischemic cardiomyopathy with a sensitivity and specificity >90%. The algorithm includes absence of Q waves in the inferior leads with either 1) a pseudo-delta waves ≥75 msec; 2) a maximum deflection index (defined as interval from earliest ventricular activation to the peak of the largest amplitude deflection in any precordial lead divided by the QRS duration) ≥0.59; or 3) a Q wave in lead I. In patients with idiopathic LV tachycardia originating remotely from the sinus of Valsalva, a maximum deflection index of ≥0.55 has been shown to identify epicardial VT with 100% sensitivity and 99% specificity.22)
In summary, ECG criteria for discrimination of epicardial versus endocardial VT are largely substrate- and site-specific. The 4-step algorithm proposed by Vallès and colleagues21) have been shown to be highly accurate and reproducible in patients with non-ischemic cardiomyopathy and VTs originating from the basal superior and lateral perivalvular sites, whereas the criteria for ischemic cardiomyopathy and idiopathic LV tachycardias presently lack validation.
Imaging
The mechanism of VT in structurally abnormal hearts most commonly involves a reentry circuit in an area of myocardial scar. Therefore, the presence of a sub-epicardial or mid-myocardial scar detected either on contrast-enhanced computed tomography (CT) or preferably magnetic resonance imaging (MRI) can help identifying potential epicardial VT circuits. In fact, scar maps derived from contrast-enhanced MRI have been shown to correlate well with electroanatomical voltage mapping and can be used to identify an epicardial ablation site.23)24)
In a study of 29 patients with non-ischemic cardiomyopathy, delayed-enhancement MRI identified scar in 14 patients (48%). In 2 patients, most of the scar and substrates were confined to the epicardium and were consequently ablated successfully via an epicardial approach. VT ablation was unsuccessful in 5 patients with an intramural scar. The authors concluded that delayed enhancement MRI in patients without a previous infarct may help to identify the arrhythmogenic substrate and to plan the appropriate ablation strategy.25)
Similarly, intracardiac echocardiography (ICE) has a potential role in identifying epicardial scar as VT substrate. In a study of 18 patients with non-ischemic cardiomyopathy and recurrent VT, increased echogenicity on ICE showed a strong correlation with an abnormal epicardial substrate by electroanatomic mapping when examined by a blinded echocardiographer. Conversely, such areas of increased echogenicity were absent in a control group of 30 patients with structurally normal hearts.26)
Epicardial ventricular tachycardia in different cardiomyopathic disease states
Previous studies have reported a prevalence of epicardial VT ranging from 14% to 33% among patients with a previous history of MI.2)4) In a recent single-center report of 95 patients undergoing epicardial VT ablation, 35% of the patients had underlying ischemic cardiomyopathy.27) Interestingly, up to 90% of epicardial VTs in patients with ischemic cardiomyopathy are encountered following circumflex- or right coronary artery-related infarctions.2) Having said that, these numbers should be interpreted with caution, as studies have been limited by small sample sizes and the possibility of selection and referral bias should be considered.2)4)27)
In general, the prevalence of epicardial VT in patients with non-ischemic cardiomyopathies tends to be higher as compared to those with an ischemic VT substrate.15)28)29) In contrast to ischemic cardiomyopathy, patients with epicardial VT and a non-ischemic substrate typically have reentry circuits located over the basal lateral LV, in proximity to the mitral and aortic valves.28) The identification of low-voltage, wide and fractionated electrograms in these areas can assist in identifying the anatomical targets for epicardial ablation.28)
