

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In the last 3 decades the combination of office and out-of-office (i.e., ambulatory or home) blood pressure (BP) measurements has achieved increasing diffusion and diagnostic relevance as it provides a more comprehensive and precise assessment of cardiovascular (CV) risk related to BP alterations in the general population.1) This modern approach allows to define 4 BP patterns, namely true normotension (normal office and out-of-office BP), white coat hypertension (WCH) or isolated clinic hypertension (elevated office and normal out-of-office BP), the reverse pattern alternatively defined as masked hypertension (MH), (normal office and elevated out-of-office BP) and sustained hypertension (elevated in-office and out-of-office BP).2)
These 4 BP patterns have been shown to differ in terms of prevalence, demographic/clinical and metabolic features, association with subclinical target organ damage and exposure to the risk of CV morbidity and mortality. Starting from the report by Pickering et al.3) published in 1988 increasing attention has been given to WCH a condition in which the detection of hypertension by office measurements is not confirmed by home and/or ambulatory BP monitoring (ABPM). In that pioneering study, approximately twenty percent of 292 patients with untreated hypertension were found to have normal day-time ambulatory pressures and were defined, for the first time, as having WCH. Compared to individuals with elevated office and ambulatory BP those with WCH were younger, more recently diagnosed with hypertension, likely to have a lower prevalence of overweight/obesity. After thirty years of clinical research many unresolved problems and controversies still remain about the clinical and prognostic significance of the WCH and, more importantly, on its optimal clinical management.
This article will examine some relevant issues concerning WCH by focusing in particular on: 1) diagnostic criteria, prevalence and clinical characteristics, 2) relationship with subclinical target organ damage, 3) prognostic significance, 4) therapeutic perspectives. It is worth mentioning that many of the data discussed in this review are based on the results generated by the Pressioni Arteriose Monitorate E Loro Associazioni (PAMELA) study. The main features of this population-based observational project can be briefly summarized as follows. The PAMELA study started in 1990–1991 and was carried out in 3,200 individuals aged between 25 and 74 years, randomly selected from the residents in Monza (a town near Milan, Italy).4) Participation rate was 64%, thus complete baseline data were collected in 2,051 subjects. After their informed consent had been obtained during the initial visit, all participants underwent the following procedures: medical history and physical examination, 3 sphygmomanometric BP measurements in the sitting position, blood and urine sampling, standard 12-lead electrocardiogram and echocardiogram. On the same day, all subjects were fitted with an ABPM device. In addition, each individual was given a validated semi-automatic device for BP measuring at home. Seventy percent of subjects enrolled in the original study accepted to repeat the same measurements 10 years later. Moreover, the number of fatal and non-fatal CV events (stroke, myocardial infarction and heart failure) and all-cause mortality was recorded during a follow-up ranging from 148 to 192 months.
PREVALENCE AND CORRELATES
Based on data from European, Australian, and Asian populations it has been shown that an office BP of 140/90 mmHg corresponds to home BP values of 135/85 mmHg and to ABPM values defined as a daytime systolic BP/diastolic BP of 135/85 mmHg, a night-time systolic BP/ diastolic BP of 120/70 mmHg, and a 24-hour systolic BP/diastolic BP of 130/80 mmHg.5) Definition of WCH relies on elevated office BP (>140 mmHg systolic BP and/or >90 mmHg diastolic BP) during repeated visits concomitant with out-of-office BP values below the accepted thresholds for ambulatory hypertension (i.e., mean day-time systolic BP/diastolic BP <135 and <85 mmHg or mean 24-hour BP below 130/80 mmHg) or home hypertension (i.e., <135/85 mmHg). Due to the clinical and prognostic relevance of nocturnal BP, the 2013 European Society of Hypertension (ESH) position paper proposed that WCH diagnosis should be based on office readings above 140/90 mmHg and mean 24-hour BP below 130/80 mmHg, thereby incorporating nocturnal BP values in the definition.6) In the PAMELA study 24-hour BP and home BP normality were defined as <125/79 mmHg and <132/83 mmHg, respectively. These values are similar or somewhat lower than the normality values for 24-hour and home BP reported by guidelines.
