

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Approximately 40% to 65% of patients presenting with ST-segment elevation myocardial infarction (STEMI) have multivessel coronary artery disease (MVD), which is strongly correlated with a higher frequency of major adverse cardiac events (MACEs).1)2) According to the current guidelines, percutaneous coronary intervention (PCI) of the nonculprit vessel in patients with STEMI and MVD should not be performed at the time of primary PCI except in patients with cardiogenic shock.3) However, 3 approaches are used in clinical PCI strategy in patients with STEMI and MVD including, simultaneous PCI of the nonculprit vessel during primary PCI, a staged PCI of the nonculprit vessel after primary PCI, and a conservative approach with PCI for the nonculprit vessel only in cases of persistent ischemia or a positive result on an ischemia-provoking test.4) However, no studies have investigated the optimal timing of PCI for the non-culprit vessel in patients with STEMI and MVD, and current guidelines also do not recommend the optimal time frame of staged PCI in patients with STEMI with MVD.
Dangas et al.5) assessed the optimal timing of staged PCI in patients with MVD on the basis of the opinions of interventional cardiology experts. They reported that about 80% of the interventional cardiologists surveyed recommend staged PCI at a later date in patients with STEMI, whereas 37% recommend late staged PCI in patients with non-STEMI (NSTEMI). Regarding the timing of staged PCI, 62% of the cardiologists suggested a time frame of >2 weeks for the staged PCI in patients with STEMI and 55% recommend >2 weeks in patients with NSTEMI; in addition, the heterogeneity in decision making is due to many factors that can affect the decision to perform staged PCI.
The optimal timing of a staged PCI for nonculprit vessels and the impact on clinical outcomes of different time frames of staged PCI remain unclear. The purpose of this study was to investigate the current status of the staged PCI procedure in STEMI patients for nonculprit vessels and the impact of different time frames of staged PCI on the incidence of MACEs on the basis of a Korean multicenter registry.
Subjects and Methods
Study population
A total of 5025 patients with AMI from 9 centers of 2 universities were registered in the prospective COREA-AMI registry (Convergent Registry of Catholic and Chonnam University for Acute myocardial infarction [MI]) from January 2004 through December 2009. A trained study coordinator collected data by using a standardized protocol; and the ethics committee of each participating hospital approved the study protocol.
From 5025 AMI patients, 2102 NSTEMI patients were excluded. From 2923 STEMI patients, we excluded 309 patients who treated by thrombolytic therapy, 1410 patients with single vessel disease, 301 without significant stenosis, 31 patients who underwent failed PCI and 14 patients with cardiogenic shock. Among these, 753 patients who were treated by multivessel PCI strategy were finally included in our study.
The eligible patients had been diagnosed with STEMI at admission on the basis of clinical presentation, increased cardiac biomarkers, and 12-lead electrocardiographic findings. MVD was defined as critical stenosis (>70% of diameter stenosis) in at least 2 major epicardial coronary arteries on a diagnostic coronary angiogram. These patients were divided into 3 groups according to the time interval from initial PCI to second staged PCI: group 1 (multivessel PCI of simultaneous culprit and nonculprit vessels during primary PCI, n=316), group 2 (staged PCI of nonculprit significant vessel within 1 week after primary PCI, n=360), and group 3 (staged PCI performed 1 week after primary PCI, n=77). Principal exclusion criteria were as follows: 1) hemodynamic instability and history of coronary artery bypass grafting; 2) history of bleeding diathesis, conditions predisposing to hemorrhagic risk, or refusal to receive blood transfusions; 3) stroke or transient ischemic attack within 6 months; and 4) recent or known platelet count <100000 cells/mm3 or hemoglobin <10 g/dL.
Definitions and coronary angiography
For all subjects, we assessed clinical and diagnostic parameters including medical history of coronary artery disease and smoking, results of laboratory tests, and 2-dimensional echocardiographic results. The lipid profile, levels of troponin I, serum creatinine clearance, and levels of high-sensitivity C-reactive protein were assessed. STEMI was defined as new ST-elevation in at least 2 contiguous leads, measuring >0.2 mV in leads V1-V3 or >0.1 mV in all other leads or presumably new-onset left bundle branch block.
Diagnostic coronary angiography and PCI were performed after premedication with aspirin (100 to 300 mg) and clopidogrel (300 to 600 mg). Coronary angiography was performed through the femoral or radial artery. A 50- to 70- U/kg dose of unfractionated heparin was infused before or during PCI to maintain an activated clotting time of 250 to 300 s. After PCI, 100 mg aspirin and 75 mg clopidogrel were prescribed daily as maintenance doses. Angiographic data were obtained visually by PCI operators at the investigative site. Mandatory data fields included the identification of the infarct-related artery (IRA), its pre-interventional flow, and the maximum percentage stenosis in the left main, left anterior descending, left circumflex, and right coronary artery. Flow in the IRA was graded by using the thrombolysis in myocardial infarction flow grade visually. Coronary stents were deployed after prior balloon angioplasty, and platelet glycoprotein IIb/IIIa inhibitor was administered in patients who showed large thrombotic burdens in angiography according to the decision of the operator.
