

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aortic diseases are disorders of the aorta that include acute aortic syndromes, aortic aneurysms, atherosclerosis, inflammatory diseases, and aortic tumors. They can be detected early based on acute symptoms or diagnosed much later. Aortic diseases, particularly acute aortic syndromes, require the swift identification or exclusion of diseases, which affect patient prognosis.
Several imaging modalities have been used to determine the presence and progression of aortic diseases. Chest x-rays can detect abnormalities in aortic contour or size,1 but chest x-rays are inadequate for excluding the presence of aortic dissection and screening for chest trauma.23 Considering the advantages of universal availability, rapid acquisition, and high resolution of computed tomography (CT), CT has thus far played a central role in the diagnosis, risk stratification, and management of aortic disease, particularly in emergency settings.4 In contrast to CT, which lacks the ability to show crucial differences in physiology, nuclear medicine imaging has the advantages of providing molecular and functional information. In recent years, as technology has developed, combined Positron Emission Tomography/Computed Tomography (PET/CT) has been adopted for offering both the high resolution of CT and the ability of PET to show the molecular aspect; thus, integrated PET/CT images can simultaneously reveal anatomical, molecular, and functional information. Consequently, PET/CT improves the diagnostic accuracy and localization of many lesions.5 Since South Korea began reimbursement via a public insurance system in June 2006,6 the number of PET studies has greatly increased. Moreover, as the market for PET/CT devices increases, the clinical application of PET/CT is expanding beyond malignant diseases. South Korea has adopted broad 18F-fluorodeoxyglucose (FDG) PET/CT indications, including assessment of malignancy, ischemic heart disease, partial-onset seizure, and other diseases that may benefit from its use. Europe and the United States have also accepted a relatively broad spectrum of indications. Therefore, there is an increasing trend in the use of FDG PET/CT for diseases other than malignancy.
This article provides an overview of recent PET/CT studies in the field of aortic disease. Seeing as PET/CT imaging has been applied in a wide range of clinical settings, its use has increased in the evaluation of diseases involving the aorta and arteries. Although the usefulness of PET/CT has not been established in the field of aortic disease, we summarize previous studies on PET/CT, and address its potential role in diseases involving the aorta and arteries, including the acute thoracic aortic syndromes, aortic aneurysm, atherosclerotic lesions, aortitis and aortic tumors.
ACUTE THORACIC AORTIC SYNDROMES
Acute thoracic aortic syndromes encompass a spectrum of emergency conditions, including aortic dissection, intramural hematomas and penetrating atherosclerotic ulcers. They are life-threatening conditions that require prompt diagnosis. CT is the imaging modality of choice for suspected dissection and in general in cases of acute aortic syndromes,78 and emergent operations are performed according to CT images. In contrast to CT, the major drawback of FDG PET/CT is its prolonged scan time. The acquisition of PET/CT starts 60 minutes after FDG administration, not immediately, however, the interval between FDG administration and the start of acquisition can be shortened to some extent.9 Nevertheless, in an emergency, it is unethical to delay surgery for FDG PET/CT diagnosis, and it is thus prohibited. Obviously, FDG PET/CT is not included in recent guidelines regarding acute aortic syndromes.78 Therefore, most previous studies have retrospectively reviewed images in cases of aortic dissection or in cases where an emergent operation could not be performed because of the greater severity of the patient's accompanying disease. Considering the disadvantages of a prolonged scan time, which obviates its applicability in acute settings, FDG PET/CT studies are relatively few in number. Very few studies have been conducted on cases of Stanford type A aortic dissection that need emergent surgical repair.10