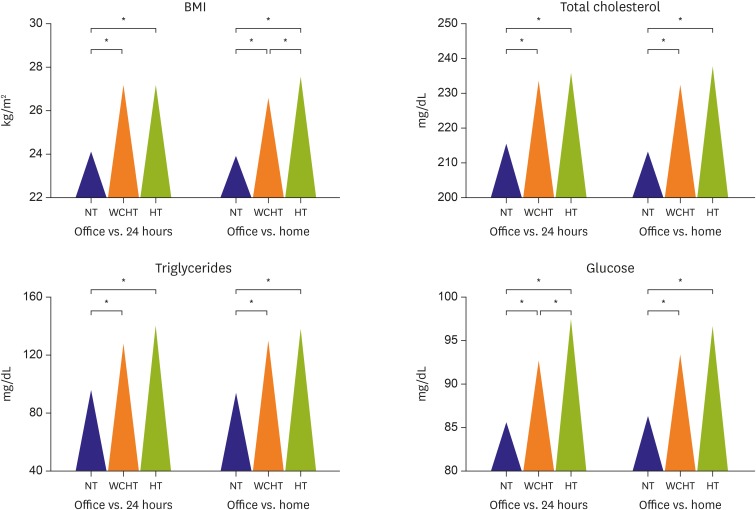
The prevalence of WCH varies widely in relation to the demographic and clinical characteristics of the populations analyzed and to the methods used to measure BP (i.e., routine office measurement of BP by clinician observers versus unattended BP measurements). In the PAMELA population WCH prevalence ranged from 9% to 12%, depending on whether out-of-office normotension was defined by home BP (<132/83 mmHg) or 24-hour ABPM (<125/79 mmHg), respectively.7) WCH participants were likely to have a more frequent history of CV events and a greater body mass index (BMI), serum total cholesterol, serum triglycerides and serum glucose values than normotensive controls (Figure 1).7) Furthermore, and more importantly, 24-hour and home BP values, although falling within the normal range, were significantly and not marginally greater (24-hour systolic BP +7 mmHg, diastolic BP +4 mmHg; home systolic BP +17 mmHg diastolic BP +9 mmHg) in the WCH than in the normotensive group. These observations are in line with the findings provided by individual studies and meta-analyses showing that compared with normotensive controls subjects with WCH exhibit 1) a higher prevalence of overweight or obesity, dyslipidemia, diabetes mellitus, or an impaired fasting plasma glucose state than normotensive controls, and 2) an increased risk of developing true hypertension or diabetes mellitus, and asymptomatic organ damage with documented prognostic significance.8)9)
Figure 1
Mean values of (A) BMI, (B) total cholesterol, (C) plasma triglycerides and (D) glucose in NT, WCHT and in established HT recruited in the PAMELA study. The progressive and significant increase in anthropometric and metabolic variables was evident both when the blood pressure data were analyzed as office vs. 24 hours and as office vs. home.7)
HT = hypertensives; NT = normotensives; PAMELA = Pressioni Arteriose Monitorate E Loro Associazioni; WCHT = white coat hypertensives.
*Refer to the statistical significance (p<0.01) of the values recorded in the different groups.
