

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer, as an increasing incidence malignancy, is the most common lethal disease in females [1]. Most breast cancer patients have lymph node metastasis when they are initially diagnosed or operated on, which results in a poor prognosis [2]. Although there was no significant improvement on disease-free survival (DFS) and overall survival (OS), lymph node dissection was recently identified to reduce the local recurrence rate in breast cancer patients with node micrometastasis [3]. To date, sentinel lymph node biopsy (SLNB) has become the standard of care as a staging procedure for breast cancer patients with clinically node-negative disease, and regional nodal irradiation after a positive SLNB has been considered as a reasonable alternative to axillary lymph node dissection (ALND) [4]. ALND remains a standard method of treating regional disease not only in patients with clinically positive nodes but also in some SLNB positive patients [5], while the latest researches demonstrated that most SLNB positive patients would be candidates to avoid ALND if they underwent breast-conserving therapy (BCT) [6,7]. Therefore, the accurate evaluation of lymph node metastasis is very important to the procedure of surgery, in addition to the predication the prognosis of breast cancer patients. Unfortunately, there is not an authoritative method for detection the nodal metastasis from breast cancer before surgery. On the other hand, we have to admit the fact that there is not a satisfactorily biomarker with the high specificity and sensitivity for screen the relapse of patients following the mastectomy. Lymphatic metastasis represents a series of sequential processes that include the dissemination and invasion of tumor cells from the primary tumor into the surrounding stromal tissue, penetration of the tumor cells across the lymphatic walls, implantation in the regional lymph nodes, and extravasation and proliferation in the parenchyma of target organs [7]. In general, vascular endothelial growth factor (VEGF)-C and -D have been defined as lymphangiogenic growth factors and play an important role in tumor lymphangiogenesis via activation of the VEGF receptor (VEGFR)-3, which is expressed in lymphatic endothelial cells [8,9]. However, these two biomarkers can not provide the information of dissemination and invasion of tumor cells, penetration of the tumor cells, and so on. These aforementioned defects make VEGF-C and -D not to be widely applicable to diagnosis the lymph node metastasis or to screen the nodal relapse in clinic.
Signal transducer and activator of transcription 3 (STAT3), an important member of the STAT family, is a latent transcription factor that has been shown to act as an oncogene in several malignant diseases [10]. It is well known that STAT3 is activated (phosphorylated STAT3, pSTAT3) in response to the binding of a large number of cytokines, hormones and growth factors to their receptors. Actually, STAT3 has been demonstrated to up-regulate genes encoding apoptosis inhibitors (Bcl-xL, Mcl-1, and survivin), cell-cycle regulators (cyclin D1 and c-Myc) and angiogenesis inducers (e.g., VEGF), which are important molecular cub for tumor progression [11-13]. Recently, several investigators reported that STAT3 aberrant expression were significantly associated with the status of lymph node metastasis in various malignant disease [14-19]. Theoretically, STAT3 has the ability to promote the lymphatic metastasis from malignancy. The detailed correlation between lymph node metastasis and STAT3 expression is not elucidated.
In view of aforementioned causalities, we designed this study for exploration the implication of the STAT3 aberrant expression in breast cancer. They are as follows: 1) to elucidate the STAT3 aberrant expression for predication the OS of breast cancer patients after curative resection; and 2) to initially analyze the correlation between the STAT3 aberrant expression and lymph node metastasis from breast cancer.
METHODS
Patients
A total of 140 patients who underwent potentially curative resection for breast cancer at the Department of Thyroid and Breast Surgery, West China Hospital of Sichuan University between June 2005 and December 2005 were eligible for this study. Eligibility criteria for this study included: 1) histologically proven primary breast cancer, 2) no history of mastectomy or other malignancy, 3) a lack of noncurative surgical factors except for distant metastasis (such as liver, lung, brain, or bone-marrow metastasis) and supraclavicular lymph node metastasis, 4) ALND performed, and 5) no patients died during the initial hospital stay or for 1 month after surgery, 6) no neoadjuvant therapy (including chemotherapy, radiotherapy, and hormone therapy).
Surgical treatment
All patients were operated on according to the potentially curative mastectomy plus ALND method. Curative resection was defined as a complete lack of grossly visible tumor tissue and metastatic lymph nodes remaining after resection, with pathologically negative resection margins. Primary tumors were resected en bloc. The choice of surgical procedure of mastectomy (radical or modified radical mastectomy) was made by the attending surgeon's preference, and based mainly on the breast cancer treatment guidelines. Surgical specimens were evaluated as recommended by 7th American Joint Committee on Cancer (AJCC) TNM classification for breast cancer.
