

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Implantable cardioverter-defibrillators (ICDs) are one of the established therapies for preventing sudden cardiac death in patients who are considered to be at a high risk for ventricular tachycardia (VT) or ventricular fibrillation (VF), or for those who are resuscitated from sustained VT/VF.1)2) Patients with left ventricular (LV) dysfunction due to ischemic or non-ischemic causes are at a risk for life threatening ventricular tachyarrhythmias, and a properly delivered shock from an ICD can improve their survival.3)4)5)6)7)8)9)10)11)12) Current guidelines for the implantation of ICDs have been supported by sufficient evidence from clinical trials on their beneficial effects on survival.1) However, to date, there are few data in the Korean population, about the efficacy of ICD therapy for preventing sudden death from sustained VT/VF due to ischemic or non-ischemic cardiomyopathy (CMP). Mainly Caucasians from Western societies have been the subjects of most clinical trials to prove the efficacy of ICDs in the prevention of sudden cardiac death. Some limitations would exist in extrapolating that data to Korean patients in the context of a different ethnic group. An ICD registry in this community would be a valuable resource that could provide important insight into the clinical and procedural characteristics of patients receiving ICDs in Korea, and further contribute to refine cardiovascular outcomes.13)
This study was done to evaluate the efficacy of ICD therapy in the Korean population of the Yeongnam province, according to the indication (primary prevention vs. secondary prevention) and underlying etiologies (non-ischemic CMP vs. ischemic CMP).
Subjects and Methods
From November 1999 to September 2012, a total of 287 patients enrolled in the registry database of 9 centers in Yeongnam province (Andong Medical Group, Daegu Catholic University Medical Center, Daegu Fatima Hospital, Inje University Busan Paik Hospital, Keimyung University Dongsan Medical Center, Kosin University Gospel Hospital, Kyungpook National University Hospital, Pusan National University Yangsan Hospital, and Yeungnam University Medical Center, in alphabetical order) were analyzed in this retrospective study. Patients classified as having hypertrophic CMP, arrhythmogenic right ventricular dysplasia/cardiomyopathy, genetic arrhythmic disorders (Brugada syndrome and long QT syndrome), or idiopathic VF were excluded. The selected patients (n=146) were divided into two groups, according to the following two criteria: 1) etiology: ischemic CMP (n=73) vs. non-ischemic CMP (n=73), and 2) indication for the device implantation: primary prevention (n=36) vs. secondary prevention (n=110, Fig. 1).
Ischemic CMP was traditionally considered to be present in patients with heart failure who had either a myocardial infarction (MI), evidence of a viable hibernating myocardium, or severe coronary disease on angiography, which might be regarded as the determining cause. Conversely, non-ischemic CMP was defined as heart failure not due to coronary arterial disease. The ICD for primary prevention were implanted when the following reimbursement criteria of the Korean Health Insurance Review & Assessment Service was met: patients with an LV ejection fraction (EF) less than 30%, or 30-35% with the induction of sustained VT/VF in the electrophysiologic study. ICD implantations for secondary prevention were those in which the device was implanted because they had a decreased LV systolic function and documented VT, or were resuscitated from sudden cardiac arrest due to witnessed or unwitnessed VT/VF.
All devices were implanted in the right or left subpectoral region, under local anesthesia. The manufacturers of the generators were Medtronic (Minneapolis, MN, USA), Guidant Corp. (Indianapolis, IN, USA), and St. Jude Medical (St. Paul, MN, USA). Each center attempted to tailor the shock therapy based on electrophysiologic studies, and an arrhythmic history of the patients, without any prior standardization.
