

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Clavicle fractures are common injuries in adults, accounting for 5% of all fractures and 44% of all shoulder fractures.1-3) Clavicle midshaft fractures have been usually treated with conservative measures.4,5) However, the operative treatment of displaced, comminuted fractures resulting from high energy injuries, such as motor vehicle accidents, industrial accidents and sporting injuries, is used to prevent shortening or angular deformities that can cause constant pain, and the importance of obtaining functional satisfaction with early exercise has been emphasized.6,7) There are various methods for treating clavicle midshaft fractures, such as intramedullary K-wires or Steinmann pins fixation and plate fixation.8-11) In particular, plate fixation can help obtain firm anatomical reduction in severe displaced or comminuted fracture. There are various plates including Sherman plates, dynamic compression plates and semitubular plates. Among them, a reconstruction plate and reconstruction locking compression plate (LCP), which can be bent to the S-shaped curvature of the clavicle, are the most preferred. This study examined the clinical and radiological outcomes between the reconstruction plate and reconstruction LCP for clavicle midshaft fractures along with its efficacy.
METHODS
Materials
Between June 2000 and May 2008, 69 cases of an open reduction and internal fixation with a plate were performed for clavicle midshaft fractures. Of them, 41 patients, who could have been followed until bony union was achieved, were reviewed retrospectively. Reconstruction plates and reconstruction LCPs were used in 19 and 22 cases, respectively. The operative indications were fractures involving ≥ 20 mm displacement or shortening, comminuted fractures, fractures with suspected soft tissue interposition that could not be reduced by a closed reduction, open fractures, multiple fractures and fractures with a neurovascular injury. A decision on plate selection was not affected by the indications.
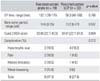
In the reconstruction plate group, the mean follow-up period was 13.2 months (range, 7 to 35 months). There were 12 males and 7 females with a mean age of 45.0 years (range, 22 to 70 years). The cause of the injury was a traffic accident in 13 cases, slip down in 3 cases, a sports injury in 1 case, fall down in 1 case and miscellaneous in 1 case. Associated injuries were encountered in 15 cases: scapular fracture in 3 cases (floating shoulder was also noted in 2 of them), hemothorax and rib fracture in 2 cases, and acromioclavicular joint dislocation in 1 case.
According to Robinson's classification,12) there were 7 B1 type and 12 B2 type fractures. The mean interval from injury to operation was 14.4 days (range, 3 to 44 days). In the reconstruction LCP group, the mean follow-up period was 11.9 months (range, 7 to 24 months). There were 17 males and 5 females with an average age of 46.0 years (range, 19 to 69 years). The cause of the injury was a traffic accident in 17 cases, slip down in 3 cases, fall down in 1 case and miscellaneous in 1 case. An associated injury was found in 16 cases: hemothorax and rib fracture in 5 cases, scapular fracture in 3 cases (floating shoulder was observed in 2 of them), and rotator cuff tear in 1 case. There were 9 B1 type and 13 B2 type fractures. The mean interval from injury to surgery was 9.0 days (range, 1 to 29 days) (Table 1).
Operative Technique and Rehabilitation
A transverse skin incision was made along the superior border of the clavicle under general anesthesia. Fixation was performed following a reduction with minimal periosteal stripping. Each plate was contoured to the shape of the clavicle. In the reconstruction LCP group, plate contouring was performed with the locking sleeves inserted into the plate holes to prevent deformation of the holes. To obtain maximum fixation strength, ≥ 3 screws were used in the proximal and distal areas, respectively. If necessary, a circlage wire and lag screw were used in cases where fracture reduction could not be achieved due to a severe comminuted fracture with ≥ 2-3 bone fragments. In cases where severe comminution was observed in the inferior surface of the clavicle, autogenous iliac bone grafting was also performed to avoid nonunion or fixation failure or metal breakage caused by tension. Bone grafting was performed in 8 cases in the reconstruction plate group and in 7 cases in the reconstruction LCP group. An arm sling was used for approximately 2 weeks after surgery, and pendulum exercise and active range of motion exercise were then started.
