

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anti-estrogen hormone therapy is a major treatment modality in breast cancer, and long-term results from randomized clinical trials have indicated its efficacy in reducing mortality rates of estrogen receptor-positive and progesterone receptor-positive breast cancer [1234]. Oral anti-estrogen agents are generally prescribed for 5 years, and have been used as the first-line adjuvant treatment for early hormone receptor-positive breast cancer. Although numerous resources and consistent efforts have been applied towards novel drug discovery, there has been no paradigm shift in the hormonal treatment of hormone receptor-positive breast cancer. Moreover, several studies have validated the benefits of extended hormonal treatment (for > 5 years) [356], and the number of recipients of long-term oral hormonal treatment has been increasing.
Adverse events due to hormonal treatment, such as hot flashes, arthralgia, or mood changes, increase the difficulty of medication adherence [78910]. The socio-economic status of patients, including personal plans for marriage or childbirth, can also affect treatment compliance [1112131415]. As adherence to hormonal treatment correlates strongly with breast cancer prognosis [816171819], treatment non-adherence, assessed by various methods, has been an important subject of previous research.
Though several studies have assessed the relationship between treatment discontinuation and breast cancer prognosis [1920], there is a difference in the observations between controlled studies and actual clinical situations “Hawthorne effect”. Moreover, there may be a loss of information when estimating adherence based on claims data obtained from patients [21]. Nevertheless, data on patient visits and drug prescriptions being accumulated in electronic medical records (EMRs) closely mirror actual clinical data, and can thus facilitate compliance assessment. In particular, the prescription refill gap—an indicator of medication adherence—can be measured concurrently, as prescription data are accumulated [22].
In the present study, we aimed to examine differences in clinical outcomes according to the hormone prescription gap in breast cancer patients. To evaluate patient risk as a result of the gap in medication, we assessed prescription data extracted from EMRs in relation to outcomes in a breast cancer patient series. Moreover, we determined the suitability of using the prescription refill gap as an indicator of hormonal treatment adherence.
METHODS
In this retrospective study, we investigated the association between the gap in hormone treatment and breast cancer outcomes using clinical data from the Asan Medical Center. All clinical data were anonymized for research purposes using a de-identified clinical data warehouse: Asan BiomedicaL research Environment [23]. We assessed adherence by analyzing the gap between successive prescription refill dispensation visits, compared to the interval between regular visits or when the patient visited the hospital after a greater delay than expected. We examined the effect of adherence within the conventional treatment period (4.5 years) on the prognosis of breast cancer after that period.
Study design and subjects
We enrolled patients with pathologically confirmed stage I–III breast cancer who underwent surgery at Asan Medical Center between January 1, 1997, and December 31, 2009. Follow-up data were collected up to May 31, 2015. Among the 10,426 breast cancer patients who underwent surgery at Asan Medical Center, we excluded those who met the following criteria: hormone receptor-negative cancer and/or no record of hormonal agent prescription and presence of early recurrence and/or early loss to follow-up (within 4.5 years [54 months] after surgery). Figure 1 details the patient selection process.
Figure 1
Flow diagram of patient selection; a total of 5,928 patients were enrolled in this study.
AMC = Asan Medical Center.

Prescription data (prescription visit date and prescription duration) for hormonal treatments, including first-line adjuvant anti-estrogen oral medications (i.e., tamoxifen citrate, toremifene citrate, letrozole, anastrozole, and exemestane), were analyzed for each patient. Patient demographic data, including the age at breast cancer diagnosis, marital status at diagnosis, type of residential area, education level, body mass index, and family history of breast cancer, were additionally collected. Further, information on breast cancer stage, histologic type, histologic grade, operation methods, and adjuvant treatment (i.e., chemotherapy and/or radiation therapy) were included.
Determining the duration of the prescription refill gap
The number of days of treatment omission was estimated by subtracting the duration of medication coverage from the intervals between prescription dates. Prescription refill gaps (hereafter referred to as gaps) were recorded when the gap duration was > 4 weeks (28 days). The interval between routine follow-up and a prescription visit was 6 months, and the last visit (without prescription) was not included in the prescription data. Therefore, the total prescription period analyzed was 4.5 years (54 months), starting from the first prescription date; no cases of treatment extensions were considered. The gap was calculated up to 4.5 years after surgery (the duration of prescription completion). If the medication was discontinued within 4.5 years, the gap was estimated as the duration from the expected date of medication depletion to the date of prescription completion. The gap ranged from 29 to 1,641 days (median gap: 92 days).