After the device implantation, all ICD/CRT-D (cardiac resynchronization therapy with defibrillator devices) were regularly evaluated, and the follow-up data, including the intracardiac electrograms, were reviewed by experienced electrophysiologists at each center. The overall clinical outcomes were determined by comprehensively reviewing the medical records during routine outpatient visits or by telephone interviews during the follow-up period. The endpoints of this study comprised of all-cause deaths and shock therapy, whether it was appropriate or not. All-cause death was defined as the sum of the cardiac and non-cardiac deaths (death that was not primarily due to cardiac causes); after reviewing the medical records, cardiac death was further subclassified as sudden or non-sudden death. Appropriate shocks were defined as those that terminated VT/VF that would not spontaneously terminate or could not be terminated by anti-tachycardia pacing (ATP). Inappropriate shocks included the traditionally classified shocks rendered in unnecessary situations: shocks delivered for supraventricular tachycardia (SVT) (such as atrial fibrillation [AF] with a rapid ventricular response, or oversensing), those delivered for ventricular tachyarrhythmias (monomorphic or polymorphic) that would otherwise have spontaneously terminated without delivery of any therapy, VTs that would terminate with ATP, or VT that was too slow to require therapy. We also included tachyarrhythmia caused by lead problem.12)
Statistical analysis
The results are reported as the mean±standard deviation for numerical variables, and as frequencies and percentages for categorical variables. The independent t-test was used to compare group continuous variables and the Chi-square test or Fisher's exact test was used to compare the categorical variables between groups. Incidences of all-cause death and the frequency of shock therapies (including appropriate and inappropriate shocks) in each group were determined using Kaplan-Meier event curves, and compared using log-rank tests. A multivariate logistic regression analysis was used to identify the predictors of all-cause death in the total study population. SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for the statistical analyses, and statistical significance was accepted for p value<0.05.
Results
Baseline characteristics
A total of 146 patients were evaluated. The mean age and mean LVEF were 63 years old and 30%, respectively, with an average follow up of 3.5 years (range, 9 months to 170 months). The patients were classified into two groups, based on the etiology and device indication. A comparison of the clinical characteristics between ischemic CMP and non-ischemic CMP, and a comparison between the primary prevention group and secondary prevention group, are summarized in Table 1 and 2, respectively.
Ischemic CMP vs. non-ischemic CMP
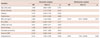
More male patients (56 males vs. 43 females, p=0.021) as well as more patients who had a history of a previous MI (45 patients vs. 8 patients, p<0.001) were present in the ischemic CMP group. Also, the average age was higher in the ischemic CMP group (65.6 years vs. 60.2 years, p=0.028). Patients who had experienced previous heart failure (HF) were more frequently observed in the non-ischemic CMP group (60 patients vs. 46 patients, p=0.009). The proportion of ICD implantations was higher in the ischemic CMP group, whereas the proportion of CRT-D implantations was higher in the non-ischemic CMP group (94.5% vs. 74.0%, and 26.0% vs. 5.5%, p=0.001 for all, Table 1).
Primary prevention vs. secondary prevention
Patients with underlying HF were more common in the primary prevention group (94.4% vs. 65.5%, p<0.001). The LV end-diastolic and end-systolic measurements in the primary prevention group were greater, and the LVEF was significantly lower, compared to that in the secondary prevention group (Table 2). The proportion of ICD implantations was higher in the secondary prevention group than the primary prevention group, whereas the proportion of CRT-D implantations was higher in the primary prevention group (93.6% vs. 55.6%, and 44.4% vs. 6.4%, p<0.001 for all, Table 2).
Clinical outcomes
Shock deliveries
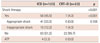
The overall ICD shock rate (not including ATP) was about 39.0%, regardless of the underlying etiology. No difference was observed in the appropriate shock rate between the ischemic- and non-ischemic CMP (27.4% vs. 28.7%, p=NS, Table 3). Appropriate shock therapies tended to be more frequently delivered in the secondary prevention group (31.8% vs. 13.9%, p=NS, Table 4). ICD shock therapies were significantly more frequent in the secondary prevention group (46.4% vs. 16.7%, p=0.002, Table 4), and the cumulative probability of a first appropriate shock therapy was significantly higher in the secondary prevention group (log rank p=0.015, Fig. 2). During the first year after the ICD implantation, a higher rate of the first appropriate shock therapy was delivered (Fig. 3). There was no significant difference in the mortality rate, cause of death, or mode of death between the two groups (Table 3, 4). When classified according to the device category (ICD group vs. CRT-D group), shock therapies were observed in half the patients in whom an ICD was implanted (45.5 % vs. 4.3 %, p<0.001, Table 5) and only one patient with a CRT-D experienced an inappropriate shock therapy.