FDG PET/CT may help to discriminate acute from chronic aortic dissection.11 Acute dissection of the aortic wall leads to elevated metabolic activity at the site of fresh laceration of the aortic wall, and acute vascular injury may induce repair mechanisms leading to accumulation of glycolytic active cells, such as macrophages and activated myofibrinocytes in the vessel wall, thus enhancing FDG uptake. Reeps et al.11 suggested that FDG PET/CT can be helpful in the diagnosis of asymptomatic acute dissection, which results in severe complications. The standardized uptake value (SUV) ratio and SUVmax can overcome the low specificity of electrocardiograms and laboratory parameters such as fibrinogen and D-dimers, to exclude acute dissection. Furthermore, FDG PET/CT imaging may be helpful in identifying patients with acute aortic syndromes with an increased risk of disease progression. Kuehl et al.12 reported vessel wall inflammation in one-third of examined patients with acute aortic syndromes, and this patient group seemed to have a high risk for disease progression. A case study that reviewed data from serial cancer-screening PET/CT obtained 5 years prior to acute aortic events revealed a trend of gradually increasing aortic FDG activity when the dissection was imminent.13 Kato et al.10 showed that SUVmax and SUVmean were significantly greater for the unfavorable outcome group than for the favorable outcome group. A mean SUV greater than 3.029 demonstrated significantly greater predictive power for acute aortic dissection, and greater FDG uptake in the dissected aortic wall was significantly associated with an increased risk for rupture and progression of aortic dissection. Unlike CT scans, follow-ups with serial FDG PET/CT may be able to detect pathologic changes in the dissected aorta and to clarify the pathologic mechanism of the disappearance or regression of acute aortic dissection.1014 However, the revised 2014 ACR Appropriateness Criteria15 rated FDG PET/CT scans with a score of 3 for acute chest pain - suspected aortic dissection, which typically indicates an inappropriate modality.15 Nevertheless, FDG PET/CT may play a role in prognosticating the outcome in individuals diagnosed with aortic dissection and further investigation is warranted.
Intramural hematomas and penetrating atherosclerotic ulcers are components of acute aortic syndromes. A few PET/CT case reports have been published on intramural hematoma, acute intramural hematoma of the aorta with positive FDG uptake,16 acute intramural hematoma of the ascending aorta,17 intramural hematoma at a pulmonary artery bifurcation site and the ascending aorta,18 and intramural hematomas with penetrating ulcer and saccular pseudoaneurysm in the abdominal aorta.19 These cases exhibited significant FDG uptake with an SUV of 4.4 to 10 in the lesions. In accordance with intramural hematomas, penetrating aortic ulcers exhibited increased glucose metabolism within the penetrating ulcer.20 Patients with penetrating aortic ulcers who exhibited greater FDG uptake in the aortic wall were more likely to develop adverse aortic events, and a target-to-background ratio of 1.5 had an acceptable predictive value for differentiating high-risk from low-risk patients.21 Gorla et al.22 demonstrated that pathological glucose uptake in aortic wall lesions determined using FDG PET/CT was associated with high C-reactive protein (CRP) levels, increased mortality, and more major adverse events at 3-year follow-ups in acute aortic syndromes including penetrating aortic ulcers.
In summary, FDG PET/CT for acute aortic syndrome plays a potential role in diagnosis and risk stratification, discrimination of acute from chronic dissection, prediction of development of aortic dissection, and prediction of unfavorable outcomes including rupture and progression.
AORTIC ANEURYSM