Clinical surveys performed in individuals attending out-patient hypertension centres have reported that WCH can vary from 15 to 30–40%. In a selected sample of untreated 2,209 individuals who underwent full BP assessment at a specialist unit Tocci et al.10) found that the prevalence of WCH was 16%. Compared to normotensives, WCH subjects had a greater BMI and female prevalence. The prevalence and associated conditions of WCH defined on the basis of the normality of all day-time, night-time, and 24-hour BP, only day-time, or only 24-hour BP was assessed by the Investigators of Spanish Ambulatory Blood Pressure Monitoring Registry in 115, 708 patients (45,020 untreated and 70, 688 treated).11) WCH was estimated in patients with elevated office BP (≥140 and/or 90 mmHg) by using normal day-time (<135/85 mmHg) BP, normal 24-hour BP (<130/80 mmHg), or normal day-time, night-time (<120/70 mmHg) and 24-hour BP. Prevalence of WCH was 41.3%, 35.2%, and 26.1% in untreated, and 45.8%, 38.9%, and 27.2% in treated patients with elevated office BP, by using the criteria of day-time, 24-hour BP, or all ambulatory periods, respectively. Of note, compared with the normotensive group, WCH with a fully normal out-of-office (i.e., normal daytime, night-time, and 24-hour BP) did not significantly differ in terms of other CV risk factors or organ damage. In contrast, patients from other groups (either only normal daytime BP or 24-hour BP) had significantly more prevalence of diabetes, dyslipidemia, microalbuminuria, LVH, impaired renal function, and prior history of CV disease.
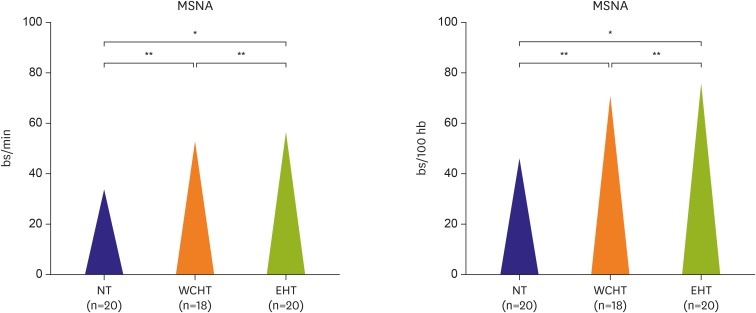
As compared with normotensive individuals, a higher frequency of metabolic alterations (i.e., impaired glucose tolerance, type diabetes, dyslipidemia and metabolic syndrome) has been documented in subjects with WCH in a number of cross-sectional studies and less frequently in long-term longitudinal study.12) In the PAMELA population, the increase in plasma glucose levels and incidence of new-onset diabetes (plasma glucose ≥126 mg/dL or use of antidiabetic drugs) among 1,412 participants over a 10-year period, was significantly greater in individuals with WCH than in normotensives (age and sex-adjusted risk of 2.9).13) Along with the above mentioned alterations WCH is associated with a marked activation of the sympathetic nervous system (Figure 2),14) which may be favor, together with other factors, the occurrence of the above mentioned dysmetabolic alterations and target organ damage as well (see below).15)
Figure 2
Mean values of MSNA uncorrected (A) or corrected (B) for heart rate in NT and in patients with WCHT and EHT.14)
EHT = established hypertensives; MSNA = muscle sympathetic nerve traffic; NT = normotensives; WCH = white coat hypertensives.
*,†Refer to the statistical significance (*p<0.05, †p<0.01) of the values recorded in the different groups.
Scanty information, however, is available on the value of WCH in predicting the long-term incidence of a cluster of metabolic alterations such as the metabolic syndrome in the general population. To the best of our knowledge, the PAMELA study is the first population-based survey providing data about the value of abnormal BP patterns determined by office, home and 24-hour measurements in predicting the development of metabolic syndrome.16) In this 10-year prospective follow-up study compared to subjects with in- and out-of-office normal BP, a greater incidence of new onset age- and gender-adjusted Mets was observed in WCH, when out-of-office BP was defined by ambulatory criteria. Similar findings were observed when out-of-office BP was defined by home criteria.
