

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Left ventricular ejection fraction (LVEF) is a widely used parameter for the assessment of left ventricular (LV) systolic function, and reduced LVEF is associated with various cardiac diseases.1) It has a clinical significance as a predictor for higher incidence of acute ischemic stroke (AIS) and mortality in patients with congestive heart failure (CHF) and coronary heart disease (CHD).2)3) Reduced LVEF irrespective of overt CHF increased the risk of AIS in the general population.4) However, the effect of reduced LVEF on overall outcomes after AIS is a debated issue.
A previous study reported that reduced LVEF was associated with the early and long-term poor functional outcome and mortality in AIS.5)6) LVEF was an independent predictor of 5-year mortality in young adult patients with first-ever AIS.7) In contrast, in the absence of atrial fibrillation (AF), reduced LVEF itself was not related to higher mortality rate at long-term follow-up in AIS.8) These inconsistent results of the previous studies could be attributed to the presence of concomitant cardiac diseases and different assessments of mortality and functional disability.
AF and CHD are major two cardiac diseases which lead recurrent cardiovascular events and mortality after AIS.9) The aim of this study is to identify whether reduced LVEF per se, in the absence of AF or CHD, is related to the long-term functional and cardiovascular events in AIS.
METHODS
Patients and case ascertainment
We screened the 2,289 patients with AIS (within 7 days from the onset) or transient ischemic attack (TIA) who were prospectively registered in Soonchunhyang University Hospital from January 2008 to July 2016. The patients with AF (n=484), CHD (n=128) and cardiomyopathy (n=15) were excluded. CHD was defined as any history of myocardial infarction (MI), coronary stenting or ischemic change of cardiac muscle detected by transthoracic echocardiography (TTE) at admission. Cardiomyopathies were diagnosed in the absence of abnormal loading conditions or CHD to cause systolic impairment by the cardiologist.10) The followings were also excluded: stroke of other determined etiologies including arterial dissection, Moyamoya disease, cerebral venous thrombosis and vasculitis (n=74); patients without magnetic resonance angiography or computed tomography angiography (n=52); patients without TTE (n=71). Finally, a total of 1,465 patients with AIS (n=1,342; 91.6%) or TIA (n=123; 8.4%) participated in the analysis. This study was approved by the local Institutional Review Board (No. 2017-01-032) before the study initiation, and all of the subjects agreed on the consent form for the poststroke outcome catchment.
Variables and other risk factors
Data were systematically collected including demographic data, medical history, vascular risk factors, laboratory findings and poststroke outcomes in a web-based registry.11) Hypertension was defined as current use of any antihypertensive medication or a systolic blood pressure of at least 140 mm Hg and/or a diastolic blood pressure of at least 90 mm Hg on the seventh day after stroke onset. Diabetes mellitus was defined as current medication of oral hypoglycemic agents or fasting serum glucose ≥126 mg/dL or HbA1c ≥6.5%. Sampling of serum lipid profiles was conducted on the day after the admission with the patients fasting overnight. Presence of smoking habit meant current smoker or former smoker who had quit within 6 months before the stroke onset. Stroke severity was assessed by National Institutes of Health Stroke Scale (NIHSS) by a neurologist. The uses of antithrombotics, antihypertensives, and statins were counted when information of ≥80% adherence to prescribed drug was collected by patients or caregivers during the follow up period. The 24-channel elecrocardiography (ECG) and Holter monitoring were performed in all patients with AIS, and additionally frequent ECG and Holter monitoring were repeated during hospitalization when a cardioembolic stroke is highly suspicious by neuroimaging.
Echocardiographic data
Among the patients without AF or CHD, transthoracic echocardiography was conducted in 95.4% which was relatively higher than that of whole registered patients within 7 days after the stroke onset.12) The Philips iE33 (Philips Medical Systems, Bothell, WA, USA) with 5-MHz transduce was used for M-mode and Doppler by 3 cardiologists (Hyon MS, Park BW, and Lee MH) who were blind to the information of this study. With the subjects on the left lateral decubitus position, M-mode based parasternal long-axis left atrial diameter and LV posterior wall thickness were obtained. LVEF was measured by Simpson biplane method. If technically unavailable, Teichholz method or visual estimation was used. Doppler mitral valve inflow was obtained by pulsed wave from the apical window, with a 1- to 3-mm sample volume placed between the tips of the mitral leaflets during diastole. Mitral peak E velocity was measured from the transmitral flow tracing. Early diastolic mitral peak E′ velocity was estimated by tissue Doppler imaging measurements at the mitral annulus. The ratio of transmitral early LV filling velocity to early diastolic tissue Doppler imaging velocity of the mitral annulus (E/E′) was calculated.
