

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
BRCA1 and BRCA2 are tumor suppressor genes that are involved in multiple cellular processes, including DNA damage repair, cell cycle control, and transcription [12]. These processes perform universally essential functions in the homeostasis of all mammalian cells. However, the prevalence of BRCA1/2 (BRCA1 or BRCA2) mutation-related cancers is not similar across various organs [3]. Carriers of germline mutations of BRCA1 and BRCA2 are more likely to develop cancers of the breast and ovary, followed by those of the colon and prostate, with lesser incidence [4]. Breast and ovarian cancers are known to be regulated by sex hormones; thus, it is possible that BRCA1/2 may be important regulators of growth and differentiation in hormonally responsive epithelial cells.
BRCA1 can regulate the estrogen receptor (ER)-mediated downstream signaling by inhibiting transcriptional activators, such as activation function 2 (AF-2) [5] and p300 [6]. Further, mutations in the BRCA1 gene can lead to increased vascular endothelial growth factor secretion and breast epithelial proliferation, via direct interaction between BRCA1 and the ER protein [7].
As several studies have highlighted the potential interactions between the BRCA1/2 genes and the ER in developing breast cancers, we hypothesized that the reproductive histories of women who are BRCA1/2 mutation carriers can influence the clinical presentation of their breast cancer. To address this issue, we investigated the relationship between reproductive factors and the clinical characteristics of breast cancers in Korean women with germline mutations in BRCA1 and BRCA2.
METHODS
This study was conducted on women with either proven BRCA1/2 mutations, or both, who were recruited to the Korean Hereditary Breast Cancer (KOHBRA) study, from 2007 to 2014. The study design and eligibility criteria have been described in a previously published KOHBRA interim report [8]. All probands received genetic counseling, and the genetic testing for the BRCA mutations was performed after obtaining informed consent. For this study, genetic mutations were narrowly defined as protein-truncating and missense mutations. Unclassified variants were not considered as genetic mutations. After extracting the genomic DNA from peripheral blood, genetic testing was carried out using three methods: fluorescence-based conformation sensitive gel electrophoresis, denaturing high performance liquid chromatography, and direct sequencing. BRCA1/2 mutation testing was conducted by four DNA testing laboratories; all these laboratories are certified annually by the Korean Institute of Genetic Testing Evaluation. Each participating centre was linked to one of four DNA testing laboratories.
In this study, parous women were defined as women with one or more full-term pregnancies. For this analysis, the requirement to obtain separate consents was waived by the Institutional Review Board of Seoul National University Hospital (IRB number: 1511-010-714).
Statistical analysis
We retrospectively analyzed women who carried either the BRCA1 or the BRCA2 mutation. BRCA1 and BRCA2 mutation carriers were separately analyzed. To assess the association between the reproductive factors of the BRCA mutation carriers and breast cancer, we used a cohort study design to compare women with BRCA mutations who developed breast cancers with those that did not. Continuous variables were compared using the Student t-test, and categorical variables were compared using the chi-square tests. Hazard ratios (HR) and 95% confidence intervals were calculated using the logistic regression test. All analyses were carried out using SPSS version 19.0 (IBM Corp., Armonk, USA). Values of p<0.05 were deemed statistically significant.