Outcome variables
We assessed the follow-up results for up to 10 years (120 months) from the date of prescription completion. As per a regular follow-up schedule, the last prescription visit was made 4.5 years after the first visit in the planned 5-year treatment regimen. Cancer-related outcome after treatment completion was evaluated after excluding cases of recurrence or death during the 4.5-year treatment period. The outcome parameters included breast cancer recurrence (of any type), distant metastasis, breast cancer-specific death, and overall death, which occurred after the 4.5-year treatment period.
Statistical analysis
All reported p values are 2-sided, and p-values < 0.05 were considered significant. Statistical analysis was performed using SPSS statistics version 21 (IBM Corp., Armonk, USA) and R version 3.2 (R Development Core Team, Vienna, Austria). Differences between groups were examined using the χ2 test for categorical variables. Survival curves were constructed using Kaplan-Meier estimates, and curves were compared using the log-rank test. To determine the accumulated effect of gaps, we sub-classified the patients with gaps according to the summation of the gap (gap sum). The gap-positive group was further divided into 4 subgroups based on quartiles: from 1st quartile (patients with low gap sum) to 4th quartile (patients with high gap sum). The range of the gap sum was 29–1,625 days, and the cut-off between successive quartiles was 64, 160, and 391 days. Analysis using multivariate Cox proportional hazards regression model was performed according to the gap sum quartile. The relative risk of breast cancer outcomes was assessed to determine the linear tendency of increasing risk as the cumulated gap increased.
Ethics
This study was approved by the Institutional Review Board (IRB) of Asan Medical Center, Korea (IRB No. 2015-0924). The need for informed consent was waived by our Institutional Review Board, as this study involved routinely collected medical data that were anonymously managed at all stages, including during data cleaning and statistical analysis.
RESULTS
Patient characteristics
A total of 5,928 patients with no breast cancer recurrence within 4.5 years from the date of breast cancer surgery, were enrolled in the present study. Among these cases, 2,821 (47.6%) had a gap of > 4 weeks. The baseline demographic and clinical characteristics of patients with and without gaps are presented in Table 1. Patients who were younger (p < 0.001), had a non-married status at diagnosis (p < 0.001), had stage II breast cancer (p = 0.013), underwent mastectomy (p < 0.001), or did not undergo chemotherapy (p = 0.013) and/or radiation therapy (p < 0.001), were significantly more likely to have a gap. Patients with invasive lobular carcinoma tended to have a greater gap than patients with invasive ductal carcinoma, although this difference was not significant (p = 0.078).
Table 1
Baseline characteristics of the enrolled patients, according to the presence of a gap

Prognostic and survival effect of the gap
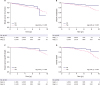
Patients were followed up to 10 years from the completion of hormone treatment, and breast cancer recurrence (of any type) was observed in 318 patients in this period. Distant metastasis was noted in 214 patients and 116 breast cancer-related mortalities occurred. As shown in Figure 2, the presence or absence of the gap was found to be significantly linked to survival outcome in all breast cancer types. In patients with distant metastases, the survival estimate was 95% in patients without a gap, and 85% in patients with a gap (log rank, p < 0.001; Figure 2B).
Accumulated prognostic effect of the gap
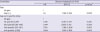
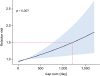
Multivariate Cox analysis indicated that the hazard ratio (HR) of distant metastasis was independently greater in patients with a gap (HR, 1.6; 95% confidence interval [CI], 1.182–2.166), as compared to patients without a gap, after adjusting for age at diagnosis, breast cancer stage, chemotherapy, and radiation therapy. The risk of distant metastasis increased with an increase in the gap sum, although the increase was not significant in the first and second gap sum quartile groups (p = 0.250 and p = 0.200, respectively). However, in the third and fourth gap sum quartile groups, the risk of distant metastasis was significantly high (HR, 1.758; 95% CI, 1.186–2.606 and HR, 1.844; 95% CI, 1.262–2.693; Table 2). The risk of distant metastasis constantly increased as the gap sum increased, and patients with a gap sum of approximately 3 years appeared to have a 50% greater risk of distant metastasis than those with lower gap sum values (Figure 3).
