

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Patients with coronary artery disease and chronic hypoperfusion develop persistent left ventricular (LV) dysfunction that returns to normal after revascularization, the so called myocardium hibernation.1)2) The distinction between ventricular dysfunction arising from either myocardial fibrosis or underperfused but viable hibernating myocardium has important therapeutic and prognostic implications.3)
For the diagnosis of viable myocardium, several authors4-6) have used dobutamine stress echocardiography (DSE) and demonstrated the usefulness of the color Doppler tissue image (DTI) M-mode with DSE for the prediction of reversible dysfunction early after reperfusion in patients with acute myocardial infarction.
In two experimental animal studies, postsystolic shortening during acute coronary occlusion was correlated to recovery of LV systolic function measured early and late after reperfusion.7)8) These results suggested that postsystolic motion (PSM) may be related to an active process reflecting myocardial viability. Although different methods have revealed PSM of the ischemic myocardial segments as regional asynchrony of myocardial wall motion during acute ischemia,9)10) there are a few reports concerning PSM and its diagnostic value for the improvement of dysfunctional myocardium during DSE after successful revascularization. Therefore, this study was performed to determine whether PSM during DSE predicts functional recovery of dysfunctional myocardium after successful percutaneous coronary intervention (PCI) in patients with chronic stable angina.
Subjects and Methods
Patient population
We enrolled 30 patients diagnosed with chronic stable angina with dysfunctional myocardium in the left anterior descending coronary artery (LAD) territory, who underwent a successful PCI on the LAD territory by routine methods. A dysfunctional myocardium was defined by wall motion abnormality in the LAD territory. DSE was performed in all 30 patients 1 month after PCI. The patients were divided into two groups according to improvement of dysfunctional myocardium in the LAD territory 6 months later. Exclusion criteria included: prior PCI or myocardial infarction, acute coronary syndrome, a significant lesion at other coronary arteries, dilated cardiomyopathy, significant valvular disease, arterial and ventricular arrhythmia, pacemaker implantation, bundle branch block and an LV ejection fraction below 45%. Signed informed consent was obtained from all individuals before enrollment into the study.
Resting and Dobutamine Stress Echocardiography with Doppler myocardial imaging
Echocardiographic studies were performed using the commercially available Vivid 7 echocardiography (General Electronics Corp., Horten, Norway) imaging system and a 3.5 MHz transducer equipped with Doppler myocardial imaging (DMI) imaging.
A standard dobutamine stress protocol was used starting at a dobutamine infusion rate of 5 µg/min/kg body weight, and thereafter increasing the dosage every 3 minutes to 10, 20, 30, and 40 µg/kg/min.11) Apical 2 and 4 chamber views were used for the assessment of longitudinal myocardial motion by DMI.
The DMI study during DSE was performed using a real-time color DMI system. At frame rates of >100 frames/s, this system has a high temporal resolution of <20 ms. All images were saved to magneto-optical disks for off-line analysis.
Echocardiographic analysis
Off-line visual assessment of echocardiographic images was performed independently by two investigators (KSK, LYS), blinded to the functional recovery data. Analysis of the stress test, including wall motion score index (WMSI), was confined to the LAD artery territory. The apico-septal and mid-septal segments in the apical four-chamber view and basal anterior segment in the apical two-chamber view were selected for assessment of WMSI and DMI data of the LAD territory.12) The average value from three beats was taken for each measurement.
To evaluate WMSI in the LAD artery territory, each ventricular segment of the LAD artery territory was scored on a five-point scale: 1=normal, 2=hypokinesis, 3=akinesis, 4=dyskinesis and 5=aneurysm. Following the recommendations of the American Society of Echocardiography,13) a regional WMSI was calculated for each patient as the sum of the scores of the segments in the LAD artery territory divided by three. Functional recovery of dysfunctional myocardium was defined as an increase in WMSI at 6-month follow-up echocardiography.
To assess DMI at the LAD artery territory during DSE, peak systolic velocity, peak velocity of PSM, peak velocity of early ventricular filling, and peak velocity of atrial contraction were determined. PSM was defined as a positive wave appearing after the curve of systolic ejection had reached the zero line (Fig. 1). The inter- and intra-observer concordances of PSM were, respectively, 89 and 91% in our echocardiographic laboratory.
Statistical analysis
The Statistical Package for Social Science 12.0 (SPSS inc., Chicago, IL, USA) statistical software package was used for all calculations. Data are presented as means±standard deviation (SD) for continuous variables and as percentages for categorical data. DMI data were analyzed using an unpaired Student's t-test. Categorical data and proportions were analyzed using the Chi-square test. Cut-off values for DMI during low-dose DSE for discriminating the presence from the absence of functional recovery were derived from receiver-operating characteristics curves as the points with the highest sum of sensitivity plus specificity; the corresponding areas under the curves were obtained. A p<0.05 was regarded as statistically significant.