RESULTS
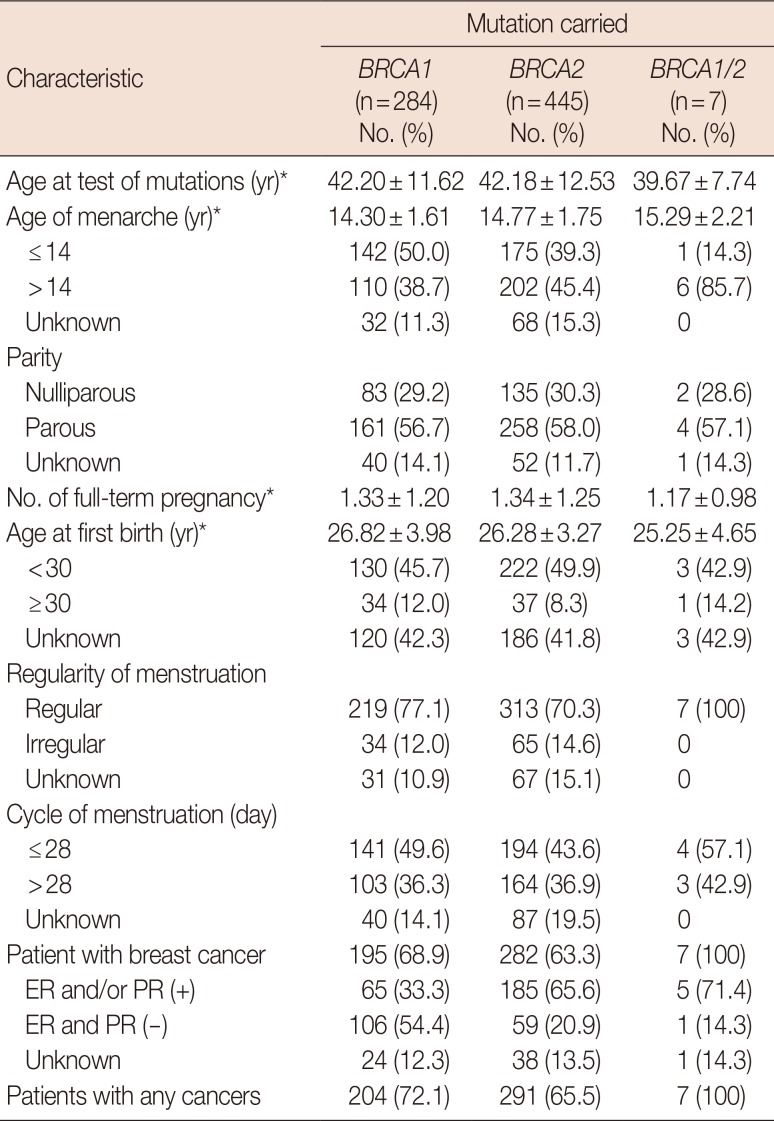
The present retrospective analyses were conducted on a cohort of 739 women with either proven BRCA1 or BRCA2 mutations, or both, who were registered in the KOHBRA study. Among these, three women for whom reproductive histories were unavailable were excluded from the present analysis. There were 284 women with the BRCA1 germline mutation, 445 with the BRCA2 mutation, and seven, who had mutations in both BRCA1 and BRCA2. The characteristics of the entire study cohort and the distribution of reproductive factors among them are presented in Table 1.
The effect of reproductive factors on the development of breast cancers in women with the BRCA mutations
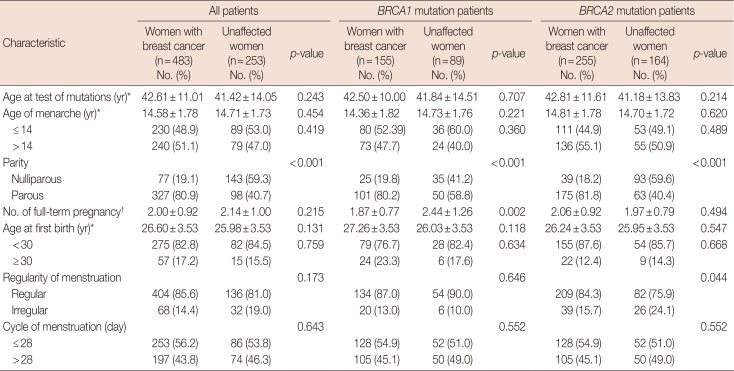
Among the 736 women, a total of 483 had developed breast cancers at the time of their interview. Characteristics of the women with or without breast cancers are listed in Table 2. There were no differences in the risks of breast cancer in these women, based on their regularity and cycles of menstruation. Compared with parous women, nulliparous women were significantly associated with women who did not develop breast cancers, and this association was also observed in the subgroup with BRCA1/2 mutations. However, except in the nulliparous women, the number of full-term pregnancies was lesser in women with breast cancers than in those who did not develop breast cancer, in the group with the BRCA1 mutation (1.87±0.77 vs. 2.44±1.26, p=0.002). The age of first childbirth was not associated with the risks of developing breast cancer.
