

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A single coronary artery (SCA) is an extremely rare congenital anomaly of the coronary circulation, often associated with other congenital cardiac malformations and frequently presenting with angina.1) The incidence of SCA is only 0.024% to 0.066% in the general population undergoing coronary angiography.2) We report a case with a congenital anomalous right coronary artery, extending from the left circumflex artery, with stenosis in the proximal left anterior descending artery. The anomaly was successfully treated by stenting.
Case
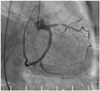
A 77-year-old woman presented with complains of progressive effort-related chest pain for 20 days. She had no particular medical history. On physical examination, the blood pressure was 130/70 mmHg, and her pulse rate was 76 beats/min. Her heart sounds were normal and no murmur was heard. The electrocardiogram displayed normal sinus rhythm without any ST depression or T-wave inversion. The transthoracic echocardiography demonstrated normal hemodynamics with a normal pattern of contractility. The coronary angiography showed that the left coronary artery originated normally from the left sinus of Valsalva, but revealed a 90% tight stenosis at the proximal portion of the left anterior descending artery (Fig. 1). The figure of the left circumflex artery was unique, in that an aberrant branch extended from the distal left circumflex artery, which crossed the crux and continued to the right atrioventricular groove, covering the territory of the right coronary artery (Fig. 2A). After several failed attempts to engage the right coronary artery, we performed aortography using a power injector to exclude high take-off of the right coronary artery. This also confirmed the absence of the right coronary ostium (Fig. 2B). Without delay, we successfully deployed a 4.0×12 mm zotarolimus-eluting stent (Endeavor™, Medtronic Vascular, Santa Rosa, CA, USA) at the left anterior descending artery, after intravenous injection of 5,000 IU heparin. Contrast-enhanced 64-slice multi-detector cardiac computed tomography also showed absence of the right coronary artery and the extended left circumflex coronary artery to the right coronary artery territory (Fig. 3). Before discharge, a technetium-99m single photon emission computerized tomography (SPECT) study demonstrated noregional any regional perfusion defect. The stent was intact in an 8-month follow-up coronary angiography.
Discussion
The definition of an isolated SCA is when only one coronary artery originates from one of the sinus of Valsalvas, with this supplying the entire heart, regardless of its distribution. This type of congenital anomaly is very rare, with a reported incidence of only 0.024% to 0.066% in the general population undergoing coronary angiography.2) In Korea, the incidence is even less. One retrospective study showed only 4 patients (0.00025%) diagnosed with SCA among 16,099 patients, who underwent coronary angiography.3) In 1979, Lipton et al.2) proposed a very useful angiographic classification, further modified in 1990 by Yamanaka and Hobbs.4) According to the Lipton classification, our patient would be categorized in the L-I group, where L implies the ostium is located in the left sinus of Valsalva.
SCA is commonly associated with other congenital anomalies, such as transposition of the great vessels, coronary arteriovenous fistula, or bicuspid aortic valve.1) Its prognosis is usually benign, and it is known that SCA does not interfere with coronary perfusion. However, Yamanaka and Hobbs4) categorized SCA as a potentially serious anomaly in the analysis of 1,686 patients undergoing coronary angiography. Some reports have also indicated that significant symptomatic ischemic heart disease developed in 15% of SCA patients.5) It is reasonable to think that the clinical meaning and risk of SCA depends on the degree of stenosis and position of the stenotic lesion. If the stenosis develops at the proximal portion of the originated artery, it can cause grave clinical events, and caution is needed when performing intervention.
An interesting case report, clinically presented as acute myocardial infarction at the middle portion of the anterior descending artery, revealed that the right coronary artery originated from the middle portion of the left anterior descending artery, on the distal part of the culprit lesion, through the transverse branch.6) This patient was successfully treated with a stent. In another SCA case, the right coronary artery originated from the distal left circumflex artery and had a significant stenosis just at the take-off of the aberrant right coronary artery. This patient was successfully treated with coronary bypass surgery.7)
However, myocardial ischemia can develop without definite stenosis, due to coronary vasospasm,8) with slow controlled ischemia caused by its long travel distance, as one of the possible mechanisms. Consequently, if a patient complains of chest pain, but does not show causative lesions in SCA, the above possibility should be considered. It is necessary to check whether ischemia can develop by stress tests such as a treadmill test or a SPECT scan. In our patient, coronary angiography revealed a relatively slow flow and delayed contrast media washout in SCA, but did not show ischemia in a technetium-99m SPECT study.


 XML Download
XML Download