

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Situational syncope is characterized by loss of consciousness in particular situations such as with a cough, micturition, deglutition.1-3) This form of syncope is thought to account for 5% of syncopal episodes.2) Several cases of deglutition syncope have been reported to be successfully treated with a permanent pacemaker. However, there are few cases with an initial atrial fibrillation rhythm. Here, we report a case of deglutition syncope in a patient with permanent atrial fibrillation, who underwent permanent pacemaker implantation to prevent ventricular asystole during the episodes of deglutition syncope.
Case
A 62-year-old man was referred to our hospital because of recurrent syncope. The patient had syncopal episodes while drinking fluids starting seven years ago. He reported the feeling of a foreign body sensation at his mid sternal area after drinking a cold beverage, and then suddenly lost consciousness. The duration of unconsciousness was a few seconds. There were no seizure-like movements or incontinence during the attack, and he felt no numbness or motor weakness before or after the events. The patient reported more than twelve episodes of syncope before presenting to the cardiology outpatient clinic at Samsung Medical Center. A skin laceration was noted on his forehead from the last episode of syncope.
The patient was diagnosed with atrial fibrillation seven to eight years ago, and had been taking warfarin since then. He was also diagnosed with diabetes mellitus three years ago. His diabetes was well controlled with oral hypoglycemic agents.
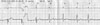
The initial electrocardiogram (ECG) showed atrial fibrillation with a ventricular response of 60-70. His echocardiography did not show any significant abnormality of the heart except bilateral atrial enlargement. On the second day of admission, he felt a globulous sensation at the mid esophagus after drinking a cold beverage in the sitting position, and then lost consciousness. His telemetry ECG monitoring at that time showed abrupt ventricular asystole that was sustained for 12 seconds (Fig. 1). Another episode of syncope occurred on the same day while drinking. His telemetry ECG monitoring showed ventricular asystole for 4 seconds (Fig. 2).
We evaluated the esophagus with a barium swallow; there were no abnormal findings in the esophagus. On the treadmill test, his heart rate and blood pressure increased to 176/min and 218/83 mmHg, respectively. The head-up tilt test three months before admission was negative; the head-up tilt test was repeated. During the repeated head-up tilt test, provocation with drinking a cold beverage showed no significant pause or hypotension.
The patient underwent permanent pacemaker implantation of a VVI type pacemaker to prevent ventricular asystole. After implantation of the permanent pacemaker, there were no further episodes of syncope after drinking a cold beverage (Fig. 3).
Discussion
Deglutition syncope was first documented in 1906 by Meckenzie.3) Since then, it has been reported in patients evaluated by many different medical disciplines including: cardiology, gastroenterology, neurology, and otolaryngology. The vasovagal reflex between the heart and the esophagus is thought to be associated with deglutition syncope via the vagus nerve, where a signal from the mechanoreceptors in the esophagus is sent to the cardioinhibitory center in the medulla; the medulla then delivers the signal to the sino-atrial or atrioventricular (AV) nodes via the vagus nerve again, and the result is a variety of brady-arrhythmias.4)5) Sapru et al.3) reported a case supporting this theory. They found that an esophageal lesion caused syncope while swallowing in a young female patient by repeating esophageal ballooning with ECG monitoring; the patient had eight episodes of syncope while swallowing. They removed all branches of the vagus and sympathetic nerves entering the affected esophagus. After the surgery the patient had no more syncope. The vagus nerve is the key route in the afferent and efferent limbs of deglutition syncope. Inhibition of the vagal reflex with medication has been tried for treatment in some cases. Intravenous atropine injection abolished an AV block in some provocation tests.6)7) In another case of AV block after swallowing, oral atropine sulphate tablets were tried. However, the symptoms were not relieved fully and there were intolerable side effects.3)
Deglutition syncope is often combined with esophageal disorders such as a hernia, stricture, achalasia, diverticulum, and esophageal spasm.8) Gordon et al.9) reported syncope with paroxysmal atrial fibrillation provoked by esophageal reflux. The patient was treated with a proton pump inhibitor. Maekawa et al.10) reported a patient with deglutition syncope that had a very large hiatal hernia compressing the left atrium after eating a large meal. If deglutition syncope is suspected by the patient's history, an evaluation for esophageal abnormalities should be performed. The patient in our case had no abnormality of esophageal function or anatomic structure, as shown by the barium swallow. Implantation of a permanent pacemaker successfully treated the symptoms of AV block and ventricular asystole with swallowing. In a case of deglutition syncope without ECG changes, the pacemaker does not improve symptoms.11) Therefore, prior to implantation of a permanent pacemaker, ECG documentation of an AV block or pause should be obtained.
Deglutition syncope with atrial fibrillation has been previously reported. Gordon et al.9) reported that the occurrence of paroxysmal atrial fibrillation with a rapid ventricular response caused syncope after swallowing. Armstrong et al.11) reported a case with a slow idioventricular rhythm with permanent atrial fibrillation associated with syncope after drinking. However, our patient had ventricular asystole that caused syncope after drinking a cold beverage; after implantation of the permanent pacemaker the patient did not lose consciousness.


 XML Download
XML Download