

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Oxidative stress (OS) and inflammation might play important roles in the pathogenesis and perpetuation of atrial fibrillation (AF).1)2) Previous research has indicated that there is some synergism between OS and a systemic inflammatory response; oxidative metabolites such as hydrogen peroxide can promote synthesis of proinflammatory cytokines, resulting in amplification of the inflammatory cascade. Conversely, the acute-phase reactant C-reactive protein (CRP) has been shown to enhance intracellular generation of reactive oxygen species (ROS).3)
The role of inflammation in the development of AF is well demonstrated, and the relationships between various inflammatory biomarkers and AF have been established in the past few years.4) High-sensitivity CRP (hsCRP) was most frequently measured as one of these biomarkers. Elevation in hsCRP level has been associated with an increased risk of AF recurrence following a successful electrical cardioversion5) and catheter ablation.6)
A few studies have recently reported the relationship between the neutrophil to lymphocyte ratio (NLR) and AF.7)8)9)10)11)12) The NLR has emerged as a novel systemic inflammatory marker and a prognostic indicator of cardiovascular disease.7)8) The potential association between the NLR and development of AF has also been reported.9)10)11)12)
Recently, several studies have shown the potential association between increased red cell distribution width (RDW) and adverse cardiovascular events, and elevated RDW might also be correlated with nonvalvular AF.13)14) A high RDW level might reflect an activated inflammatory state, and the RDW is also an independent predictor of a high CHA2DS2-VASc score in AF patients;15) however, the potential mechanisms between elevated RDW and development of AF are unclear.
The 8-iso-prostaglandin F2α (8-iso-PGF2α) has been suggested as a new indicator of OS, and it is currently the most accurate and reliable method for quantifying OS in humans.16)17) Currently, there is a lack of easily determinable bedside markers for OS; therefore, identifying whether any of these readily available systemic inflammatory markers are correlated with OS will be valuable for clinical diagnostics. However, there are only a limited number of studies about the possible links between systemic inflammatory markers and OS burden in an AF population. In this study, we aimed to assess whether these systemic inflammatory markers were associated with 8-iso-PGF2α as an index of OS in AF.
SUBJECTS AND METHODS
Study population and grouping
This cross-sectional study recruited 220 consecutive patients who visited the clinic for medical check-ups or were diagnosed with AF and were admitted for an evaluation or radiofrequency catheter ablation from June 2011 through July 2012. All tests including blood sampling for chemistry tests, transthoracic echocardiography, 24-hour ambulatory electrocardiogram (ECG) recordings, and treadmill exercise tests were performed at the time of admission. Based on the past medical history and test results, patients were categorized into the ‘No AF group’ (103 patients) or ‘AF group’ (117 patients). The patients that were included in the No AF group had no known inflammatory disease, significant conduction disturbance, any atrial or ventricular tachyarrhythmia, and heart failure. The AF group was subcategorized into a paroxysmal AF group (PaAF, 65 patients) or persistent AF group (PeAF, 52 patients) based on the definition from the 2012 focused update of the European Society of Cardiology guidelines.18) The protocol for this study was approved by the Institutional Review Board of Yeungnam University Hospital (YUMC 2016-12-017), and informed consent was obtained from all study participants.
Systemic markers of OS and inflammation
The 8-iso-PGF2α is an isoprostane that is useful for assessing OS in vivo. We quantified the 8-iso-PGF2α level in blood to estimate the OS burden. Patients were instructed to, if possible, discontinue medications such as statins, angiotensin-converting enzyme inhibitors (ACEIs), or angiotensin II receptor blockers for 1–5 days, depending on the 5 half-lives of the drug, before blood sampling. After an overnight fasting period, blood samples were collected in sterile vacuum tubes in the morning and immediately centrifuged at 15,000 g for 15 minutes; plasma samples were frozen at 80°C until the time of the assay at the conclusion of the study. We used 1 part 10N NaOH for every 4 parts plasma sample. After incubation at 45°C for 2 hours, 100 μL of concentrated (10N) HCl per 500 μL of hydrolyzed sample were added, and the samples were centrifuged for 5 minutes at 12,000 rpm in a microcentrifuge. The 8-iso-PGF2α level was evaluated using a commercial enzyme-linked immunosorbent assay kit (OxiSelect™ 8-iso-Prostaglandin F2α ELISA kit; Cell Biolabs Inc., San Diego, CA, USA). A total of 3 repeated results were obtained, and the mean value was reported.