In Chagas' cardiomyopathy, the reentrant circuits causing VT can involve the subendocardial, intramural or subepicardial fibers. While an endocardial-only approach may lead to transmural injury in some patients and effectively eliminate the arrhythmia, a predominantly subepicardial circuit encountered in others may not be entirely amenable to endocardial ablation. This hypothesis led to the development of a subxiphoid approach for epicardial mapping and ablation.8) In fact, patients with Chagas' cardiomyopathy and ventricular arrhythmias typically have larger epicardial than endocardial scars, and more than one-third require an epicardial approach for successful ablation.30)31) Arrhythmogenic RV cardiomyopathy (ARVC) is a genetically-determined condition characterized by fibrofatty tissue replacement of the myocytes, particularly in the RV. In a pathological study of patients with ARVC, it was demonstrated that fatty or fibrofatty tissues occurred more extensively on the epicardial surface.32) Therefore, it is not surprising that the outcomes of endocardial ablation alone for ARVC-related VT is associated with suboptimal results. Acute procedural success and 3-year event-free survival following endocardial VT ablation in ARVC have been reported as low as 73% and 43%, respectively.33) On the other hand, combined endocardial-epicardial mapping and ablation in 13 patients with ARVC who had previously failed an endocardial ablation resulted in no recurrent VT in 10 (77%) patients during a mean follow-up of 18±13 months.34) In addition, the areas of low-voltage electrograms were significantly greater on the epicardium (95±47 cm2) as compared to the endocardium (38±32 cm2), which underscores the importance of an epicardial approach in this patient population.34)
In a more recent study, combined endocardial-epicardial VT ablation with scar dechanneling in 11 patients with ARVC was associated with recurrence in only 1 patient after a median follow-up of 11 months.35) A meta-analysis of combined endocardial-epicardial ablation in 26 ARVC patients versus an endocardial-alone approach in 23 ARVC patients found significantly higher freedom from recurrent ventricular arrhythmias or implantable cardioverter defibrillator (ICD) therapies (84.6% vs. 52.2%) and elimination of anti-arrhythmic therapy (69.2% vs. 21.7%) in the endocardial-epicardial ablation group after more than 3 years of follow-up.36)
In a study of 20 patients with biopsy-proven viral myocarditis and drug-refractory VT, 6 (30%) could not be ablated using an endocardial-only approach and required epicardial ablation to successfully abolish the clinical VTs.37)
In a small case series of 8 patients with cardiac sarcoidosis referred for ablation, 2 patients underwent epicardial mapping and ablation after an endocardial-only approach failed to abolish VT.38) Similarly, a systematic review of 5 studies and 83 patients with cardiac sarcoidosis undergoing VT ablation found that 18% of the patients required epicardial ablation.39) Importantly, however, due to scar multifocality characteristics of cardiac sarcoidosis, the average number of VTs per patient is approximately 4.38)39) Therefore, other inducible VTs can persist despite successful ablation of the clinical tachycardia. The freedom from recurrent sustained VT is 50% at best, and approximately 25% of patients require a second ablation procedure.38)39)
A recent systematic review of ablation strategies for patients with Brugada syndrome including 233 individuals found that among those who underwent both endocardial and epicardial mapping, there was no identifiable endocardial substrate in 93% of cases. Furthermore, elimination of type I Brugada pattern on electrocardiogram was approximately 98% and 35% with and without an epicardial approach, respectively. Freedom from recurrent VT or ventricular fibrillation (VF) was 97% and 71% with epicardial versus endocardial-only ablation, respectively.40)
EPICARDIAL ACCESS
Subxiphoid percutaneous access
Access to the epicardial surface of the myocardium can be achieved via the coronary sinus. However, such an access is significantly limited by the anatomy of the coronary sinus vein and its tributaries. In order to gain unlimited access to the epicardium, a subxiphoid percutaneous approach is often necessary to guide epicardial ablation. This technique is somewhat similar to the traditional subxiphoid access utilized for pericardiocentesis, albeit in the presence of minimal to no pericardial fluid as opposed to a supraphysiologic volume expansion in the abnormal setting of pericardial effusion.