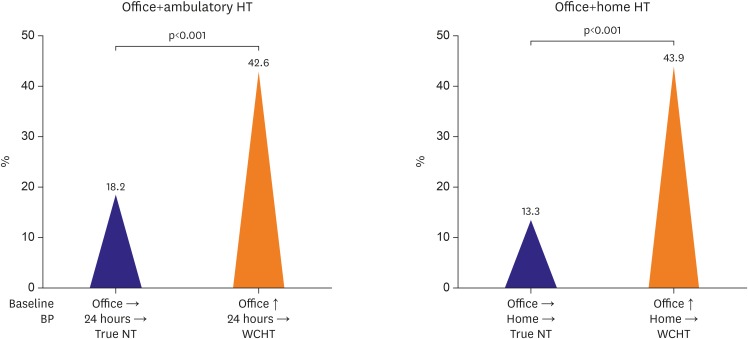
It is largely debated whether WCH is a condition at greater risk of developing a sustained hypertensive state.17) This important issue was examined in 1,412 untreated subjects belonging to the PAMELA population.18) At the first examination, 758 (54.1%), 225 (16.1%), and 293 (20.9%) subjects were classified according to office and ABPM criteria as normotensive, WCH and sustained hypertensives, respectively. At the second examination ten year later, 136 normotensives (18.2%) and 95 WCH (42.6%), subjects became sustained hypertensives (Figure 3A). As compared with normotensives, adjusting for age and sex, the risk of becoming hypertensives was significantly higher for WCH subjects (p<0.0001). Similar results were obtained when the definition of the various conditions was based on home BP (Figure 3B). Independent contributors of worsening of hypertension status were not only baseline BP, but also, although to a lesser extent, metabolic variables and age.
Figure 3
Incidence of “new” hypertension in NT and in patients with WCHT, defined by 24-hour (A) or home (B) in the PAMELA study. p<0.01 between values observed in the 2 different groups.18)
NT = normotensives; PAMELA = Pressioni Arteriose Monitorate E Loro Associazioni; WCHT = white coat hypertensives.
Finally, it worth noting that most of the studies targeting WCH defined this condition based on a single ABPM recording. Although more reproducible than office BP measurement, 24-hour BP monitoring has an intrinsic variability between recording sessions depending on numerous factors including the degree of physical activity, quality of sleep, work stress, seasonal variations and changes in eating habits. Obviously, this variability affects average ABP levels and the consistency of WCH classification over time.19) We investigated the short-term WCH reproducibility by performing two 24-hour ABPMs at 1–4 week interval in 650 untreated hypertensives.20) In approximately 50% of patients defined as WCH at first ABPM, average day-time BP values at the second ABPM were >135 mmHg systolic or 85 mmHg diastolic, thus shifting them into the category of sustained hypertensives.
TARGET ORGAN DAMAGE
The extent of subclinical organ damage (i.e., left ventricular hypertrophy [LVH], carotid atherosclerosis, microalbuminuria and retinopathy) in WCH has been reported to be similar as in normotensive subjects by some investigators, but as severe as in sustained hypertensives by others.21) Among the manifestations of hypertensive organ damage, most attention has been devoted to LVH, because of the high prevalence of this phenotype and the associated increased risk of CV morbidity and mortality.22) LVH reflects the long-term exposure of the heart to pressure overload and may identify individuals more exposed to the adverse effects of high BP.
A number of echocardiographic studies performed in different clinical settings (i.e., hypertension clinics, primary care, pediatric setting and population-based cohorts) assessed the association between WCH and subclinical cardiac abnormalities. The first study addressing this topic including a total of 143 patients with newly diagnosed mild-to-moderate hypertension (53 with intracranial hemorrhage (ICH) as defined by day-time ambulatory DBP <90 mmHg), was carried out by Høegholm et al.23) They found that subjects with WCH had a significantly lower left ventricular (LV) mass index than those with sustained hypertension (94±23 g/m2 versus 102±27 g/m2, p=0.04). This was also the case for LV relative wall thickness, an index of LV concentric geometry. Of note, LV geometry and structure was normal in up to 83% of WCH subjects as compared to 61% sustained hypertensives. Left atrial diameter was not different between the groups. In a multiple regression model, ambulatory BP values but not office BP values were significantly associated with LV mass index.