Inappropriate shocks
Inappropriate shock therapy rate was insignificantly higher in the ischemic CMP group than non-ischemic CMP group (15.1% vs. 6.9%, p=NS, Table 3), and higher in the secondary prevention group than primary prevention group (14.5% vs. 2.8%, p=NS, Table 4, Supplementary Fig. 1 in the online-only Data Supplement.). In the 146 subjects evaluated, regardless of the etiology and indication, the link between inappropriate shocks and death was explored. Although the death rate was higher in patients who had inappropriate shocks, there was no significant difference between them (34.1% vs. 18.8%, p=NS, Fig. 4 and Supplementary Fig. 2 in the online-only Data Supplement.).
Mortality
The all-cause mortality was 24.7% during the mean follow-up period; 15.8% were due to cardiac causes and 8.9% due to non-cardiac causes. There were no significant differences in the all-cause death, cardiac death, or mode of death between the groups, according to the etiology and indication (Table 3, 4). In the Kaplan-Meier survival probability estimates based on the survival curves, there was no difference in the total cumulative survival rate between the groups (primary prevention vs. secondary prevention, ischemic CMP vs. non-ischemic CMP, appropriate shock vs. inappropriate shock, ICD vs. CRT-D, presence of shock therapy vs. no shock therapy; Fig. 4 and Supplementary Fig. 3, 4 in the online-only Data Supplement). In a univariate analysis for predicting the all-cause mortality in these patients, gender female, a lower body mass index (BMI), and history of a previous hospitalization were significant prognostic factors. In a multivariate logistic regression model, a lower BMI (≤25 kg/m2) and history of a previous hospitalization were independent prognostic factors of death (Table 6).
Discussion
In the community-based device registry of the Yeongnam province of Korea, ICDs and CRT-Ds were more frequently implanted for secondary prevention than primary prevention. The main findings of this study were: 1) the overall ICD shock rate during 3.5 years of follow-up period was about 39.0%, including 11.6% that were inappropriate shocks, 2) appropriate shock therapies were more frequently delivered in the secondary prevention group; the cumulative first appropriate shock rate in the secondary prevention and primary prevention groups was 31.8% and 13.9%, respectively, both of which seemed to be lower than that in the previous ICD clinical trials based on Western populations, 3) no significant differences in the appropriate shock rate between ischemic- and non-ischemic CMP were found.
In the evaluation of whether the current ICD guideline for primary prophylaxis against sudden cardiac death are appropriate for the Korean population with severe HF, it was concluded that the primary prevention criteria for ICD implantations would also be appropriate in both the ischemic- and non-ischemic CMP patients, since Korean patients with severe HF in both the ischemic- and non-ischemic-CMP groups had an all-cause mortality and risk of sudden cardiac death comparable to the patients in the Multicenter Automatic Defibrillator Implantation Trial-II (MADIT-II) and Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) standard therapy groups.14)
Few studies on the efficacy of ICDs in Korean patients have been conducted. Recently published data from a single center in Korea reported that the ICD shock rate during 3 years of follow-up was 42.6%; however, in that study the subjects were heterogeneously composed of various cardiomyopathic diseases and genetic arrhythmia syndromes.15)
The rate of shock therapies during the follow-up period
During the 3.5 years of follow-up, the overall ICD shock rate in this study was about 39.0%, regardless of the underlying etiology. In case of secondary prevention, shocks were delivered to almost half of the study subjects (46.4%), which was in contrast to the 16.7% in the primary prevention group. In the 3-year representative ICD trial for secondary prevention, i.e. the Antiarrhythmics vs. Implantable Defibrillators trial, the cumulative percentage of patients with any activation of the defibrillator, either antitachycardia pacing or shocks, was 85% in patients with VT and 69% in patients with VF.4) Further, in the 4-year Canadian implantable defibrillator study (CIDS), the cumulative risk of receiving an ICD shock was 65.4%.6) With regards to the ICD firing rate in the primary prevention trials, 60% of the patients with an ICD had a shock discharge within 2 years after enrollment in the first Multicenter Automatic Defibrillator Implantation Trial,3) with the shock rate reaching 36% at 3 years in the second MADIT-II.8) The actuarial incidence of a first shock from the ICD was 50% at 1 year and 57% at 2 years in the Prophylactic use of ICDs in patients at high risk for ventricular arrhythmias after Coronary-artery bypass graft surgery trial (CABG Patch).5) The shock rate was 39.3% (including a 17.9% appropriate shock rate) in the DEFINITE trial, in which the follow-up lasted 29 months.9) Conversely, 31% of the ICD group received shocks for any cause (including 21% with appropriate ICD shock therapies, and ATP was not used) in the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT), and this cumulative shock rate occurred over a mean of 45.5 months.10)
Taken together, in comparison with the previous trials,3)8)9) the overall shock rate in our study was considerably lower even with a longer follow-up period. Thus, extrapolating these findings of patients residing in the Yeongnam province of Korea, we can cautiously assess that all Korean patients might have a lower incidence when compared with the patients of Western countries, in the same disease category.
