

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast-conserving surgery (BCS) has become the standard treatment for early-stage breast cancer since randomized trials showed that BCS followed by adjuvant radiation therapy is the equivalent to a total mastectomy in terms of overall and disease-free survival among patients with early-stage breast cancer [1,2]. Because BCS provides a better cosmetic outcome, and generally, a better quality of life than mastectomy, the rate of BCS is increasing. In Korea, the rate of BCS increased from 18.7% in 1996 to 55.7% in 2010 [3]. According to the breast cancer database at our institution, BCS was performed for 413 (51.4%) of 764 cases of breast cancer between June 2003 and December 2007, and the rate of BCS has increased annually (39.4% in 2004, 47.2% in 2005, 60.4% in 2006, and 63.0% in 2007) [4]. However, BCS has been associated with a higher risk of local recurrence than mastectomy [1], and the most important factor associated with local recurrence after BCS is the presence of tumor cells at the surgical resection margin [5,6]. Successful BCS requires a clear pathological resection margin, while maintaining an acceptable cosmetic result, but a significant proportion of patients undergoing BCS have a positive resection margin that requires re-excision. Re-excision rates vary from 15% to 60% [7-10]. Although re-excision after BCS does not affect survival, it can cause delays in the administration of adjuvant chemotherapy and radiation therapy. Moreover, additional surgery increases morbidity, patient anxiety, wound infection rates, leads to poor cosmetic results, and adds to the costs of care, and thus, efforts to reduce the re-excision rate are important. Several risk factors associated with positive margins have been evaluated in previous studies. Younger age, smaller breasts, large tumor size, multifocality, lobular histology, presence of lymphovascular invasion (LVI), presence of ductal carcinoma in situ (DCIS), nodal involvement, and microcalcification upon mammography (MMG) have all been reported to influence the risk of re-excision, but study results vary considerably [7-14].
In this study, we aimed to assess the re-excision rates after BCS for early-stage breast cancer, and to evaluate the factors associated with re-excisions after BCS. In addition, we performed resection margin analyses to evaluate differences in resection margin status based on tumor location.
METHODS
Between June 2003 and February 2011, 986 patients with invasive breast cancer underwent BCS at Seoul National University Bundang Hospital. A total of 726 of these were pathologically confirmed with early-stage breast cancer (pathologic T stage I and II) after surgery. Patients who underwent neoadjuvant chemotherapy and those with distant metastasis were excluded. We thus retrospectively reviewed the medical records of 701 patients; 10 of these patients had bilateral breast cancer and underwent bilateral BCS, giving a total of 711 cases of BCS. This study was approved by the Seoul National University Bundang Hospital Institutional Review Board (IRB No. B-1203/148-112).
Age, body mass index (BMI), clinical T and N stage, and palpability were recorded and analyzed. Clinical stage was evaluated by physical examination and radiologic findings were obtained from electronic medical records. We classified mammographic findings into 4 categories: no visualization, mass, microcalcification, and mass with microcalcification. We identified the presence of daughter nodules by ultrasonography (USG) and non-mass-like enhancement (NMLE) by breast magnetic resonance imaging (MRI). From pathologic reports, we obtained the pathologic stage, histologic type and nuclear grade, pathologic multifocality, hormone receptor status, presence of DCIS and LVI, tumor border type, and resection margin width in 4 directions (superior, inferior, medial, and lateral). Breast cancer staging was based on the seventh staging system of the American Joint Committee on Cancer/International Union against Cancer [15].
All operations were performed under general anesthesia by one specialized breast cancer surgeon. Palpable tumors were excised with the acceptable margin width of more than 1 cm by intraoperative palpation. Non-palpable tumors were marked by USG-guided or MMG-guided needle localization before surgery. In some cases with non-palpable tumors, specimen mammography was performed to confirm the adequate resection. The intraoperative frozen section for resection margin evaluation was not performed routinely. Re-excision was performed for patients with a positive or close resection margins (> 0 to ≤ 2 mm) microscopically. A positive surgical margin is defined as the presence of tumor cells at the inked surface of the resected specimen. The operation for re-excision was also performed under general anesthesia in most of cases. In many cases, wide excision of the involved margin was sufficient for re-excision. Total mastectomy was performed for re-excision in some patients who expected poor cosmetic result after secondary BCS, and who wanted surgery without the possibility of further re-excision.