The hsCRP, NLR, and RDW levels were measured to assess the burden of inflammation. The hsCRP was assayed by a highly sensitive near infrared particle immunoassay rate methodology (SYNCHRON High Sensitivity Cardiac C-Reactive Protein reagent; Beckman Coulter Inc., Brea, CA, USA) on a UniCelDxC 880i (Beckman Coulter Inc.). The differential white blood cell count, including the neutrophil, lymphocyte, and RDW levels, was measured using the automated ADVIA 2120i system (Siemens, Erlangen, Germany).
Statistical analysis
Numerical variables are expressed as the mean±standard deviation (SD). Frequencies and percentages are used to report categorical variables. The skewed variables, such as hsCRP, were logarithmically transformed to improve the normality prior to the analysis. We used a t-test for continuous variables and χ2 test for categorical variables to compare the No AF and the AF groups. We used an one-way analysis of variance (followed by a Tukey HSD or Dunnett T3 test for multiple comparisons among groups) and χ2 test (linear by linear association) to test the differences in the study variables among the No AF, PaAF, and PeAF groups. We used the Pearson correlation to assess the relationships between systemic markers of inflammation and OS. We compared the 8-iso-PGF2α based on the AF duration or CHA2DS2-VASc score using a Jonckheere-Terpstra test. A Pearson correlation and linear regression analysis were used to evaluate the clinical factors associated with the burden of inflammation and OS. All analyses were performed using IBM SPSS version 20.0 (IBM Co., Armonk, NY, USA), and the level of statistical significance was set at a p<0.05.
RESULTS
Baseline characteristics
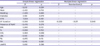
The clinical characteristics, systemic inflammatory markers, and 8-iso-PGF2α levels of the study subjects are shown in Table 1. There were no significant differences in age or incidence of diabetes mellitus (DM) or hypertension (HTN) between the groups. There was a graded increase in the left atrial antero-posterior (LAAP) diameter depending on the duration and type of AF (42.8±5.5 mm for PeAF group, 38.4±6.2 mm for PaAF group, and 35.1±4.3 mm for No AF group, p<0.001). As expected, the AF duration was longer in the PeAF group than in the PaAF group (40±40 months vs. 22±33 months, p=0.01). The mean CHA2DS2-VASc score did not differ between the PaAF and PeAF groups (1.1±1.3 vs. 1.2±1.2, p=0.68). The 8-iso-PGF2α level and NLR were higher in the AF group than in the No AF group (p<0.001 for 8-iso-PGF2α, p=0.048 for NLR). The 8-iso-PGF2α concentrations of both the PaAF and PeAF groups were higher compared to those of the No AF group (p<0.001 and p=0.024, respectively). The NLR and RDW in the PeAF group were higher than those in both the No AF group and PaAF group (p=0.041 and p=0.031 for NLR, p=0.057 and p=0.031 for RDW, respectively).
Table 1
Clinical characteristics, systemic inflammatory markers, and 8-iso-PGF2α levels of study subjects

Data are presented as mean±SD or number (%).
8-iso-PGF2α = 8-iso-prostaglandin F2α; ACEI = angiotensin-converting enzyme inhibitor; AF = atrial fibrillation; ARB = angiotensin II receptor blocker; BMI = body mass index; Ca blocker = calcium channel blocker; fT4 = free thyroxine; Hb = hemoglobin; HDL = high-density lipoprotein; hsCRP = high-sensitivity C-reactive protein; HTN = hypertension; LAAPd = left atrial antero-posterior diameter; LDL = low-density lipoprotein; lnhsCRP = natural log-transformed high-sensitivity C-reactive protein; LVEF = left ventricular ejection fraction; NLR = neutrophil to lymphocyte ratio; PaAF = paroxysmal atrial fibrillation; PeAF = persistent atrial fibrillation; RDW = red cell distribution width; SD = standard deviation; Tc = total cholesterol; TG = triglyceride.
*No AF vs. AF, overall, †PaAF vs. PeAF.