Two strategies are currently available for gaining epicardial access through a subxiphoid percutaneous approach. The traditional method was reported by Sosa et al.8) in their original description of epicardial VT ablation. This technique utilizes a 17- or 18-gauge, 6-inch Tuohy needle which is somewhat ‘blunt’ with a beveled tip. The Tuohy needle was developed for access into the epidural space which is thought to be a virtual space.41) As such, its specific design aims to reduce the risk of vascular or myocardial injury.10) Briefly, the needle is inserted along the left border of the subxiphoid process and advanced toward the left shoulder under fluoroscopic guidance. The angle of entry is adjusted accordingly to achieve an anterior or posterior puncture. As the needle is advanced, small amounts of contrast are injected to visualize the tip of the needle until entry into the pericardial space has been confirmed. Then, a long guidewire is advanced fluoroscopically into the pericardium, followed by a sheath over the wire. Ultimately, a mapping or ablation catheter can be positioned inside the pericardial space through a long introducer sheath.
More recently, a ‘needle-in-needle’ technique for epicardial access has been described.42) In this approach, a 7-cm 18-gauge needle is inserted beneath the sternum. The purpose of this short needle is to provide stability and tactile feedback for a longer (15- or 20-cm) micropuncture 21-gauge needle, which is inserted through the 18-gauge needle. Once the 21-gauge needle is inserted into the pericardial space, a long 0.018-inch guidewire with a floppy tip is advanced into the pericardial space. Upon fluoroscopic confirmation that the guidewire has been inserted into the pericardium both needles are then removed. Micropuncture dilators are then used to upsize the guidewire to a 0.35-inch wire and ultimately, an 8-Fr sheath is introduced into the pericardial space. The ‘needle-in-needle’ technique was compared in 23 prospective cases to 316 retrospective procedures using the Sosa technique. Successful epicardial access was achieved in 100% of the ‘needle-in-needle’ cases, as compared to 94% with the Sosa technique. Major pericardial bleeding was similar between both techniques (8.7% in the ‘needle-in-needle’ versus 8.9% in the Sosa approach).42)
Surgical access
Percutaneous subxiphoid access may not be feasible in patients with pericardial adhesions. In these patients, a limited surgical thoracotomy may be required to gain access to the pericardium. This technique involves a small subxiphoid incision, followed by manual lysis of adhesions and exposure of the epicardial surface. An introducer sheath is then placed into the pericardial space under direct visualization.43) This technique should be strongly considered in patients with a prior history of cardiac surgery which typically leads to dense pericardial adhesions, anatomical distortion and a greater potential for catastrophic complications associated with conventional percutaneous access.44)
EPICARDIAL VENTRICULAR TACHYCARDIA ABLATION
Energy sources
Radiofrequency
The electrophysiological principles that guide epicardial VT ablation are similar to those of endocardial ablation. Some nuances of epicardial ablation, however, should be emphasized. First, the convective cooling provided by blood flow in endocardial ablations is not present in the epicardium. As a result, when radiofrequency (RF) is used as the energy source for ablation, irrigation is only required to prevent premature heating of the catheter tip which can otherwise limit the delivery of sufficient RF energy. On the other hand, thrombus formation is not so much of a concern during epicardial ablation. Irrigated ablation is generally preferred over standard RF, as the former has been shown to create larger and deeper epicardial lesions particularly in areas covered by epicardial fat.45)
In a recent study of ex vivo and in vivo animal models, RF applications with reduced irrigation rates (5–7 mL/min) resulted in similar lesion sizes as those created by conventional (higher) flow rates (≥10 mL/min), without an increase in steam pop or tissue disruption. Meanwhile, presence of intra-pericardial fluid was associated with significant reductions in lesion diameter, depth and volume.46) Altogether, these findings suggest that reduced irrigation rates (5–7 mL/min) and a relatively ‘dry’ pericardial space is preferred when performing irrigated epicardial RF ablation.