Results
Demographic characteristics
Table 1 presents the demographic characteristics of the study populations. There were no differences in age or gender between the groups. In addition, there were no differences in cardiovascular risk factors such as obesity, history of smoking, and diabetes between the groups except for history of hypertension. Medications taken during the 6-month follow-up period were not different between the groups. However, by definition, the regional WMSI in the group where functional recovery was present was significantly decreased compared with that of the group where functional recovery was absent (p<0.05).
Myocardial Doppler parameters during dobutamine stress echocardiography
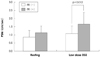
Myocardial Doppler parameters, including peak systolic and diastolic velocity of resting, low and high dose DSE were not different between the functional recovery groups (Table 2). However, PSM of low dose DSE in the presence of functional recovery was significantly increased compared to the group with an absence of functional recovery (Fig. 2). When comparing PSM according to functional recovery, 1.2 cm/sec was found to be applicable as a cut-off value for differentiating between presence and absence of functional recovery; this cut-off was associated with 73% sensitivity and 73% specificity (Fig. 3).
Discussion
This study evaluated the efficacy of myocardial Doppler imaging during low dose DSE evaluated at one month in dysfunctional myocardium after successful PCI in patients with chronic stable angina.
Postsystolic thickening or motion of myocardium is a myocardial contraction that develops during late systolic or early diastolic phase, and PSM can be considered not only as a marker of acute ischemia but also as a marker of successful myocardial reperfusion in an animal model.14)15)
Several authors have reported that PSM is a useful marker for viability or functional recovery after reperfusion in obstructive coronary artery diseases like acute myocardial infarction and chronic occlusive disease. Hosokawa et al.16) demonstrated that postsystolic shortening in patients with acute anterior myocardial infarction correlates with subsequent recovery of systolic function by ventriculography after revascularization. In addition, Song et al.17) reported that PSM detected by DMI in the infarct territory was related to peri-infarction ischemia or viability at DSE.
In the case of chronic coronary artery disease, Wong et al.18) demonstrated that post-ejection shortening assessed by radionuclide ventriculography causes regional post-systolic emptying, and this correlates with post-revascularization improvement in regional wall motion. Barletta et al.19) reported that regions with PSM were viable and showed a moderate decrease in coronary perfusion. In contrast, Lim et al.20) stated recently that PSM is not a specific marker of viability in chronic LV dysfunction and that delayed myocardial shortening may be associated with scarred segments.
However, several authors suggest the efficacy of PSM during DSE in coronary artery disease. Celutkiene et al.12) reported that the peak velocity of PSM during DSE was the most accurate index of induced ischemia (sensitivity 73-100%, specificity 82-97%). Akutsu et al.21) demonstrated that functional recovery in the stunned myocardium was predicted by DSE performed 1 week after early reperfusion following acute myocardial infarction. Moreover, Rambaldi et al.22) observed that the ratio of ejection phase shortening and post-systolic shortening velocity during DSE could predict a death-free outcome during long-term prospective follow-up after surgical reperfusion in patients with severe LV dysfunction. In our study, PSM during DSE in patients with chronic coronary artery disease and functional recovery at follow-up was increased compared to that in patients with no functional recovery after successful reperfusion of an occluded coronary artery.
The major value of assessing myocardial viability is to select patients who will benefit from revascularization. However, our study was conducted after reperfusion of the occluded coronary artery to diagnose the hibernating myocardium. We therefore propose that recognition and diagnosis of hibernating myocardium is important from a practical standpoint and may affect patient management.23)
The limitations of this study are as follows. First, because the study included a small number of patients and a limited follow-up period, large-scale and long-term follow-up studies are required to confirm our findings. Second, because the dysfunctional myocardium may have been injured more intensely,24) the recovery of dysfunctional myocardium may have been delayed more than 1 month after reperfusion. Third, angle dependency is another limitation of myocardial Doppler imaging, which has been reported to be minimized by the apical approach.25) In addition, myocardial Doppler imaging can evaluate only the longitudinal motion, but not the radial motion. Fourth, we estimated the wall motion of the LAD artery territory only in the apical two- and four-chamber views but, not in the apical three chamber view. Fifth, we assessed the dysfunctional myocardium only by WMSI but not by independent methods, including scintigraphy and magnetic resonance imaging.
Nevertheless, the present results suggest that PSM during DSE predicts functional recovery of dysfunctional myocardium after successful PCI in patients with chronic coronary artery disease.




 XML Download
XML Download