Aortic aneurysm is an enlargement of the aorta of up to 1.5 times the normal size. Aortic aneurysms cause weakness in the wall of the aorta and increase the risk of aortic rupture. Studies conducted before 2010 reported many cases with FDG uptake in the aortic aneurysm wall;2324 hence, FDG PET/CT was introduced as a new diagnostic technique to study aortic aneurysm disease in vivo.25 Sakalihasan et al.23 reported several cases that required emergent or urgent aneurysmectomy for ruptured, leaking, rapidly expanding, or painful aneurysms with FDG uptake. In a surveillance study of small aortic aneurysms,26 the majority of non-specific aortic aneurysm patients exhibited increased FDG uptake with a SUVmax of over 2.5. Histologic study showed that increased FDG uptake in the aortic aneurysm wall was correlated with higher densities of inflammatory infiltrates and macrophage, T-cell infiltrations, and lower collagen fiber content and vascular smooth muscle cell density.25 Thus, FDG PET/CT may contribute to improved prediction of aneurysmal rupture risk. Another study also demonstrated that FDG uptake in the aortic aneurysmal wall displayed alterations potentially related to medial degeneration and considerable degradation of the fibrillary structures of the adventitia.27 They showed that the FDG uptake is related to the massive infiltration of activated lymphocytes and macrophages in the aneurysmal wall, inducing profound remodeling. In addition, FDG activity was commonly focused in the shoulder region of the aneurysmal wall, which is possibly related to a destructive macrophage phenotype; accordingly, it is considered to provide information different from that obtained from an MRI.28 Furthermore, high stress to aortic aneurysm wall may also be linked with high levels of FDG uptake.29
However, studies conducted after 2010 have also addressed aortic aneurysm in asymptomatic patients, and they have consistently shown that FDG uptake in aortic aneurysm is not a common finding. Tegler et al.30 reported no significantly increased FDG uptake in asymptomatic aneurysmal patients compared with healthy controls, although histologic examination of the aneurysm walls showed high inflammatory cell infiltration by T lymphocytes, B lymphocytes, and macrophages. Palombo et al.31 assessed the prevalence of increased FDG uptake in aneurysmal walls in asymptomatic patients with aortic aneurysms, and found that increased FDG uptake was extremely rare in patients with aortic aneurysms with a diameter close to the indication for surgery. Severe loss of wall structure and a low number of cells may explain the lack of visible FDG uptake in asymptomatic patients with aortic aneurysms, the diameter of which is close to the indication for surgery.32 Another longitudinal PET/CT study, in line with recent studies, showed that aortic aneurysms with lower FDG uptake may be more likely to expand.33 Barwick et al.34 also demonstrated no correlation between aneurysmal size and metabolic activity in a relatively large series with an unselected and well-matched control group. Previous histologically validated studies have shown that increased FDG uptake on PET/CT predicts the degree of wall inflammation,232526 but currently increasing studies are reporting that FDG uptake varies widely in the process of aneurysmal expansion and the results for FDG uptake as a predictor of clinical outcomes such as expansion or rupture are inconsistent.
Thus, because of the inconsistent results regarding FDG PET/CT, preclinical and clinical studies using various radiopharmaceuticals that can target different disease processes are currently underway to monitor the biological activity of aortic aneurysms. 68Ga-DOTATATE,35 11C-PK11195,36 18F-cross-linked iron oxide nanoparticle37 and 18F-choline383940 can target macrophages, while 18F-fluciclatide,41 18F-FPPRGD42 and 64Cu-NOTA-TRC105-Fab43 can be used for neovascularization and angiogenesis in the process of aortic aneurysms. Another radiopharmaceutical targeting microcalcification,44 18F-Sodium fluoride (NaF), has critical clinical application in aortic aneurysms. The Sodium Fluoride Imaging of Abdominal Aortic Aneurysms (SoFIA) study demonstrated both that NaF uptake identifies advanced aneurysmal disease and its association with aneurysm growth and clinical events.45 Many radiopharmaceuticals are being developed to target the various pathogenic mechanisms of aortic aneurysm progress; therefore, it is expected that PET/CT using various tracers will offer a clearer understanding of aortic aneurysms.
In summary, FDG PET/CT of aortic aneurysms has the potential to predict expansion and progress in symptomatic patients, but FDG uptake varies widely in asymptomatic patients. PET/CT using new radiopharmaceuticals related to pathogenic processes will shed new light on aortic aneurysms and the additional clinical studies will strengthen the role of PET/CT for aortic aneurysms.