In the PAMELA population, LV mass index and wall thickness (septal plus posterior wall thickness) at baseline evaluation had a substantially normal distribution, with values lower in women and progressively greater with aging.7) In subjects with WCH, LV mass index and wall thickness were on average lower than in hypertensives with both elevated office and ambulatory or home monitoring but higher (+9%) than in normotensives with normal office, ambulatory or home BP values. Similar findings were obtained when data were separately analyzed in men and women and adjusted for age. Furthermore, in WCH individuals LVH was less frequent (15–18%) than in subjects with both office and 24-hour hypertension (23–26%) but more frequent than in sustained normotensives (4%).
A recent meta-analysis of our group including 7,382 untreated subjects (2,493 normotensive, 1,705 WCH, and 3,184 hypertensive individuals) of both genders from 25 studies provided a comprehensive and updated information on the presence and extent of subclinical structural and functional cardiac damage, as assessed by echocardiography, in subjects with WCH.24) Mean LV mass index was lowest in normotensive (88.05±2.5 g/m2), intermediate in WCH (95.72±1.8 g/m2) and highest (109.2±2.5 g/m2) in sustained hypertensive subjects. As for LV diastolic function, as assessed by the ratio of early (E) to late (A) peak of mitral inflow velocity (E/A ratio) the average value from pooled data of 8 studies was 1.17±0.07 in normotensive, 1.07±0.07 in WCH and 0.99±0.11 in sustained hypertensive subjects. Left atrium diameter was greater in WCH than in normotensive and in sustained hypertensive than in WCH subjects. All differences were significant and unaffected by publication bias or single study effect. Finally, a meta-regression analysis performed on data from all WCH showed a direct correlation between office systolic BP and LV mass index; this was not the case for day-time systolic BP.
Hypertension has been demonstrated to be the major risk factor for carotid structural changes such as intima-media thickening and plaque progression, due to the combined impact of mechanical stress on the arterial wall and of growth/inflammatory factors operating in hypertension.25)26) Although a significant increase in intima-media thickness (IMT) has been described in patients with various degrees of hypertension compared with age-matched normotensive controls, few studies have addressed this issue in WCH. Thus, we recently performed a meta-analysis of with the primary aim to increase the level of evidence in this research area. A total of 3,478 untreated subjects, 940 normotensive (48% men), 666 WCH (48% men), and 1,872 hypertensive individuals (57% men) included in 10 studies were analyzed.27) Common carotid IMT showed a progressive increase from normotensive to WCH and to hypertensive subjects IMT. After assessing data for publication bias, only the difference between normotensive and WCH subjects persisted to be significant. On the whole, available literature based on recent individual studies and meta-analyse supports the view that cardiac and vascular structural/functional alterations in in WCH subjects, are intermediate between sustained hypertensives and normotensive controls. This finding suggests that WCH may not be entirely harmless on clinical grounds.