Markers of OS and systemic inflammation in AF
The differences in 8-iso-PGF2α level and systemic inflammatory markers between the No AF and AF subgroups are shown in Figure 1. As mentioned in Table 1, the 8-iso-PGF2α levels were higher in both the PaAF and PeAF subgroups than in the No AF group and tended to be higher in the PaAF group compared to the PeAF group. Interestingly, there was a graded decrease in the 8-iso-PGF2α level along with an increase in the AF duration (Quartile 1, 86.91±55.67 pg/mL vs. Quartile 2, 73.53±42.90 pg/mL vs. Quartile 3, 70.32±38.20 pg/mL vs. Quartile 4, 57.68±42.29 pg/mL, p=0.008) in the AF group (Figure 2A). In contrast, the lnhsCRP increased gradually depending on the AF duration (Q1, −2.43±0.93 vs. Q2, −2.23±0.74 vs. Q3, −2.15±0.87 vs. Q4, −1.96±1.04, p=0.087) (Figure 2B). No difference in the 8-iso-PGF2α level according to the CHA2DS2-VASc score was found (Supplementary Figure 1).
Figure 1
Box plots depicting the differences in 8-iso-PGF2α level and systemic inflammatory markers between the No AF and AF subgroups.
8-iso-PGF2α = 8-iso-prostaglandin F2α; AF = atrial fibrillation; lnhsCRP = natural log-transformed high-sensitivity C-reactive protein; NLR = neutrophil to lymphocyte ratio; PaAF = paroxysmal atrial fibrillation; PeAF = persistent atrial fibrillation; RDW = red cell distribution width.
*p<0.05.

Figure 2
The changes in 8-iso-PGF2α and lnhsCRP levels according to quartile of AF duration. The graph is expressed as the mean±SD. AF duration was graded as 1st quartile (≤3 months), 2nd quartile (3–12 months), 3rd quartile (12–39 months), and 4th quartile (>39 months) in the AF group.
8-iso-PGF2α = 8-iso-prostaglandin F2α; AF = atrial fibrillation; lnhsCRP = natural log-transformed high-sensitivity C-reactive protein; SD = standard deviation.

Correlations between OS markers and inflammation in AF
The relationships between OS markers and inflammation were analyzed in the AF group (Figure 3). Neither hsCRP nor NLR was correlated with the 8-iso-PGF2α level in the AF group. The RDW was not correlated with the level of 8-iso-PGF2α in the AF group.
Figure 3
Scatterplots depicting the relationship between the 8-iso-PGF2α and systemic inflammatory markers in AF; (A) 8-iso-PGF2α vs. hsCRP, (B) 8-iso-PGF2α vs. NLR, and (C) 8-iso-PGF2α vs. RDW.
8-iso-PGF2α = 8-iso-prostaglandin F2α; AF = atrial fibrillation; hsCRP = high-sensitivity C-reactive protein; lnhsCRP = natural log-transformed high-sensitivity C-reactive protein; NLR = neutrophil to lymphocyte ratio; RDW = red cell distribution width.

Factors associated with OS markers and inflammation in the AF group
A multiple linear regression analysis was performed to evaluate factors that determined the burden of OS and systemic inflammation in the AF group. The 8-iso-PGF2α level was negatively correlated with the AF duration (β=−0.259, p=0.049) (Table 2). On the other hand, the markers of inflammation were positively correlated with the LAAP diameter (β=0.055, p<0.001 for the lnhsCRP) and the presence of PeAF (β=1.225, p=0.002 for NLR; β=0.509, p=0.002 for RDW) (Supplementary Tables 1, 2, 3).
Table 2
Factors associated with 8-iso-PGF2α level in AF
8-iso-PGF2α = 8-iso-prostaglandin F2α; AF = atrial fibrillation; BMI = body mass index; fT4 = free thyroxine; HDL = high-density lipoprotein; HTN = hypertension; LAAPd = left atrial antero-posterior diameter; LDL = low-density lipoprotein; PeAF = persistent atrial fibrillation; Tc = total cholesterol; TG = triglyceride.