The use of contact-force and its limitations
The development of contact-force (CF) sensing catheters has had important implications in the field of epicardial VT ablation. In animal models, 1 in 5 RF applications in the absence of CF-sensing technology do not result in tissue lesions; as such, the addition of CF can significantly improve lesion formation, both endocardially and epicardially.47) Further, excessive CF has been associated with steam pops, acute coronary arterial damage and phrenic nerve injury.48) The optimal tissue CF required for epicardial mapping and ablation has not yet been conclusively established. Based on linear mixed model analysis, 4 g of force has been proposed as the best cutoff value in order to obtain normal signal amplitude (>1.5 mV) in the epicardium.49)
Additionally, adequate vector orientation seems to play a pivotal role in the delivery of RF energy and catheter ablation. In a study including 4,155 epicardial mapping points, adequate catheter orientation, defined as a vector directed toward the myocardium, was present in only 46% of points. In the apical and basal LV, more than 2/3 of the vectors were not directed inward toward the myocardium. This is in sharp contrast to a 94% rate of adequate vector orientation in 4,824 endocardial mapping points.49) Meanwhile, the median CF of adequate vector orientation was 15, 13 and 8 g for the LV endocardium, RV endocardium and epicardium, respectively. Altogether, these findings indicate that endocardial ablation relies more on adequate CF, whereas epicardial mapping and ablation are more dependent on adequate catheter orientation. In fact, the 2-fold increase in CF with inadequate vector orientation in epicardial mapping suggests that higher CF in the epicardium may redirect the catheter away from an axial myocardial direction, potentially increasing the risk of collateral injury to extracardiac structures.47)49) The tendency for a non-axial vector orientation and higher CF exerted laterally during epicardial catheter ablation may also provide an explanation for the wider and shallower RF lesions typically seen with epicardial versus endocardial ablation.47)
Cryoablation
Although RF is the predominant energy source used for epicardial VT ablation, cryoablation can be used as an alternative modality. In vivo animal studies have demonstrated that cryoablation can produce lesions on the epicardium with similar size and depth as those created on the endocardium.50) In a report of all patients undergoing epicardial VT ablations in 3 tertiary care centers, cryoablation was used in 11 of 156 (7%) procedures mainly due to concerns regarding the close proximity of the ablation site to the epicardial arteries.10) However, Lustgarten and colleagues51) showed that cryoablation can also create injury to epicardial vessels by promoting intense neointimal proliferation. Head-to-head comparisons of RF versus cryo-energy for epicardial VT ablation are presently lacking.
Epicardial fat
The presence of epicardial fat is another crucial difference between epicardial and endocardial VT ablation with two main implications. First, a layer of epicardial fat >5 mm can in part mimic scar. Second, epicardial fat can insulate the myocardium and significantly reduce the effectiveness of energy delivery, particularly that of RF.
Prior studies have demonstrated that an epicardial fat thickness of <5 mm does not significantly influence the pacing threshold, peak-to-peak bipolar voltage amplitude or bipolar electrogram duration as compared to areas without epicardial fat.52)53) In contrast, presence of thick epicardial fat (>5 mm) can considerably decrease peak-to-peak electrogram amplitude and prevent ventricular pacing capture even at higher outputs (i.e., 10 mA).52) In a study of 59 patients undergoing coronary artery CT, the mean pericardial fat thickness was reported as 5.3±1.6 cm.54) Several factors are associated with the increased thickness of epicardial fat, including advanced age,54)55) female gender,54) heart weight,55) body mass index,55) waist circumference,55) and presence of coronary artery disease.55)56)
Fat is also significantly thicker in the regions of the atrioventricular groove and RV anterior free wall, whereas the LV lateral wall tends to have little epicardial fat.54) As mentioned, thick epicardial fat can produce electrogram morphologies similar to that of scar tissue, particularly decreased voltage amplitude. However, fractionated electrograms with prolonged duration typically do not occur as a consequence of epicardial fat alone. Hence, this can be especially helpful when discriminating true scar from areas of low voltage encountered in the presence of epicardial fat.57)