PROGNOSTIC SIGNIFICANCE
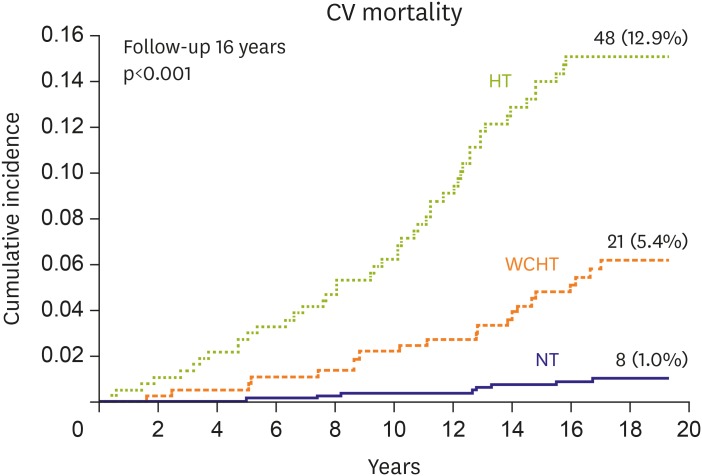
Until little more than 10 years ago the evidence regarding the relationship between WCH and incident CV disease and/or mortality was largely confined to a few studies based on ambulatory BP in populations with selected ages, limited follow-up periods, and variable definitions of ambulatory BP normality over 24 hours or the day only. The prognostic value of WCH in the PAMELA study was assessed over a long observational period in a general population rather than in selected cohorts of subjects, as in most previous studies.28) The incidence and risk of CV death showed a progressive increase from subjects in which in-office and out-of-office BPs were both normal to subjects with WCH and in-office and “out-of-office” hypertension, independent of age and gender (Figure 4). Second, the progressive increase in mortality from the entirely normotensive to the entirely hypertensive group occurred regardless of whether the above conditions were identified based on office versus ambulatory or office versus home BP. The trend remained significant also after further adjustment for history of CV disease, smoking, serum cholesterol, and blood glucose. In WCH subjects the gender-adjusted hazard ratio (HR) for CV and all-cause mortality amounted to 1.76 (p=0.002).
Figure 4
Kaplan-Meier curves for CV mortality in NT, WCH, and sustained HT. WCH was defined by an office BP elevation and ambulatory (24 hours) or home BP normality. NT and sustained HT were defined by normality or elevation of all 3 BPs, respectively. Average FU was 16 years.29)
BP = blood pressure; CV = cardiovascular; FU = follow-up; HT = hypertensives; NT = normotensives; WCH = white coat hypertension.
The PAMELA is a population study in which BP was measured in office, over day and night, and by subjects at home. This allowed us to investigate for the first time the relative risk in 2 WCH subgroups, that is, those in whom both out-of-office BP values were normal and those in whom one was found to be normal but the other was elevated. In this further analysis mortality was assessed over a 16-year follow-up (i.e., the longest follow-up available in longitudinal WCH studies).29) In a noticeable number of subjects normal 24-hour systolic BP or diastolic BP values were accompanied by a home systolic BP or diastolic BP elevation and vice versa. This allowed to split the WCH subjects into those in whom both 24-hour and home BP were normal (true WCH, 41.9%) and those in whom out-of-office BP was normal whereas the other was elevated (partial WCH, 58.1%). In the whole WCH group, the risk of dying showed remained almost twice (CV mortality) and 50% (all-cause mortality) greater than that of normotensive subjects when data were adjusted for major confounders. Notably, the most important and entirely new finding of the study, however, was that the incidence and risk of CV and all-cause mortality were not significantly different from those of normotensive subjects if both ambulatory and home BP values were normal. In contrast, in subjects in whom normality of one out-of-office BP was accompanied by elevation of the other, the incidence of fatal events was significantly increased, with a fully adjusted risk of CV and all-cause mortality that was, respectively 3-fold and 60% greater than that of normotensive individuals. This means that information on both out-of-office BP values is clinically relevant and that a diagnostic approach based on 3 rather than 2 different BPs may represent a valuable procedure to be implemented for refining CV risk evaluation.
In a subsequent analysis of the PAMELA database we have investigated another possibility to distinguish, within the WCH category, individuals at different CV risk, that is, whether CV risk differs between those in whom WCH is or not persistent at subsequent versus initial office BP measurements.30) Data analysis was restricted to untreated WCH hypertensives (versus untreated normotensive controls) to avoid the confounding effect of BP-lowering drugs. Compared with the normotensive group, the long-term risk of CV and all-cause death was not significantly different in unstable (not persistent) WCH, whereas in stable (persistent) WCH the risk was increased also when data were adjusted for baseline confounders, including ambulatory BP.