Study endpoints
The study endpoint was the impact of different time frames of staged PCI on the composite incidence of MACEs during 3.4 years of follow-up after discharge (median; interquartile range, 1.9-4.7 years). MACEs included the composite of all-cause mortality, non-fatal MI, and repeat PCI including target lesion revascularization (TLR), target vessel revascularization (TVR), and non-target-vessel revascularization (non-TVR). Non-fatal MI was defined as recurrent symptoms with new electrocardiographic changes reflecting MI or increased cardiac biomarkers at least twice the upper normal limit. TLR was defined as PCI for restenosis or other complications of a lesion that were treated from 5 mm proximal and 5 mm distal to the stent. TVR was defined as repeated PCI for any segment of the entire coronary artery proximal and distal to the target lesion. Stent thrombosis (ST) was defined as definite and probable stent thrombosis according to the Academic Research Consortium definition.6)
Statistical analysis
The statistical analyses were performed with SPSS for Windows, version 21.0 (IBM SPSS Inc., Chicago, IL, USA). Continuous variables were presented as the mean value±standard deviation (SD) and differences were investigated by use of one-way analysis of variance (ANOVA). Discrete variables were presented as percentages and relative frequencies and comparisons were made by using Chi-square tests. A logistic regression model was used to determine independent predictors of 3-year MACEs and all variables considered relevant to predicting MACEs were tested. Composite endpoints were compared with the Kaplan-Meier method to estimate MACE-free survival in the 3 groups and statistical difference was analyzed by log-rank test. All variables were considered significant when the p-value was <0.05.
Results Baseline characteristics and angiographic findings
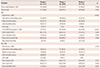
As shown in Table 1, the baseline characteristics were similar in the three study groups. There were no significant differences in demographics, atherosclerotic risk factors, or laboratory findings among the three groups except for a higher level of high-sensitivity C-reactive protein in group 3 (p=0.001). During the in-hospital period, patients received essential medical treatment including antiplatelet agents, beta-blockers, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers. After discharge, the patients continued to receive the optimal medications, which were presented in Table 2.
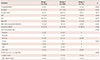
The coronary angiographic and procedural characteristics in each group were shown in Table 3. The most common culprit vessel in group 1 was the left anterior descending artery, whereas the right coronary artery was a major culprit vessel in half of the staged PCI cases (groups 2 and 3). An initial thrombolysis in myocardial infarction (TIMI) flow grade of zero was seen less often in group 1 than in groups 2 and 3. Angiographic and procedural findings of nonculprit vessels were comparable among the 3 groups. Time distribution from primary to second staged PCI in STEMI patients with multivessel disease described in Supplementary Fig. 1 in the online-only Data Supplement.
Clinical outcomes during follow-up
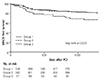
We also compared composite MACEs during clinical follow-up in the three study groups (Table 4). There were no significant differences in mortality, non-fatal MI, or repeat PCI among the 3 groups. However, the incidence of composite MACEs tended to be greater in group 3 than in group 1 or group 2 (35.1% compared with 23.7% and 22.5%, respectively, p=0.063). The 3-year MACE-free survival in the 3 groups was shown in Fig. 1. The lowest MACE-free survival rate was seen in group 3 (log-rank p=0.032).
Predictors of 3-year MACEs
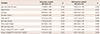
In the logistic regression model, independent predictors of 3-year MACEs were high Killip class, left ventricular ejection fraction <45%, and a timeframe of >1 week to staged PCI, as compared with simultaneous culprit and nonculprit vessel PCI during primary PCI (Table 5).
Discussion
The principal findings of the present study of patients with STEMI and MVD experiencing multivessel PCI were as follows. 1) There were no significant differences in individual endpoints between the groups, however staged PCI performed 1 week after the primary PCI in patients with STEMI and MVD was associated with increased 3-year composite MACEs, as compared with simultaneous culprit and nonculprit artery intervention during the index PCI, and 2) in real clinical practice in Korea, many patients who underwent multivessel PCI received simultaneous culprit and nonculprit PCI during the primary PCI.