Outcome catchments
Modified Rankin Scale (mRS) was used to estimate the functional disability.13) We defined the poor functional status as mRS ≥3 (moderate disability; requires some help, but able to walk without assistance). Major adverse cardiovascular events (MACE) included an occurrence of nonfatal stroke, nonfatal MI or cardiovascular death. Cardiovascular death was defined as a death resulting from MI, CHF, stroke, cardiovascular procedures, cardiovascular hemorrhage, and other cardiovascular causes. When death is clearly due to a noncardiovascular cause, a cardiovascular cause of death was excluded.14) The physician or clinical researcher rated mRS, and identified cardiovascular outcomes of the subjects at every visit of outpatient clinic and by telephone interview at 3 months and 1 year. In case of missing data, we investigated the data from National Health Insurance Service to check whether a subject had expired or not. The cause of death was identified by the medical record or telephone interview with the caregivers.
Statistical analysis
Statistical analysis was performed with IBM SPSS Statistics 18.0 (SPSS Inc., Chicago, IL, USA). Sample size was calculated according to the 1-year all-cause mortality rate of about 23% in AIS.15) We estimated that the enrollment of 1,434 cases would provide statistical power of 80% to detect a relative increase of 20% in the fraction of cardiovascular mortality in the patients with reduced LVEF. We used paired t-test for the continuous variables and χ2 test for the categorical variables to examine the differences of each variable. The LVEF were divided by 10% interval from 55% (the lowest cutoff value of normal range). Mean survival times of each subgroup were presented with 95% confidence interval (CI) based on the Kaplan-Meier estimates. Survival curve was plotted for each subgroup, and p value was calculated by log-rank test between LVEF <55% compared with the remainder. Cox proportion hazards regression analyses were conducted to evaluate the predictors for MACE and all-cause mortality. We assessed the incremental value from LVEF by increase of area under curve (AUC) and net reclassification improvement (NRI) in survival analysis to evaluate a new risk model for predicting MACE and all-cause mortality.
RESULTS
A number of 1,465 patients were followed up for functional disability and cardiovascular outcomes. The mean follow-up time was 259.9±148.8 days. During follow-up period, a total of 29 non-fatal strokes, 3 MIs and 33 cardiovascular deaths occurred. There were 60 MACE and 53 all-cause mortalities. The mean LVEF was 66.3±7.1 (range, 29–84) for study subjects (Figure 1). The proportion of poor mRS and the incidence of MACE are shown among LVEF groups divided by 10% interval (Table 1). The functional disability were not different among 4 LVEF subgroups (p=0.553). The crude incidence of MACE and all-cause mortality within 1 year of the index stroke was higher in the lowest LVEF group. The cumulative incidence of MACE and all-cause mortality were significantly higher in the group of LVEF <55 compared with the remainder (p=0.022 and 0.009 in log-rank test; Figure 2).
Figure 1
The distribution of LVEF in the subjects of this study.
LVEF = left ventricular ejection fraction.
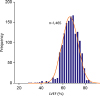
Table 1
Poststroke outcomes in LVEF subgroups

Figure 2
Cumulative incidence of MACE (A) and all-cause mortality (B) in LVEF subgroups.
LVEF = left ventricular ejection fraction; MACE = major adverse cardiovascular events.

Baseline characteristics with echocardiographic parameters are given by the occurrence of MACE and all-cause mortality (Table 2). The mean intervals from stroke onset to timing of echocardiographic measurement were not different between without and with all-cause mortality (1.3±0.7 vs. 1.5±0.8 days, p=0.095). The means of LVEF was lower in event groups (p=0.003 and 0.007), but the other echocardiographic parameters were not different between the two groups. The mean left atrial diameter (LAD) was rather smaller in the survivors.
Table 2
Baseline characteristics according to the presence of MACE and all-cause mortality
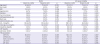
BMI = body mass index; CRP = C-reactive protein; LAD = left atrial diameter; LDL-C = low-density lipoprotein cholesterol; LVEF = left ventricular ejection fraction; LVPWd = left ventricular posterior wall dimension; MACE = major adverse cardiovascular events; NIHSS = National Institutes of Health Stroke Scale; TTE = transthoracic echocardiography.
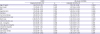
Regarding the prediction of MACE and all-cause mortality, older age (per 10 years) was associated with an increased rate of MACE (hazard ratio [HR], 1.64; 95% CI, 1.23–2.20) and all-cause mortality (HR, 1.72; 95% CI, 1.19–2.48). NIHSS (HR, 1.14; 95% CI, 1.08–1.20) and C-reactive protein (HR, 1.08; 95% CI, 1.02–1.15) significantly increased hazards for all-cause mortality, but body mass index (HR, 0.83; 95% CI, 0.73–0.94) decreased the hazards. In terms of LVEF (per 10%), HRs were 0.54 (95% CI, 0.36–0.80) for MACE and 0.61 (95% CI, 0.39–0.97) for all-cause mortality after adjusting traditional risk factors and potential determinants (Table 3). LAD (HR, 0.95; 95% CI, 0.90–1.00; p=0.055) and E/e (HR, 1.01; 95% CI, 0.94–1.09; p=0.692) were not significant when they participated in the same Cox hazard regression models instead of LVEF. AUC was improved from 0.697 to 0.718 for MACE (p=0.149) and from 0.909 to 0.910 (p=0.842) for all-cause mortality in the new model. An estimated overall NRI was 0.009 (95% CI, −0.108, 0.127) for MACE and 0.036 (95% CI, −0.245, 0.319) for all-cause mortality.