It worth of comment that earlier investigations on the prognostic significance of WCH has produced inconsistent results (i.e., evidence for an independent association with an increased CV risk as well as no difference from the risk entailed by the normotensive status) and similar divergent findings have been provided by some meta-analyses published in the last decade. In a pooled population of 7,961 initially untreated subjects from 8 studies, Pierdomenico et al.31) found that the incidence of CV events was not different in WCH compared to true normotensive subjects. The prognostic significance of WCH in 1,593 elderly with isolated systolic hypertension, free of CV disease at baseline and stratified according to the presence or absence of antihypertensive treatment was assessed by the investigators of the International Database on Ambulatory Blood Pressure Monitoring in Relation to Cardiovascular Outcomes (IDACO) study.32) During a median follow-up of 10.6 years, untreated subjects with WCH and true normotensives had a similar incidence of non-fatal and fatal CV events (HR, 1.17; 95% confidence interval [CI], 0.87–1.57; p=0.30). On the contrary, the results of 3 updated publications were in line with those generated by the PAMELA study. The International Database of HOme blood pressure in relation to Cardiovascular Outcomes (IDHOCO), a prospective registry totaling 6,458 participants from 5 different populations, followed for 8.3 years, documented that CV risk was significantly higher in WCH compared to normotensive subjects (adjusted HR, 1.42; 95% CI, 1.06–1.91; p=0.02).33)
Based on 14 studies for a total of 29,100 participants (13,538 normotensive, 4,806 WCH and 10,756 sustained hypertensive subjects), the results of the meta-analysis by Briasoulis et al.34) showed that in WCH, the risk of outcomes is substantially less than in both in and out-of-office (‘sustained’) hypertension. The authors further reported that in WCH individuals, 1) the incidence of overall CV events was 6.0% compared with the 4.0% seen in normotensive patients, with a 73% increase in risk (p<0.001), 2) the incidence of fatal CV events was 4.0 and 1.2% in the 2 groups, respectively, with an even greater CV risk increase (+179%).
Finally, data from the largest study published so far (a registry-based, multicenter, national cohort including 63,910 adults recruited from 2004 through 2014 in Spain) demonstrated that 24-hour systolic pressure was more strongly associated with CV and all-cause mortality than office systolic BP.35) As for WCH, this BP phenotype was more strongly associated with all-cause mortality than normotension. Results for CV mortality were similar to those for all-cause mortality. Overall, increasing evidence clearly supports the conclusion that in WCH the cumulative outcomes lay in an intermediate position between normotension and sustained hypertension.
THERAPEUTIC PERSPECTIVES
The WCH represents the only clinical condition in which the prognostic significance of office BP is completely ignored in terms of therapeutic decisions. This is because there are no prospective randomized clinical trials that have documented favorable effects of antihypertensive therapy on CV outcomes in individuals with WCH. Indeed, available information is limited on whether and to what extent WCH is affected by antihypertensive treatment.
To date, information is mainly based on few single small studies and post-hoc analyses of large clinical trials.36)37)38)39) The SYSTolic Hypertension in Europe (SYSTEUR) trial, which demonstrated that anti-hypertensive treatment reduces ambulatory BP and CV morbidity and mortality less in WCH than in sustained hypertensive individuals.38) In the hypertensive patients of the European Lacidipine Study on Atherosclerosis (ELSA), office and ambulatory BP were measured before treatment and at 6-month (office BP) or 12-month (ABPM) intervals during the 4-year administration of calcium channel blocker–based or β-blocker-based treatment.39) The 2 groups were pooled and data were analyzed separately in patients with sustained hypertension or WCH. In WCH antihypertensive therapy reduced office BP to a degree that was quantitatively similar to, or only slightly less pronounced than, that observed in sustained hypertensive patients, whereas it did not have any consistent lowering effect on 24-hours, day-time and night-time BP, at variance with the clear-cut persistent reduction seen in the sustained hypertensive group. This implies that in WCH, antihypertensive treatment should not be expected to have a significant lowering effect on ambulatory BP, even when office BP undergoes a concomitant marked and persistent reduction.