DISCUSSION
The main findings of this study were: 1) there was no direct correlation between the OS marker 8-iso-PGF2α and the systemic inflammatory marker hsCRP in AF. Neither the NLR nor RDW was correlated with serum 8-iso-PGF2α level, as was the case with the hsCRP, and 2) the 8-iso-PGF2α concentration was higher in the AF group than in the No AF group. In addition, the 8-iso-PGF2α level decreased gradually with an increase in AF duration or persistence, contrary to the change in the inflammatory marker.
Previous studies showed that OS and inflammation were mutually interactive in the pathogenesis of AF.19)20)21)22)23) Therefore, it will be important to determine if a direct correlation between OS burden and the inflammatory markers is present in AF. However, there are not currently any studies that have explored the interconnection between inflammation and OS in the context of AF. Therefore, based on the findings of our study, no readily available inflammatory marker, including hsCRP, can be used as a surrogate marker of OS in AF.
In the analysis, we found that AF duration was the only factor that was negatively correlated with OS. In contrast, the inflammatory markers were positively correlated with left atrial diameter and presence of PeAF. Therefore, inflammation might represent a pathogenic role in the maintenance of AF, and OS might play a role in the initiation of AF.
The change in the major source of OS in the natural history of AF could be caused by a decreased OS burden with persistence of AF.24)25) Direct myocardial generation of ROS in the atrium has appeared to play a role in initiating and sustaining AF in animal models and humans.26)27) Among the several potential sources of ROS present in the atrial myocardium, NOX2-containing NADPH oxidases are the main sources of ROS production in human atrial myocytes, and NOX-derived ROS production is increased in atrial samples from patients with (mostly paroxysmal) AF.28) Reilly et al.24) reported that OS assessed by NOX2 activity and urinary isoprostanes increased in patients with paroxysmal and recent AF. In keeping with these findings, uncoupled nitric oxide synthase (NOS) activity and mitochondrial oxidases become the most important sources of ROS in the setting of longstanding AF and atrial structural remodeling. A study by Cangemi et al.25) showed that patients with permanent AF had a weak increase in the serum levels of soluble NOX2-derived peptides and no difference in urinary isoprostanes compared with the controls. Findings of earlier studies reporting that a nitric oxide-redox imbalance in AF differs with the duration of AF support our results. Loss of atrial myocardium, which is an important source of ROS in AF, and progression to atrial fibrosis (structural remodeling) with perpetuation of AF can explain the decrease in OS burden in longstanding AF.
However, these results are not consistent with other previous studies, which have found appropriate biomarkers for examining the correlations between the different inflammatory markers and oxidative indices.29)30) Il'yasova et al.29) reported that the urinary level of 2,3-dinor-5,6-dihydro-15-F2t-isoprostane (F2-IsoP) positively correlated with the CRP level in 60 individuals at high risk for cardiovascular disease. Korantzopoulos et al.30) presented a few studies that investigated the possible link between CRP and OS, but those studies included subjects who had peripheral arterial disease, end-stage renal disease on dialysis, HTN, or diabetes; individuals with AF were not included in their studies. Thus, we can assume that the involvement of inflammation and oxidative damage in the pathogenesis of age-related chronic diseases differs from that of AF.
There were some limitations to this study. First, the baseline clinical characteristics that could affect OS, such as smoking habits, age, and gender, were not completely matched between the groups. However, no difference in 8-iso-PGF2α level between the patients with CHA2DS2-VASc scores of 0, 1, or ≥2 was found. This indicated that those comorbid conditions did not affect the oxidative status in this study. Second, although patients were educated to stop all medications with anti-inflammatory and anti-oxidative effects, such as statins or ACEIs, before sampling, some were allowed to continue due to ethical issues. This might have influenced our results. Finally, blood samples were not drawn during AF sustenance, especially in patients with PaAF. This might have biased the biomarker levels of inflammation and OS. Because both inflammation and OS involve complicated linking messengers and metabolites, it is difficult to draw a firm conclusion from this study, which examined a few biomarkers in a small number of patients. Based on our results, additional studies are needed to determine if there are direct correlations or interactions between inflammation markers and OS in AF.
In conclusion, the level of 8-iso-PGF2α, an OS marker, was not correlated with the conventional systemic inflammatory markers in AF. This discordant relationship suggests a different pathogenic role of OS and inflammation in atrial structural and electrical remodeling in AF. A larger prospective cohort study is needed to elucidate these relationships.
 XML Download
XML Download