Furthermore, patients with a CRT-D device had a lower shock rate compared to that of the patients with ICDs in our study. The reason is unclear, but we speculate that it was driven by improving the LV function by the negative LV remodeling effect of the CRT.16)
The issue of inappropriate shocks
In our study, the inappropriate shock therapy rate was numerically higher in the ischemic CMP group and the secondary prevention group. The rate of inappropriate shock therapies also seemed to be lower than that of the previous trials of Western populations.11)12)17)18)19)20)21)22) Regardless of the etiology and indication, our study patients undergoing inappropriate shocks had a numerically but insignificantly higher death rate than those who did not. However, the MADIT-II trial results had revealed that prior occurrences of inappropriate shocks doubled the risk of total mortality.11) This can be explained by a potential direct mechanical, arrhythmogenic effect of the shock itself, and the presence of AF, which is the cause of both inappropriate shocks and an increased risk of mortality. We speculated that this difference arose due to the small number of our patient population.
Mortality
During the follow-up period, the all-cause mortality was 24.7%, which included 15.8% due to cardiac causes and 8.9% due to non-cardiac causes. In comparison, in a representative secondary prevention trial over a mean follow-up of 18 months, the crude death rates were 15.8% in the ICD group, and 24.0% in the antiarrhythmic-drug group.4) The mortality rate of the ICD group in the primary prevention trials varied: 7.9% over 29 months in the DEFINITE trial,9) and 15.7% and 14.2% in the first and second MADIT trials, respectively.3)8) In the SCD-HeFT,10) the mortality rate in the ICD group was 22%. In short, the mortality rate of our current study seemed to be similar to or higher than that reported in the ICD group in the previous trials due to inexplicable reasons.
Limitations
Although this study gave us a fascinating glimpse into the activation or efficacy of ICDs implanted in Korean HF patients for primary and secondary prevention, we are as yet unaware of the actual efficacy or life-saving effects of an ICD therapy due to the following reasons: First, the number of patients enrolled was quite small and lacked a control group. Second, device programming settings for the VT/VF therapy were not standardized in each center, and therefore the shock therapy might not have been delivered in the same ICD therapy zone. As shown in the MADIT-RIT (Multicenter Automatic Defibrillator Implantation Trial–Reduce Inappropriate Therapy trial) and PainFree SST (SmartShock Technology) trial, which demonstrated a reduction in the inappropriate and appropriate ICD therapies and mortality according to the ICD programming and the adoption of novel enhanced detection algorithms,18)22) the frequency of ICD therapy varied depending on the ICD programming. Third, we need to know that a shock therapy is a surrogate marker of a lifesaving effect, and not all appropriate and successful shocks are life-saving. Finally, we could not provide any information on the concomitant medications, especially the beta blockers used, and information about the presence of AF, other SVTs, and/or abnormal sensing as a cause of inappropriate shocks.
Though it is quite difficult to draw a firm conclusion because of the various reasons mentioned above, this study gives us a fascinating glimpse into the activation or efficacy of ICDs implanted in the Korean population for both primary and secondary prevention.
In conclusion, in this In this multicenter regional registry data, most cases of ICD implantations were performed for secondary prevention. The ICD shock therapy rate was higher in the secondary prevention group than in primary prevention group, in both ischemic and non-ischemic CMP patients. Both the appropriate and inappropriate shock rates seemed to be lower than that of the prior trials based on Western populations. However, additional randomized prospective trials in a large population are needed to determine the true efficacy of ICD therapy in Korean patients with LV dysfunction.








 XML Download
XML Download