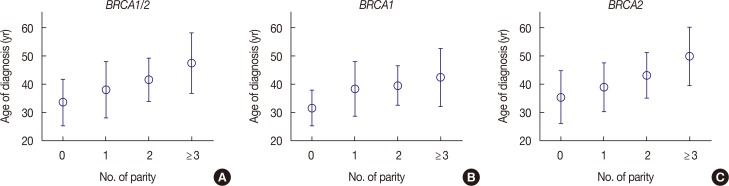
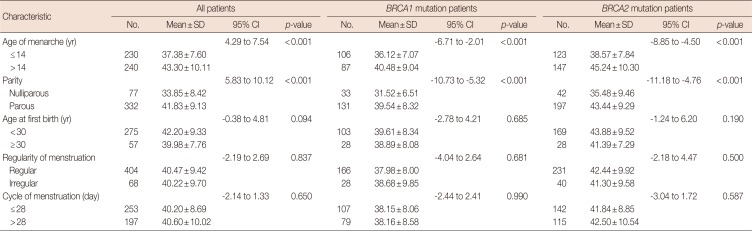
In this study, the mean age of diagnosis of breast cancer in all patients was 39.0 years; in women with the BRCA1 mutation, 38.01±8.31 years, and in women with the BRCA2 mutation, 42.36±10.04 years. The age at menarche and the parity were significantly associated with the age of diagnosis. Women who experienced menarche at 14 years of age or earlier were diagnosed with breast cancer at younger ages than women who experienced menarche at over 14 years of age (37.38±7.60 and 43.30±10.11 years, respectively, p<0.001). Additionally, the number of full-term pregnancies was significantly associated with the age of diagnosis, especially in women with the BRCA2 mutation (p<0.001) (Figure 1). However, the regularity and cycles of menstruation were not significant (Table 3).
Differences in breast cancer stage according to the reproductive factors
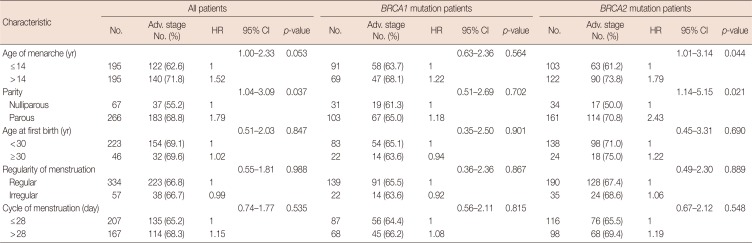
Among 483 patients with breast cancers, 27 had in situ cancers, 391 had stage I–III disease, and 65 had unknown status. We examined the association between the reproductive factors and breast cancer stage. Our analysis showed that the number of parous events was significantly associated with the risk of advanced disease (stage II or III vs. stage I). In all patients, the prevalence of the advanced stage was higher in parous women than in nulliparous women (68.5% vs. 55.2%, p=0.043). The association was more pronounced in women with the BRCA2 mutation (HR, 2.67; p=0.014) (Table 4). With increase in the numbers of full-term pregnancies, the probability of developing advanced breast cancers was higher in parous women than in nulliparous women, in the group with the BRCA2 mutation (Supplementary Table 1, available online).