Immunohistochemistry
Paraffin sections (4 µm thick) were deparaffinized and rehydrated. Antigen retrieval treatment was done at 95℃ for 40 minutes in 0.01 mol/L sodium citrate buffer (pH 6.0), and endogenous peroxidases were blocked using 3% hydrogen peroxide for 30 minutes. Purchased antibodies were: rabbit anti-STAT3 (BA0621, 1:100 dilution; Boster, Wuhan, China), rabbit anti-pSTAT3 (AP0247, 1:150 dilution; Bioworld, Nanjing, China), rabbit anti-VEGF-C (BA0548, 1:100 dilution; Boster), rabbit anti-VEGF-D (BA1461, 1:50 dilution; Boster), rabbit anti-Ki-67 (BA1653, 1:150 dilution; Boster), rabbit anti-estrogen receptor (ER) (BA3599, 1:100 dilution; Boster), Wuhan, China), rabbit anti-progesterone receptor (PR) (ZA0255, 1:150 dilution; Zhongshan, Beijing, China), and rabbit anti-human epidermal growth factor receptor 2 (HER2) (RM2112, 1:50 dilution; Lab Vision\Neomarker, Kalamazoo, USA). All sections were incubated overnight with the primary antibody at 4℃. The sections were then treated with peroxidase using the labeled polymer method with Peroxidase (Boster) for 30 minutes. Antibody binding was visualized using the Avidin Biotin Complex Elite Kit and 3,3-diaminobenzine according to the manufacturer's instructions (Molecular Cancer Laboratory, West China Hospital of Sichuan University, Chengdu, China). Sections were then counterstained in hematoxylin. For general negative controls, the primary antibody was replaced with PBS.
Microscopic assessment of STAT3, pSTAT3, VEGF-C, VEGF-D, Ki-67, ER, PR, and HER2 expression
All sections were assessed blindly by two independent observers, and in cases of assessing disagreement a third independent assessment was performed. Staining for STAT3, VEGF-C, and VEGF-D was considered potentially positive if there was cytoplasmic staining. Staining for HER2 was considered potentially positive if there was membraneous staining. The grade of staining intensity of STAT3, VEGF-C, VEGF-D, and HER2 was rated on a scale from 0 to 3, with 0, indicating no staining; 1, weak staining; 2, moderate staining; and 3, strong staining. The intensity scores of 2 and 3 were considered positive staining. Positive staining for pSTAT3, Ki-67, ER, and PR was defined as >25% nuclear staining with more than a moderate intensity for the tumor cell.
Evaluated variables
The following clinicopathological variables were evaluated: 1) age at surgery (<50, or ≥50 years); 2) depth of primary tumor invasion (T stage, according to 7th AJCC TNM classification) (T1, T2, T3, or T4); 3) number of lymph node metastasis (N stage, according to 7th AJCC TNM classification) (N0, N1, N2, or N3); 4) TNM classification (I, II, III, or IV); 5) World Health Organization classification of primary tumor (I, II, or III); 6) STAT3 expression (negative or positive); 7) pSTAT3 expression (negative or positive); 8) VEGF-C expression (negative or positive); 9) VEGF-D expression (negative or positive); 10) Ki-67 expression (negative or positive); 11) ER expression (negative or positive); 12) PR expression (negative or positive); and 13) HER2 expression (negative or positive).
Ethics statement
The study was approved by the Research Ethics Committee of West China Hospital of Sichuan University (2012-251), China. Informed consent was obtained from all patients before participating in the study.
Statistical analysis
Categorical variables were statistically compared a chi-square or Fisher's exact test. Continuous data were shown as mean±SD and were statistically compared using the Mann-Whitney test. The median OS was determined by using the Kaplan-Meier method, and log-rank test was used to determine significance. Factors that were deemed of potential importance on univariate analyses (p<0.05) were included in the multivariate analyses. Multivariate analysis of OS was performed by means of the Cox proportional hazards model, using the forward procedure for variable selection. Hazard ratios (HR) and 95% confidence interval (CI) were generated. Akaike information criterion (AIC) and Bayesian information criterion (BIC) were performed in the multinomial logistical regression model for evaluation the best clinicopathological variable for predication the lymph node metastasis from breast cancer. The smaller are AIC value and BIC value, the better is clinicopathological variable for predication the lymph node metastasis. In all statistical analyses, significance was defined as p<0.05 and the statistical significance was two sided. The OS analysis of all patients was initially completed in March 2012. All statistical analyses were performed with statistical analysis program package SPSS version 18.0 (SPSS Inc., Chicago, USA).