Assessment of Treatment Outcomes
For a radiological assessment, the bone union period was compared using radiographic evidence, such as callus formation and trabecular bridging across the fracture site. For the clinical assessment, the Quick Disability of the Arm, Shoulder, and Hand (DASH) scores13) suggested by the American Academy of Orthopedic Surgeons (AAOS) were evaluated using a patient interview and telephone survey. Statistical analysis was performed using SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA). An independent t-test and chi-square test were used. A p-value < 0.05 was considered significant.
RESULTS
The patients' age, gender, cause of injury, fracture pattern, interval from injury to operation and autogenous bone grafting were no statistically significant difference in the two groups (p > 0.05). The mean operative time was 102.1 minutes (range, 70 to 175 minutes) in the reconstruction group and 99.3 minutes (range, 40 to 180 minutes) in the reconstruction LCP group, showing no notable intergroup differences (p > 0.05).
Bony union was achieved in all cases after surgery at an average of 14.6 weeks (range, 8 to 35 weeks) and 13.2 weeks (range, 8 to 27 weeks) in the reconstruction and reconstruction LCP group, respectively, indicating no significant intergroup difference (p > 0.05). In the clinical assessment, the reconstruction group and reconstruction LCP group showed a mean score of 33.85 (range, 22.7 to 40.9 points) and 34.81 points (range, 22.7 to 81.8 points), respectively (p > 0.05).
Postoperative complications were noted in both groups. In the reconstruction group, there was hypertrophic scarring without pain in 2 cases (10.5%), limited shoulder motion in 2 cases (10.5%), painful shoulder in 2 cases (10.5%), and screw loosening causing neither pain nor functional disability in 3 cases (15.8%) (Fig. 1). In the re construction LCP group, hypertrophic scarring was observed in 4 cases (18.2%), limited shoulder motion in 1 case (4.6%) and painful shoulder in 1 case (4.6%), but neither screw loosening nor plate failure were observed (Fig. 2). Infection and nonunion was not observed in either group (Table 2) (p > 0.05).
DISCUSSION
Most clavicle midshaft fractures are treated conservatively. In 1960, Neer14) reported that nonunion occurred only in 3 of the 2,235 patients in whom clavicle midshaft fractures had been treated non-surgically. In 1968, Rowe15) reported that nonoperative treatments resulted in nonunion in only 4 out of 566 clavicle midshaft fracture cases, and the surgically treated patients presented with more postoperative complications and nonunion. Accordingly, nonoperative treatments have been preferred by many surgeons. However, according to Zlowodzki et al.,16) nonunion occurred after nonoperative treatments in 6% of 1,145 clavicle midshaft fracture cases and the percentage increased to 15-20% particularly in the 159 fracture cases with severe displacement. While only 2% nonunion was noted in the surgically treated cases. In addition, the extent of fragment displacement is closely associated with fracture union12,17) and anatomical restoration of the displacement is considered essential for rapid recovery. Hence, there has been increasing interest in surgical treatments with open reduction and internal fixation. In particular, operative treatments are performed more often for the treatment of clavicle midshaft fractures due to the increasing instances of severely displaced and comminuted fractures caused by high energy injuries in motor vehicle accidents, industrial accidents and sport injuries.6,7) Shen et al.11) obtained satisfactory outcomes in 94% of the 232 cases by open reduction and plate fixation. In 2007, the Canadian Orthopaedic Trauma Society reported that internal fixation with plates resulted in more rapid union, excellent clinical outcomes, and lower complication rates in 132 patients with displaced clavicle fractures than nonoperative treatments.18)
The operative methods for the treatment of clavicle midshaft fractures involve intramedullary K-wire fixation or Steinmann pin fixation and plate fixation. The procedures using the former two materials result in low resistance to torque, carry risks of pin loosening and infection, and require a long-term fixation period.19,20) Open reduction and internal fixation with plates, such as Sherman plates, dynamic compression plates, and semitubular plates, can be effective in obtaining anatomical reduction, applying direct compression to the fracture site, and producing resistance to torque. However, it is disadvantageous in achieving firm fixation because it is difficult to hold the plates to the clavicle in severely comminuted fracture cases.21)