According to the current guidelines for the management of patients with STEMI, PCI should not be performed in a non-IRA at the time of the primary PCI. However, the current guidelines do not suggest the optimal timing of PCI of the nonculprit vessel in patients with STEMI and MVD.3) Dangas et al.5) reported that only 2% of interventional cardiologists surveyed in the United States recommended nonculprit PCI in patients with STEMI and MVD at the time of the initial PCI, and about 80% of cardiologists surveyed recommended staged PCI at a later date. In a retrospective cohort study (a total of 37436 patients) reporting rates of all 3 PCI strategies for MVD in a registry population, culprit-only PCI was always the most often performed PCI strategy (30260 of 37436 patients, 80.8%), as compared with multivessel PCI (3887 of 37436 patients, 10.4%) and staged PCI (3289 of 37436 patients, 8.8%).7)
The results of the recent PRAMI study (Preventive Angioplasty in Acute Myocardial Infarction) showed that multivessel PCI during the index procedure provided better clinical outcomes than culprit-only PCI.8) Nevertheless, it is still unclear whether multivessel PCI during the index procedure in STEMI patients is better than a staged PCI, and the ongoing trials and clinical guidelines do not specify a fully defined PCI strategy for STEMI patients with MVD. Many interventional cardiologists think that primary PCI is associated with an increased risk of potential complications and that significant nonculprit lesions should be treated by a planned staged procedure after stabilization of the patient's condition. A meta-analysis performed by Vlaar et al.9) favored a staged PCI strategy with complete revascularization in patients with STEMI. Among the different interventional strategy groups in that study, staged PCI was associated with lower short- and long-term mortality, as compared with culprit-only PCI and multivessel PCI during the primary PCI. Hannan et al.10) showed that STEMI patients who underwent staged multivessel PCI within 60 days of the index procedure had a significantly lower 1-year mortality rate than patients who underwent culprit vessel PCI only. Subgroup analysis in the Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI) Trial compared culprit-only PCI with staged PCI in patients with STEMI. The results indicated higher 1-year mortality, cardiac death, and stent thrombosis in the culprit-only PCI group than in the staged PCI group. Furthermore, there was a trend toward higher 1-year MACEs in the former group.11) Jensen et al.12) also reported that in patients with STEMI, staged PCI within 60 days of the index hospitalization could reduce 1-year mortality compared with that in patients who undergo culprit-only PCI during the primary PCI. Nevertheless, many questions remain about staged PCI, especially about the optimal timing of nonculprit PCI. In clinical practice, factors such as impaired renal function, complex lesions, high contrast media volume, high radiation doses, a hemodynamically unstable state, and a patient's devitalized physical status can influence the decision of multivessel PCI timing in patients with AMI and MVD.13)14) Generally, interventional cardiologists tend to delay secondary staged PCI in patients with these conditions. The majority of cardiologists (62%) favor staged PCI of the nonculprit artery after primary PCI in a timeframe >2 weeks in STEMI patients.5)
According to our data, 47.7% of patients underwent a second staged PCI of the non-IRA within 1 week after primary PCI. The reason for the increased risk of MACEs in the later staged PCI group (>1 week) in the current study is unclear. It is possible that multivessel PCI in the acute phase reduces ischemia and improves survival; and relatively early revascularization of the non-IRA may be helpful for improving regeneration of the infarcted myocardium, for recovery from acute myocardial infarction, maintenance of cardiac function, and improved long-term clinical outcomes.15)16)
Limitations
First, this study was not a randomized controlled trial and the retrospective analysis could have introduced selection bias. Although we adjusted for numerous confounding factors, it is possible that other potent variables that we did not adjust for were associated with clinical outcomes. Furthermore, the definitive cause of the unfavorable outcomes in the group that underwent late (>1 week) staged PCI is uncertain. Second, our study lacked data about the completeness of PCI in the diseased vessels. Complete revascularization is associated with reduced cardiovascular mortality in patients with coronary artery disease;17) however, our study did not consider the effect of complete revascularization. Third, our registry also lacked data on the complexity of the coronary anatomy and myocardial viability before staged PCI. The synergy between percutaneous coronary intervention with taxus and cardiac surgery (SYNTAX) score is designed to predict outcomes related to anatomical characteristics, such as the dominant artery, number of lesions, other lesion characteristics, and to a lesser extent, the functional risk of occlusion of any segment of the coronary artery in patients with MVD. A high SYNTAX score indicates more complex disease and is associated with poorer cardiovascular outcomes.18)19) Myocardial viability by cardiac magnetic resonance imaging or myocardial nuclear imaging and functional evaluation by fractional flow reserve should be considered before a second staged PCI; however, our registry did not contain this information.20)21)
In conclusion, in patients presenting with STEMI and MVD, secondary staged PCI of non-IRA was performed within one week in half of cases. Deferred staged PCI after one week index PCI was associated with the highest MACE, as compared to both simultaneous multivessel PCI and early staged PCI <1 week. Few studies focus on the optimal timing of staged PCI in patients with STEMI and MVD. Therefore, further large-scale randomized trials are needed to confirm these findings.


 XML Download
XML Download