ATHEROSCLEROTIC LESIONS
Atherosclerosis is a disease of the arterial wall, whereby endothelial cell damage results in the accumulation of lipids and inflammatory cells within discrete areas of the intima, eventually encroaching upon the vessel lumen.46 FDG is the most common PET tracer in atherosclerosis PET/CT imaging. A study conducted by Rudd et al.47 revealed increased FDG uptake in symptomatic carotid plaques ipsilateral to a recent stroke, marking the first human study in which atherosclerotic plaque inflammation was imaged with FDG PET. Increasing evidence has since been obtained that there is increasing evidence that FDG PET/CT can be used as a marker of plaque vulnerability to identify patients at high risk of clinical events,484950 and as a surrogate end point in clinical trials of antiatherosclerotic therapies.515253
Vascular FDG uptake mainly indicates increased macrophage activity resulting in inflammation within atherosclerotic plaques, whereas NaF is a marker of increased vascular calcification resulting in microcalcification in the vasculature. Irkle et al.44 demonstrated that NaF binds preferentially to regions of developing microcalcification in carotid atheroma, with little or no binding to non-calcific tissue types. A recent prospective study also demonstrated the ability of NaF PET to predict progression in the CT calcium score over 1 year.54 Many studies have introduced various radiopharmaceuticals targeting pathologic processes in the imaging of the vascular cell adhesion molecule (VCAM)55 of the endothelium, choline metabolism,3856 translocator protein (TSPO),3657 somatostatin receptor5859 of macrophages, monocytes and macrophages released proteases including matrix metalloproteinase (MMP) and cathepsin,6061 hypoxia62 and neoangiogenesis.636465 Based on these preclinical studies, more active clinical studies may lead to favorable results in atherosclerotic lesions.
In summary, FDG PET/CT imaging of atherosclerosis allows for the in vivo visualization of vascular inflammation, which can help evaluate plaque vulnerability and predict clinical events. Novel PET tracers, which are designed to track active calcification, inflammation, hypoxia or neoangiogenesis, may be potential markers for plaque rupture and cardiovascular risk.
AORTITIS
Aortitis is the pathological term for the inflammation of the aortic wall.66 The classification of aortitis broadly includes noninfectious and infectious aortitis. Noninfectious aortitis can be classified into large-, medium-, and small-sized vessel vasculitides. Infectious aortitis is induced by microorganisms such as tuberculosis, syphilis, salmonella or other bacteria. Aortitis may also result from idiopathic conditions or radiation.
PET/CT has the disadvantage of limited spatial resolution, and most PET/CT studies have focused on the visualized inflammation of the aorta and the larger arteries. Large-vessel vasculitides such as Takayasu arteritis and giant cell arteritis are the most common causes of aortitis.66 Takayasu arteritis frequently involves the aorta, and its major branches. Although FDG PET/CT is not a component of the criteria of American College of Rheumatology,67 FDG PET/CT may play a role in diagnosis, differential diagnosis, the exclusion of other causes of arteritis, and the identification of optimal target sites for biopsy.686970 FDG PET/CT allows differentiation between active and inactive Takayasu arteritis, because conventional inflammatory markers such as a high erythrocyte sedimentation rate (ESR) and CRP which reflect systemic inflammation, are nonspecific for Takayasu arteritis, and immunomodulatory agents can modify these parameters.71 Furthermore, SUVmax clearly represents therapeutic effectiveness (Fig. 1); hence, FDG PET/CT is recommended for the diagnosis of Takayasu arteritis and detection of its recurrence. An Indian study reported that FDG PET/CT showed high sensitivity for detecting active diseases during immunosuppression and may help in guiding therapy and in assessing the response to immunosuppression.72 Seeing as metabolic changes precede anatomical changes, FDG PET/CT may also be useful in cases in which they are difficult to detect using CT or MRI.73
In giant cell arteritis, FDG PET/CT has been shown to be sensitive to extracranial vasculitis, but not for intracranial vasculitis because of its poor spatial resolution.74 However, extracranial involvement is common in 30% to 74% of giant cell arteritis,75 and therefore, FDG PET/CT may be helpful in localization of the extent of large-, and medium-sized vasculitis involving the aorta, and subclavian, carotid, and iliac arteries7677 as well as small-diameter extracranial involvement such as the temporal, occipital and vertebral arteries.78 Giant cell arteritis is often associated with polymyalgia rheumatica, which is an inflammatory disease around the joints;7980 accordingly, FDG PET/CT can also be useful in the diagnosis of polymyalgia