In contrast, reconstruction plates can be manipulated to fit the contour of the clavicle and fracture pattern to obtain firm fixation, are lighter and thinner than dynamic compression plates and are durable to multidirectional mechanical stress imposed on the fracture site.11,22) On the other hand, penetration of the opposite cortical bone for screw fixation may cause damage to the subclavian artery and firm fixation can be difficult to maintain in osteoporotic patients over 50 years of age.23,24) In this study, the use of reconstruction plates did not result in complications, such as subclavian artery in juries and brachial plexus injuries, but 3 cases of screw loosening occurred during the follow-up period. Although nonunion, pain, or functional disabilities were not observed in these cases, it is believed that reconstruction LCPs could be used as an alterative to reconstruction plates to reduce the number of complications.
The advantages of reconstruction LCPs include strong fixation due to locking between the screw and plate, and blood supply preservation due to minimal contact between plate and cortical bone.25,26) With conventional screws and plates, fracture site stability is provided by friction between the plate and bone cortex. Accordingly, screws need to be fixed onto both cortexes. In contrast, when an LCP is used, an external force is transmitted from the cortical bone through the conically threaded plate hole to the plate because the screw head is locked firmly in the threaded plate hole. Therefore, the plate does not need to be compressed onto the cortical bone for stability, which results in good preservation of the blood supply, and the plate thread is also helpful in preventing screw loosening or instability.27,28) When LCPs are used to treat clavicle midshaft fractures, the risks of injury to the subclavicular artery or brachial plexus can be reduced because fixation can be achieved without the tip of the screw reaching the opposite bone cortex and periosteal stripping can be minimized to promote rapid union.27) It is believed that the surgery time can be reduced using LCPs because accurate plate contouring is not necessary and periosteal stripping could be minimized using self tapping screws. However, there were no significant differences between the reconstruction plate group and reconstruction LCP group in terms of the union period, surgical time, and Quick DASH score. Nevertheless, a reconstruction LCP can be an effective replacement for a reconstruction plate considering that complications, such as screw loosening and plate failure, were not observed in the reconstruction LCP group. Contour of the plates was performed with locking sleeves inserted into screw holes considering the problem of LCPs that screw fixation can be weakened if breakage of the screw holes occurs in the plate thread during plate contouring.
Unfortunately, surgical treatments for clavicle fractures leave distinct scars on the shoulder. Ali Khan and Lucas29) suggested in 1978 that patients with clavicle midshaft fractures could suffer from hypertrophic scarring after surgical treatments with plates. Surgical scars are currently considered major complications due to the increasing demand for aesthetics. Six of our patients had hypertrophic scarring after surgery and complained of discomfort in carrying out their daily activities. However, none of them had associated pain or requested cosmetic surgery. However, the patients should be informed of the possible appearance of surgical scars preoperatively and surgical techniques should be improved to address the problem.
This study had some limitations. The conclusions drawn from this analysis cannot be generalized because of the small number of cases and that the study design was retrospective. Therefore, the efficacy of a reconstruction plate and reconstruction LCP for the treatment of midshaft clavicle fractures should be tested in prospective studies involving a larger number of cases.
In conclusion, bony union could be achieved in both the reconstruction and reconstruction LCP groups and the clinical outcomes were satisfactory. Overall, operative procedures using reconstruction plate or reconstruction LCP, which can be shaped to match the contour of the clavicle, can be effective in the treatment of clavicle midshaft fractures.



 XML Download
XML Download