Table 3
Adjusted HRs for the presence of MACE and all-cause mortality during 1 year
DISCUSSION
A few studies had been conducted to evaluate the relationship between reduced LVEF and outcomes in AIS. Reduced LVEF was found to be related to the poor functional outcome (mRS ≥3) and mortality within 3 months after AIS in patients with preexisting CHF.6) But, this study had small cases of 503, and did not investigate long-term outcomes. Moreover, echocardiography was examined only in patients diagnosed with CHF based on clinical criteria.6) Milionis et al.5) proposed that low LVEF could identify a subset of AIS patients at high risk of early and long-term stroke-related disability and mortality. In this study, however, the patients with AF or CHD which can heavily influence on cardiovascular events and mortality after AIS16) were not excluded. Therefore, it was still unclear whether LV systolic dysfunction itself, in the absence of cardiac disease, is associated with poststroke outcomes.
AF is not only a cause but a consequence of reduced LVEF.17) Patients with CHD are at high risk for reduced LVEF and the mortality rate correlates highly with the degree of LV dysfunction.1)18) Because AF and CHD is closely related with mortality, stroke risk and quality of life in patients with CHF,9) the independent impact of LVEF on outcomes in AIS should be assessed by excluding the interaction between the cardiac diseases and LVEF. Holmström et al.8) revealed that reduced LVEF in the absence of AF was not associated with long-term all-cause mortality in AIS. However, relatively small sample size of 132 cases were analyzed, and outcome measurement contained only long-term all-cause mortality without measurement of functional disability and causes of death.
Several hypotheses could be proposed for the relationship between LV systolic dysfunction and poststroke mortality. Reduced LV function is a risk factor for the higher rate of recurrent stroke and MI.2) The higher prevalence of underlying risk factors in patients with reduced LVEF might contribute to the increased cardiovascular mortality.19) Although we excluded the patients with CHD by clinical history and echocardiography, the presence of asymptomatic CHD which is very prevalent in AIS20) might have influence on the cardiovascular events. Furthermore, even in normal range of LV function, reduced LVEF had an independent association with poststroke cardiovascular events in our study. This may suggest a possibility that subclinical LV dysfunction may exist in patients with AIS. Increased incidence of thromboembolic events in patients with reduced LVEF could affect the cardiovascular outcome.21) Cognitive impairment is more common in patients with reduced LV function,22) which could have some impact on higher mortality rate.23)
The negative effect of CHF on functional outcome in AIS has been considerably investigated.6)19) Decreased exercise capacity in patients with CHF could be an obstacle to the rehabilitation and finally induce poor functional outcome.6) In our study, however, reduced LVEF was not an independent predictor for poor functional outcome. This might be because reduced LVEF, as long as it does not cause symptoms of CHF, could not lead to the poor functional disability. The absence of clinical symptoms of CHF in patients with reduced LVEF is common and considered as a precursor to overt CHF.24) Exclusion of patients with AF and CHD which are related to the severe functional deficits in AIS could also have affected the results.25)
There are some advantages in our study. First, though there is insufficient consensus of performing echocardiography in all of the patients with AIS,26) the performance rate of echocardiography in our study is much higher than other centers.27) Second, most previous reports had categorized LVEF into inconsistently dichotomized two (preserved and reduced) groups,2)4)5)6)7)8) and led to very small number of the patients with low LVEF. Regression analysis of interesting factor as continuous variable like our study can reflect statistically more accurate results.28)
It is also noteworthy to address the limitations in this study. First, the study was retrospectively designed in a single center although all of the data including LVEF was collected prospectively. Biases of selection, misclassification or information are possible. Second, although we excluded the patients with AF by frequent ECG and Holter monitoring, implantation of loop recorder was not applied in this study population. The existence of undetected paroxysmal AF could have affected the cardiovascular outcomes. Third, LVEF could be reduced transiently by the cerebral infarct itself or severity of symptoms.29) Our study did not include the information of the location of cerebral infarct which could cause cardiac autonomic derangement. Fourth, various echocardiographic parameters for LV dysfunction, especially LV global longitudinal strain and LV geometric pattern, were not assessed. And, data measured by Teichholz formula or visual estimation in some patients could contain inaccurate values of LVEF. Finally, given that a slight improvement of AUC and NRI was not statistically significant, the additional prognostic value of LVEF would be limited in predicting poststroke cardiovascular outcomes.
In conclusion, reduced LVEF could be an independent predictor of cardiovascular events and mortality after AIS even without AF or CHD. Routine echocardiography in patients with AIS may provide a prediction of poststroke cardiovascular outcome as well as additional information about the strategies for secondary prevention. A larger prospective study is warranted for the clinical implication of echocardiographic parameters for the prognosis of the patients with AIS.
 XML Download
XML Download