Follow-up
After curative surgery, all patients were followed every 3 months for 2 year, then every half a year or until death. The median follow-up for the entire cohort was 54 months (range, 18-79 months). The follow-up of all patients who were included in this study was completed in February 2012. Serum values of CEA and CA 15-3, B ultrasonography, chest X-ray, and radionuclide bone scan were obtained with every visit.
RESULTS
Patient characteristics
The clinicopathological characteristics and biomarkers' expression of 140 breast cancer patients after curative resection are shown in Table 1. The 5-year survival rate (5-YSR) of all enrolled patients was 83.5%, and 111 patients were alive when the follow-up was completed.
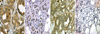
Immunohistochemical staining for STAT3, pSTAT3, VEGF-C, VEGF-D, Ki-67, ER, PR, and HER2 in breast cancer or adjacent nontumor tissues
STAT3, VEGF-C, and VEGF-D expression was observed in the cytoplasm. Staining for pSTAT3 and Ki-67 appeared in the cell nucleus. STAT3 positive expression, pSTAT3 positive expression, VEGF-C positive expression, VEGF-D positive expression, Ki-67 positive expression, ER positive expression, PR positive expression, and HER2 positive expression were respectively detected in 87 (62.1%), 67 (47.9%), 58 (41.1%), 34 (24.3%), 87 (62.1%), 64 (45.7%), 72 (51.4%), and 41 (29.3%) of 140 breast cancer specimens, whereas 27 (19.3%), 14 (10.0%), 31 (22.1%), 16 (11.4%), 20 (14.3%), 13 (9.3%), 16 (11.4%), and 0 (0%) of 140 adjacent nontumor tissue specimens were assessed as STAT3 positive expression, pSTAT3 positive expression, VEGF-C positive expression, VEGF-D positive expression, Ki-67 positive expression, ER positive expression, PR positive expression, and HER2 positive expression, respectively. There were significantly statistical differences in the positive expression incidences of STAT3 (p=0.024), pSTAT3 (p=0.015), VEGF-C (p=0.032), VEGF-D (p=0.040), Ki-67 (p=0.011), ER (p=0.004), PR (p=0.025), and HER2 (p<0.001), between breast cancer and adjacent nontumor tissue specimens, respectively (Figures 1, 2, 3, 4).
Univariate and multivariate survival analysis
With univariate analysis (Kaplan-Meier method), we found five clinicopathological variables and biomarkers' expression had significant associations with the OS of breast cancer patients after curative resection. They are as follows: N stage, TNM classification, STAT3 expression, pSTAT3 expression, Ki-67 expression, ER expression, and PR expression. All above seven variables were included in a multivariate Cox proportional hazards model (forward stepwise procedure) to adjust for the effects of covariates. In that model, only number of lymph node metastasis was identified as the independent predicators with the OS of breast cancer patients postoperatively (HR, 3.220; 95% CI, 2.257-4.594; p<0.001) (Table 2, Figure 5).
Correlation analysis between STAT3 expression and other variables in 140 breast cancer patients
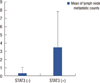
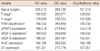
A univariate analysis (chi-squire test) identified nine variables that had statistically significant associations with STAT3 expression from breast cancer: age at surgery, T stage, TNM classification, N stage, ER expression, pSTAT3 expression, VEGF-C expression, VEGF-D expression, and Ki-67 expression (Table 3). All the nine variables were included in a multinominal logistic regression to adjust for the effects of covariates to lymph node metastasis from breast cancer. In that model, AIC and BIC values were executed by using the multinomial logistic regression according to STAT3 expression of patients when the follow-up was over. We demonstrated that both AIC value and BIC value of N stage were the smallest (AIC value, 176.930; BIC value, 256.355) in the aforementioned nine relative factors of lymph node metastasis from breast cancer, which indicated that N stage was the most important predicator of STAT3 expression in breast cancer (Table 4, Figure 6).