A further problematic point relies to the fact that the various hypertension guidelines have issued distinctly different recommendations. In the guidelines of the European Society of Hypertension and the European Society of Cardiology (ESH/ESC) this condition has been regarded as worthy of close follow-up, repeated medical examinations, and perhaps treatment.1) Indeed these guidelines offer precise practical indications to guide therapeutic making decisions can be summarized as follows. First, in subjects with WCH concomitant dysmetabolic risk factors and some asymptomatic organ damage (i.e., LVH), the presence of which raises CV risk, drug treatment may be considered in addition to appropriate lifestyle changes. Second, both lifestyle changes and drug treatment may be considered also when normal ambulatory BP values are accompanied by abnormal home BP values (or vice versa) because this condition is also characterized by increased CV risk.29) Third, in the absence of additional CV risk factors, intervention may be limited to lifestyle changes only, but this approach should be accompanied by a close follow-up of the patients (including periodical out-of-office BP monitoring) because, in WCH subjects, out-of-office BP is often higher than in truly normotensive subjects. Finally, an important element supporting the decision on pharmacological treatment in high-risk WCH individuals is related to the fact because of its high prevalence WCH was presumably well represented in antihypertensive drug trials that have established clinic BP reduction as the guidance for treatment.
On the contrary, in the guidelines issued by the British National Institute of Clinical Excellence (NICE), WCH has been equaled to normotension, with no need of medical visits, ad hoc examinations, and treatment in the subsequent 5 years.40) Although epidemiological and pathophysiological evidence accumulated over the last 7 years supports the adverse nature of WCH, 2 important hypertension guidelines published in the 2017 seem surprisingly to share all or part of NICE's recommendations. In fact, the Hypertension Canada's 2017 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults state “If the out-of-office BP average is not elevated, WCH should be diagnosed and pharmacologic treatment should not be instituted (grade C)”, without additional comments.41)
The new 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guidelines for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults5) underline that many, but not all, studies have identified a minimal increase in risk of CV events or all-cause mortality in subjects who have WCH. This has resulted in a recommendation by some expert panels to search for WCH with ABPM (or home BP monitoring) to avoid initiating BP lowering medications in such individuals. Once WCH is identified (day-time or home BP monitoring <130/80 mmHg) these guidelines simply recommend: 1) lifestyle modification, 2) annual ABPM or home BP monitoring to detect progression to sustained hypertension. The position of the Canadian and USA guidelines seems not to take into account the fact that the subjects with WCH present considerable differences in terms of total CV risk resulting from the presence of one or more metabolic risk factors, target organ damage, previous CV disease, obesity and age. In these guidelines the normality of the out-of-office BP values is the only criterion that allows to exclude the need for any pharmacological treatment.
In order to avoid underestimating the adverse nature of WCH and neglecting the clinical management of these patients, physicians should take these considerations into account. Because CV risk can markedly differ between WCH individuals a comprehensive assessment of CV risk factors should be performed in order to identify the fraction with a risk above average in whom a closer follow-up may be required. Similarly, the search for organ damage in these patients can be extremely useful for identifying those at high risk where drug treatment is indicated. In addition to assessing traditional risk factors and organ damage, a further stratification of the risk connected to the WCH can be obtained by performing more than one office visit and collecting both ambulatory and home BP values because CV risk has been found to be greater if the elevation of office BP is confirmed at a second set of measurements and only one of the 2 out-of-office BPs is normal.42)
CONCLUSIONS
WCH, is common and recent data show that it is by no means clinically innocent because of its frequent association with metabolic abnormalities, subclinical organ damage, and a risk of CV events that, although less than in sustained hypertensives, is higher than that of truly normotensive individuals. At present, the identification of the fraction of high-risk WCH subjects seems to be a key step in the selection of appropriate therapeutic strategies including antihypertensive therapy. However, in order to optimize the clinical management of the WCH prospective trials capable of providing scientifically founded data on the therapeutic decision to take in WCH are needed.
 XML Download
XML Download