DISCUSSION
As the BRCA proteins are known to play protective roles against the carcinogenic effects of estradiol [567], we hypothesized that the factors influencing the duration of the reproductive period may affect the characteristics of breast cancer presentation in carriers of the BRCA1 and BRCA2 mutations. In accordance with our hypothesis, we observed that younger age at menarche and nulliparity were strongly associated with early onset of breast cancer. However, our analysis also revealed an unexpected finding that breast cancers in BRCA2 mutation carriers who had early onset of menarche or who were nulliparous were more likely to have early-stage tumors. Bayraktar et al. [9] have reported that late menarche in BRCA1 mutation carriers was associated with advanced stages of breast cancer; in a population-based study, Alsaker et al. [10] reported worse outcomes for breast cancer in women with higher numbers of parous events. In our study, we observed that as the numbers of full-term pregnancies increased, the probability of advanced breast cancers in parous women was higher than the probability in nulliparous women, in the group with the BRCA2 mutation.
The control of cell proliferation is stimulated by increased levels of estrogen during puberty, and especially before the first birth, but may be dysregulated in breast cells that harbor BRCA1/2 mutations [211]. However, the different effects of reproductive factors on breast cancer characteristics in the carriers of the BRCA1 and BRCA2 mutations suggest that responses to hormones may differ between them. A good example of these differences is the fact that only 10% to 24% of BRCA1-associated breast cancers are ER-positive, whereas 65% to 79% of BRCA2-associated breast cancers are ER-positive [1213]. In our study, the age of breast cancer diagnosis was higher in patients with the BRCA2 mutation patients than in those with the BRCA1 mutation, and the effect of reproductive factors on surgical stage was pronounced only in women with the BRCA2 mutation.
Regarding the onset of breast cancer in patients, we found that higher number of parous events and late age of menarche had a protective effect, but this protection may be limited in the number of years. In a recent study, longer time intervals between age at first pregnancy and at breast cancer diagnosis reduced the breast cancer mortalities in premenopausal women [14]. A similar study also found that high parity may have a protective effect against small and low-grade tumors [1516]; consequently, women with high parity may have relatively advanced and more aggressive disease. Additionally, this protective effect of parity may be limited only to ER-positive tumors [17]; however, it has been suggested that high parity may also increase the risks for triple-negative breast cancer [18].
Pregnancy and childbirth have been shown to be protective factors in terms of the lifetime risk of breast cancer in the general population. However, in BRCA mutation carriers, the results from previous studies of the effect of parity on breast cancer have varied. Milne et al. [19] reported that parity was associated with protection from breast cancers in BRCA1 and BRCA2 mutation carriers, and each live-birth was associated with an estimated 13% risk reduction. On the other hand, a study based on 55 international collaborating centers [20] observed that increasing parity was associated with increased risk of breast cancer (15% per live-birth) in women who were BRCA2 carriers. In a recent meta-analysis, the risks of breast cancer in parous women who were BRCA1/2 mutation carriers were not statistically different from the risks in corresponding nulliparous women. Additionally, the risks of breast cancer associated with increasing parity were not significantly reduced [21].
Our study has several limitations. First, our results are based on retrospective data obtained from women who opted for genetic testing for the BRCA1 and BRCA2 mutations. Thus, other factors, such as psychological status or memorial ability, might have influenced the results of the study. Additionally, well-known lifestyle factors, including obesity and alcohol consumption, could have introduced a bias in the results. Second, data on reproductive factors were not available for all women who were BRCA mutation carriers. Third, the relationship between the regularity of menstruation and breast cancer in BRCA mutation carriers was not properly examined. Although most women in this study believed that they had regular cycles of menstruation, the meaning of “regular” may differ among individuals.
This study showed the differential risks of breast cancer associated with reproductive factors in women who were BRCA1/2 mutation carriers. Early menarche and nulliparity were associated with earlier onset of breast cancers in women who were BRCA1/2 mutation carriers. However, parity was associated with more advanced stage at presentation, especially in women who were BRCA2 mutation carriers. Our observations need further testing with longitudinal follow-up data, in a larger cohort of women who are BRCA1/2 mutation carriers.
 XML Download
XML Download