DISCUSSION
Lymph node metastasis from breast cancer is a complex pathophysiological process of cancer progress, which is mainly associated with the biological habits of cancer cells. Usually, biological factors may directly affect the end-results of the malignant cells to selectively invade lymph nodes rather than visceral organs, just as certain tumor types metastasize to certain organs and not others [20]. Exact recognition of the lymph node metastatic status is considered as the important clue for contribution to not only choice the appropriate surgical procedure of lymph node dissection, but improvement the prognostic predication. To date, SLNB has become the standard of care as a staging procedure for breast cancer patients with clinically node-negative disease [5]. The current guidelines recommend completion ALND when lymph node involvement is identified by SLNB [4], although the need for completion ALND has been questioned [2]. Kim et al. [21] reported that approximately 50% of patients had additional nonsentinel axillary nodal metastases, which indicated that ALND might improve the prognosis of breast cancer patients. Furthermore, Park et al. [6] found that axillary recurrences were more frequent in a group of 287 patients who underwent SLNB alone compared with those who underwent completion ALND (2.0% vs. 0.4%, p=0.004). Therefore, we have to believe that the exact diagnosis of nodal metastasis from breast cancer is a crucial factor for application the correctly surgical procedure and decrease the recurrence rate.
However, there is not an optimal method for exact detection the lymph node metastatic status before surgery. The insidiously nodal metastasis and micrometastasis of lymph nodes are so difficult to be detected with the general examinations. Biomarkers are high hopes for accurate prediction the lymph node metastasis from primary tumor. In theory, cancer cell metastasis should be considered to involve the cell proliferation, antiapoptosis, invasion enhancement, and lymphangiogenesis. According to these biological characteristics, STAT3, a cub of molecular regulator in various malignancies, is competent to evaluate the lymph node metastasis, rather than other conventional lymphangiogenetic factors [10-13].
In many solid tumors, overexpression of human epidermal growth factor receptors (e.g., HER1/EGFR and HER2) correlates with poor prognosis. As a poor prognostic factor, EGFR overexpression is frequently shown in the breast cancer cells and tissues [22]. The key one of the down-stream molecules of EGFR which is identified to the oncogenesis in various organs is STAT3 [23]. Actually, STAT3 is constitutively activated by aberrant upstream tyrosine kinase activities in a broad spectrum of cancer cell lines and human tumors. STAT3 is an oncogenic protein that is constitutively activated in many human cancers, including 30% to 60% of primary breast cancers [22]. The biological significance of STAT3 activation in breast cancer is not fully understood. STAT3 activation may modulate tumor invasiveness of breast cancer by regulating TIMP1 expression. Pytowski et al. [24] generated an in vitro system in which active STAT3 levels can be tightly controlled in breast cancer cells by using MCF-7 cells transfected with tetracycline-off constitutively active STAT3. Using immunohistochemistry and 142 primary breast tumors, they also found a significant association between the expression of the phosphorylated/active form of STAT3 (pSTAT3) and that of tissue inhibitor of matrix metalloproteinases-1 (TIMP-1) [24]. At present study, we demonstrated there were significantly statistical differences in the positive expression incidences of STAT3, and pSTAT3 between breast cancer and adjacent non-tumor tissue specimens. In addition, we also found that both STAT3 expression and pSTAT3 expression were significantly associated with the OS of breast cancer patients after curative resection. Therefore, we did consider that STAT3 was a pivotal biomarker for predication the prognosis of breast cancer. As other investigators reported, STAT3 was significantly associated with the bad prognosis in various human malignancies [18, 25-27].
Lymph node metastasis was well known as the most important predicator of prognosis of breast cancer after surgery. Recently, several investigations demonstrated that STAT3 was involved in a series of molecular events of lymph node metastasis in different human cancers [11-15]. From the results of this study, we found that lymph node metastasis was the only independent predicator of the OS of breast cancer patients after surgery. Although we demonstrated that nine variables (including VEGF-C expression, VEGF-D expression, and Ki-67 expression) that had statistically significant associations with lymph node metastasis from breast cancer, the STAT3 expression was the most important predicator of lymph node metastasis from breast cancer by using the multinomial logistical regression model analysis rather than other variables.
Notwithstanding a small scale study was performed, we concluded that STAT3 might improve the cancer cell lymphatic metastasis, which induced the bad prognosis of breast cancer patients. The anti-STAT3 monoclonal antibody might change treatment status in the nodal metastasis from breast cancer, which is worthy of hoping for further improvement the prognosis of patients.







 XML Download
XML Download