rheumatica by visualizing the affected joints.77 Moreover, although temporal artery biopsy is considered the cornerstone of the diagnosis of giant cell arteritis, false negatives can represent up to 15%–70% of cases, resulting in delayed diagnosis.8182 Negative temporal artery biopsy cannot exclude the presence of giant cell arteritis; FDG PET/CT, therefore, can be considered when giant cell arteritis is clinically suspected. This is because FDG PET/CT is able to detect early inflammation without late effects such as an arterial halo on ultrasonography and aortic wall thickening or edema on MRI.83 In addition, because giant cell arteritis with increased FDG uptake in the aorta may be more prone to thoracic aortic dilatation, FDG PET/CT can be helpful to predict individual prognoses. In chronic periaortitis, FDG PET/CT is useful to evaluate disease activity,84 and has been successfully applied after immunotherapy when residual retroperitoneal tissue persists.85 FDG PET/CT also facilitates the detection of remote disease such as that seen in multifocal fibrosclerosis, occult neoplasm, or infectious processes with which retroperitoneal fibrosis may be secondarily associated.84
In contrast to large-vessel vasculitis, vasculitis of medium and small vessels has been less thoroughly studied. However, studies have reported that FDG uptake may be possible if smaller arteries are involved,76 depending on the spatial resolution of the PET/CT camera. Several studies have reported FDG uptake in diseases involving smaller arteries such as polyarteritis nodosa,7686 Wegener's granulomatosis,87 Churg-Strauss syndrome,88 or relapsing polychondritis.899091 Furthermore, FDG PET/CT may be able to differentiate between giant cell arteritis, Takayasu arteritis, and polyarteritis nodosa.76
FDG PET/CT has also proven its usefulness in infectious aortitis. Several case reports have been published on infected aortic aneurysms resulting from Staphylococcus aureus92 or Salmonella enteritides.93 The site of FDG uptake within the aneurysm wall corresponds with that of indium-111 white blood cell accumulation.92 FDG PET/CT provides not only accurate information for the diagnosis of infected aortic aneurysm, but also monitors the response to antibiotic therapy.93 Murakami et al.94 demonstrated that infected aortic aneurysms, can be discriminated from infection-free cases based on an SUVmax of 4.46; therefore, FDG PET/CT is useful for the diagnosis of an infected aneurysm (Fig. 2) and determination of the effects of postoperative antibiotic therapy and completion of therapy.
In summary, FDG PET/CT is useful in noninfectious aortitis involving medium-, small-, and large-vessels. It aids in diagnosis, differential diagnosis, the exclusion of other causes of aortitis, and the identification of target sites for biopsy. Moreover, it is helpful for evaluating disease extent and activity, predicting of prognosis, monitoring the response to therapy, and evaluating therapeutic effectiveness.
AORTIC TUMOR
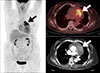
Primary malignant tumors of the aorta are extremely rare,95 and exhibit heterogeneous histopathology. Sarcomas of the intima are the most common, followed by leiosarcomas and fibrosarcomas of the media or adventitia of the aortic wall. FDG PET/CT is a useful modality for detecting malignant tumors including sarcomas of the aorta (Fig. 3).969798 In patients with peripheral or splanchnic emboli, an aortic sarcoma should be included in differential diagnosis; therefore, a whole-body PET/CT scan can be used for comprehensive staging.99 In one study of primary sarcomas of the aorta and arteries,100 FDG PET/CT showed high metabolic activity in sarcomas, local embolic spread in the pulmonary vasculature of the lungs, distant metastases to the brain, and high metabolic activity at the site of vascular filling defects, which strengthens the suspicion of malignant disease.
In summary, FDG PET/CT is useful for the evaluation of primary malignancy of the aorta, embolic spread, distant metastasis, and extension into adjacent arteries.
ETHICAL STATEMENT
No research interventions were done in this review (no ethical approval or informed consent needed).
CONCLUSION
PET/CT gives useful information for the physiological, molecular, and functional aspects of aortic diseases, providing a pathophysiologic understating of acute thoracic aortic syndromes, aortic aneurysm, atherosclerotic lesions, aortitis, and aortic tumors. Patients who need diagnosis, assessment of disease extent and metabolic activity, prediction of clinical outcome, or evaluation of therapeutic effectiveness for the aortic disease could benefit from FDG PET/CT. Future studies are needed to confirm the clinical usefulness of FDG PET/CT in large patient populations and PET/CT with developing new radiopharmaceuticals should be validated for potential clinical applications in regards to the various aortic diseases.


 XML Download
XML Download