Thick epicardial fat can also prevent the effective delivery of RF energy to the underlying myocardium. There is a significantly higher thickness of pericardial fat in patients with failed (16.9±6.8 mm) versus successful (1.5±2.1 mm) epicardial VT ablation.58) In an in vitro model, epicardial fat has been shown to severely limit lesion transmurality with conductive heating sources, particularly RF.59) In an in vivo model, non-irrigated RF was unable to produce appreciable lesions in areas covered by epicardial fat (3.1±1.2 mm thick). In contrast, irrigated RF produced 4.1±2 mm deep lesions in presence of epicardial fat.45) Other studies have also shown RF ablations to be ineffective in presence of epicardial fat measuring ≥10 mm thick.60)
COMPLICATIONS
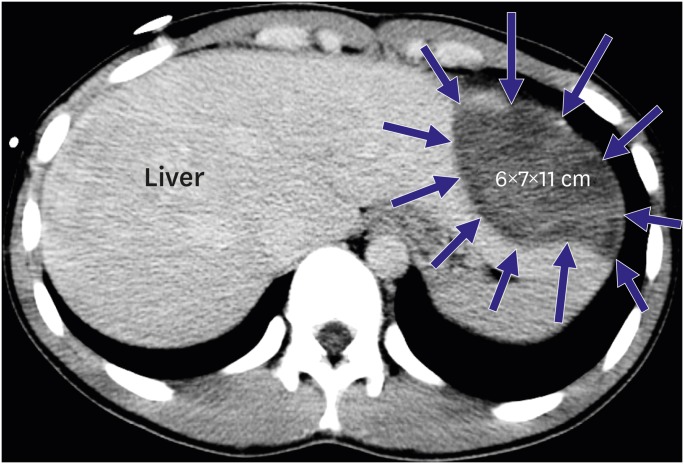
Percutaneous epicardial access and ablation can result in collateral injury to several thoracic and abdominal structures, including the epicardial vessels, the RV, the pleura, the lungs, the phrenic nerve, the diaphragm and the liver (Figure 2). In addition, a detailed medical and surgical history is necessary to assess for the possibility of pericardial adhesions. Prompt access to echocardiography, blood bank and cardiothoracic surgery should also be made available.
Figure 2
Liver puncture during epicardial access attempt, resulting in a subcapsular hematoma in the left hepatic lobe. Reproduced with permission from Koruth et al.44)
The most common complication of epicardial ablation is pericarditis, which has been reported in up to 30% of patients who undergo this procedure.61) In a study of 218 patients who underwent epicardial VT ablation, severe postprocedural precordial pain occurred in 23 (11%) patients.29) The majority of these cases can be successfully treated with conservative management including anti-inflammatory agents. Of note, constrictive pericarditis requiring surgical intervention has been reported in one patient with ARVC and multiple epicardial VT ablations.62) Strategies to prevent procedure-related pericarditis include routine use of systemic non-steroidal anti-inflammatory drugs and intrapericardial corticosteroids. The latter has been shown to prevent post-procedural inflammation and adhesion formation in animal models.63)
It should be emphasized that major complications can occur in approximately 5% of epicardial VT ablations.10)29) As previously mentioned, the curved tip of the Tuohy needle tends to mitigate the risk of RV puncture during subxiphoid percutaneous access. Nevertheless, hemo-pericardium remains the most common serious complication of this procedure.10) Inadvertent, uncomplicated RV puncture is reported in up to 17% of the cases.10) Moreover, the timing of bleeding with respect to the procedure can be particularly helpful in identifying the etiology of hemo-pericardium.
When bleeding occurs early after subcutaneous subxiphoid access, it is usually related to an accidental RV puncture, disruption of adhesions or an inadvertent puncture of an epicardial vessel. While the first two are often self-limiting, the presence of continuous, bright-red bleeding typically suggests injury to an epicardial artery and generally requires percutaneous coronary intervention and sometimes surgical repair. On the other hand, bleeding that is first detected during epicardial ablation is typically the result of an epicardial steam pop or a dry RV puncture that once again blossoms with the onset of systemic anticoagulation. In contrast, the onset of bleeding at the end of the procedure may imply a double RV puncture. In this rare complication, access to the pericardial space is gained through a sequential entry and exit puncture within the RV. Bleeding can potentially go unnoticed throughout the entire procedure until the catheter and the introducer sheath are removed, at which point brisk intra-pericardial bleeding ensues. Torrential intra-pericardial bleeding requiring emergent surgical intervention is the rule. Lastly, delayed bleeding can be observed in patients who develop post-procedural pericarditis or Dressler's syndrome while receiving systemic anticoagulation.