Table 2
Multivariate Cox regression analysis of the outcomes of breast cancer and covariates
DISCUSSION
In the present study, we assessed the prognostic significance of prescription gap and accumulated gap during hormonal treatment in a breast cancer cohort. Our findings indicate a negative effect of treatment omission on breast cancer prognosis, in agreement with previous studies that have correlated treatment adherence to better prognosis in breast cancer patients [8161718242526]. There are 2 important aspects of our study methodology which increase study reliability. Firstly, we used the prescription refill gap, including the non-intended gap between visit intervals, as an indicator of adherence. The index for measuring medication adherence, such as medication possession ratio (MPR) (used in prior studies), can only indicate the ratio within a specific period after completing treatment. In contrast, the gap and gap sum values are more realistic and are immediate indicators of medication administration, as they can be measured using real-world data from EMRs. Secondly, we assessed the long-term follow up results—i.e., up to 10 years following treatment completion, or up to 14.5 years from treatment initiation. Hence, we excluded patients with early loss to follow-up and/or early recurrence of breast cancer, and thus, the prognostic significance of the period without hormonal treatment coverage was presented more precisely. The prognostic value of disease characteristics (i.e., tumor size, grade, and node status) for early recurrence was thus minimized [27].
Hershman et al. [16] reported that an MPR of < 80% correlates with poor outcomes in breast cancer, and many other studies have defined poor adherence as an MPR < 80% [162028]. Nevertheless, the gap may serve as a more prompt indicator for discrimination between groups with different breast cancer outcomes. We observed here that the difference in disease prognosis could be caused by the accumulation of non-intended treatment blanks. Our findings can be applied in the clinics to stratify patients according to days of treatment omission, and caution them about the risks of skipping or discontinuing medication,
The differences between study groups classified on the basis of a gap period cut-off of 4 weeks were significant in terms of age, marital status, breast cancer stage, breast surgery methods, chemotherapy, and radiation therapy. Unmarried women tended to have a greater gap, which suggests that concerns regarding marriage and childbirth can affect compliance. However, as marital status was associated with the age at diagnosis (multicollinearity test, t = 16.90; p < 0.001), we could not determine whether the origin of this association was marriage itself. A younger age at diagnosis was also found to correlate with the presence of a gap, which implies that the increased risk associated with younger age in breast cancer may be caused by poor adherence to hormonal treatment [29].
We further found from our present analysis that the breast cancer stage significantly differed based on the presence of the gap, although there was no marked linear tendency for this association. Our results showed that patients who received breast conserving surgery were more likely to adhere to hormonal treatment than those who received mastectomy (Table 1), in contrast to previous findings [20]. Patients receiving radiation and/or chemotherapy should visit the hospital during the early period of adjuvant treatment, as they would have a greater opportunity to communicate with clinicians. Since the emotional support of clinicians has positive effects on medication adherence of hormonal treatment [1315], those patients would have higher chances of decreasing the gap. In patients who receive breast conserving surgery, the amount of remnant breast tissue and perceived risk of local recurrence can affect adherence. However, concerns regarding a bad prognosis should be evenly distributed as the gap does not only affect loco-regional recurrence but also distant metastasis.
Due to the limitation of the retrospective study, we did not investigate the actual cause of the treatment gap. In addition, there was no consideration of the cause of death associated with hormone therapy by analyzing overall death, and we could not determine from our present analyses whether skipping medication for 4 weeks would affect the clinical outcomes of breast cancer patients. The presence of < 3% treatment blank phases within the total treatment period is unlikely to be clinically relevant. Our current results are from a single center, and caution should be exercised about generalizing these findings, since the prescription pattern is unique to each medical center. Moreover, the issuing of a prescription does not always indicate an actual purchase or intake of medicine. Although these limitations should be considered, we contend from our present analysis that a gap of 4 weeks can be used as a validated surrogate index of adherence.
Hence, the gap can be used as a sentinel index for longer discontinuation and poor adherence. Moreover, the prescription gap is a convenient parameter that can be easily derived without the need for complicated equations, and ease of use implies that feedback can be given to patients at each visit. Patient education and communication is regarded as the main modifiable factor in improving adherence [730], and a more prompt response from clinicians may be a good solution to alleviating gap issues. Further studies involving breast cancer patients at other medical centers, or alternatively involving other medications or diseases, would be useful. In addition, further evaluation would help determine whether the gap can be used as a universal index for monitoring the effectiveness of oral medication.
 XML Download
XML Download