Several precautions should be undertaken to mitigate the risk of procedural complications when performing epicardial ablation. Pre-ablation coronary angiography is required to identify the proximity between the ablation site and the major epicardial vessels. In swine models, RF lesions delivered in close proximity (<1 mm) to epicardial coronary arteries causes acute and chronic intimal and medial thickening, as well as replacement of extracellular matrix with smooth muscle.64) Previous guidelines have recommended to maintain a minimum distance of 5 mm between the ablation catheter tip and a major coronary vessel.65) Furthermore, the extent of arterial damage by RF ablation is inversely proportional to the vessel's internal diameter.66)
Phrenic nerve injury, although rare (<1%), has also been reported in patients undergoing epicardial VT ablation.29)67) When the ablation site is felt to be in close proximity to the left phrenic nerve (usually along the lateral LV wall), high output pacing for phrenic nerve mapping must be performed prior to RF ablation in order to prevent collateral injury.29)68) The introduction of air and saline in steps of 20 mL into the pericardial space until hypotension or loss of phrenic nerve pacing capture appears to be the best strategy to prevent phrenic nerve injury during epicardial ablation.68)
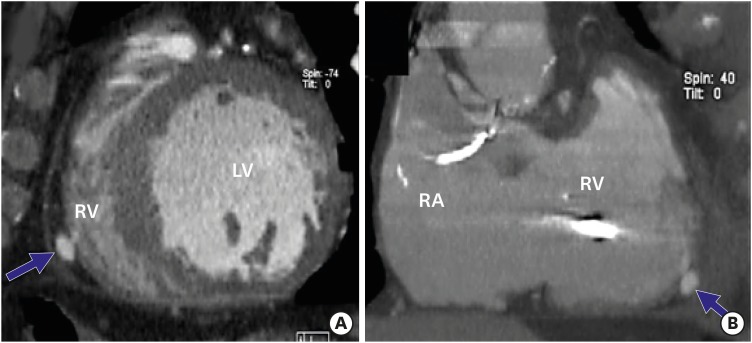
Other unusual complications of epicardial ablations include hepatic injury leading to hemoperitoneum or subcapsular hematoma, pseudoaneurysm and fistulas involving the RV (Figure 3), and coronary vasospasm.44) A case of pleuropericardial fistula with post-procedural left pleural effusion has also been reported in the literature.69)
Figure 3
RV pseudoaneurysm presenting with persistent chest discomfort 1 month after epicardial ventricular tachycardia ablation. The patient was deemed to have prohibitive surgical risk, and the pseudoaneurysm resolved on repeat imaging studies. Reproduced with permission from Koruth et al.44)
LV = left ventricular; RA = right atrium; RV = right ventricular.
Lastly, repeat epicardial access has been shown to be feasible, if necessary. In a study of 30 patients undergoing repeat epicardial mapping and ablation, significant adhesions were encountered in 7 (23%) patients, despite the use of epicardial corticosteroids during the index procedure. The adhesions limited mapping in 2 patients, whereas blunt dissection with an ablation catheter allowed for complete mapping in the remaining 5 individuals.70)
CONCLUSIONS
In summary, the development of percutaneous epicardial mapping and ablation over the last 2 decades has established this approach as a non-surgical therapeutic alternative for patients with subepicardial VT. Though the efficacy varies significantly for different VT substrates, the technique overall seems more applicable in those with non-ischemic cardiomyopathy as compared to ischemic substrate. Patients who fail an endocardial ablation and/or have ECG or imaging evidence of a subepicardial VT substrate should be considered for epicardial mapping and ablation. Operators must consider the potential impact of thick epicardial fat measuring >5 mm which can mimic low-voltage scar and drastically reduce RF energy delivery to the tissue. While up to one-third of patients may develop uncomplicated post-procedural pericarditis, the risk of serious complications such as hemopericardium and coronary or phrenic nerve injury can be reduced through careful planning.
 XML Download
XML Download