Statistical analyses were performed using SPSS version 19.0 (SPSS Inc., Chicago, USA). Pearson's chi-square or Fisher's exact test for categorical variables, and Student's t-test for continuous variables were used to identify associations between each of the clinicopathological factors and re-excision after BCS. Multivariate analysis was performed using logistic regression of the variables that were found to be statistically significant through univariate analyses. One-way ANOVA was used for the analyses of resection margins.
RESULTS
Clinicopathological characteristics
The mean age of patients was 50.8±11.3 years, and the mean BMI was 23.3±3.2 kg/m2. The characteristics of tumors are presented in Table 1. In total, 557 (78.3%) cases were clinically assessed as T1 and axillary lymph node metastasis was clinically suspected in 58 (8.2%). In comparison, 503 (70.7%) cases were reported as pathologic T1 and axillary lymph node metastasis was found in 183 (25.7%). A palpable lesion was present in 523 (73.6%). A total of 210 patients (29.5%) had no visible lesion on preoperative MMG due to dense breast parenchyma; mass lesions and microcalcification were identified in 432 (60.8%) and 194 (27.3%) patients, respectively. Daughter nodules were found in 100 (14.1%) patients upon preoperative breast USG, and NMLE was found in 35 (4.9%) patients upon breast MRI. One hundred twenty-eight (18.0%) patients had multiple lesions according to the pathologic reports. Five hundred ninety-eight (84.1%) had ductal type and 36 (5.1%) had lobular type carcinomas. Approximately 75% had a DCIS component, and LVI was found in 215 (30.2%).
Re-excision rate after BCS
Of the 711 cases of BCS for early-stage breast cancer, 71 (10.0%) required re-excision due to a positive or close resection margin. Among these 71 cases, the resection margins of 57 were involved with invasive breast cancer (n=20) or DCIS (n=37) and the remaining 14 had a close resection margin (≤2 mm) with invasive breast cancer (n=8) or DCIS (n=6). A second BCS was performed in 51, and a total mastectomy (TM) in 18. A 37-year-old woman scheduled for TM was lost to follow-up before re-excision, and a 40-year-old woman who had a positive resection margin refused re-excision, and only attended regular follow-up sessions. Of the 51 patients who underwent a second BCS, 12 (23.5%) required a second re-excision; a third BCS was performed in 4 patients and a TM in 8. No patients required a third re-excision. Thus, of the 711 cases of early-stage breast cancer for which BCS was planned, 685 (96.3%) were successfully managed without mastectomy.
Factors affecting re-excision
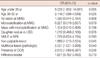
Upon univariate analysis (Table 2), the mean age of the no re-excision group was found to be higher than that of the re-excision group (51.2 years vs. 47.1 years; p=0.002); in addition, the under 35-year-old subgroup had significantly higher re-excision rates than the other age groups of 36 to 50 and over 50 (19.1% vs. 12.1% and 6.5%, respectively; p=0.005). Non-palpability (14.6% vs. 8.6%; p=0.022) was also associated with a high re-excision rate. BMI, tumor location, and clinical stage were not associated with re-excision. The presence of NMLE upon MRI was associated with re-excision, and the lack of a visible lesion and microcalcification during MMG and daughter nodules upon USG showed a relative association with re-excision upon univariate analysis. Pathologic multifocality (18.0% vs. 8.2%; p=0.001), the presence of a DCIS component (11.3% vs. 5.8%; p=0.036), and an infiltrative tumor border (10.8% vs. 5.8%; p=0.041) were found to be significantly associated with re-excision upon univariate analysis. Pathologic stage, histologic type, and LVI were not found to be associated with re-excision.
Multivariate logistic regression analysis was performed with the variables associated with re-excision through univariate analysis (variables with p<0.1). The results are shown in Table 3. Younger age, non-palpable lesions, multifocality, and the presence of a DCIS component were identified as being independently associated with re-excision after BCS. Of these factors, age, MMG, USG, and MRI findings, and palpability can be measured preoperatively.
Resection margin analyses
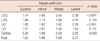
We analyzed the positive resection margin rate and the resection margin width in 4 directions - superior, inferior, medial, and lateral - among 5 subgroups categorized by tumor location, namely the upper outer quadrant (UOQ), lower outer quadrant (LOQ), upper inner quadrant (UIQ), lower inner quadrant (LIQ), and the central region. In this analysis, 6 cases were excluded for ambiguous tumor location, and finally, 705 cases (2,820 resection margins) were evaluated. The rate of resection margin involvement across all directions was 2.6%. The positive margin rate was highest at the medial margin and was lowest at the lateral margin, but this difference was not significant (3.3% vs. 2.0%, p=0.517). The mean resection margin width across all 4 directions was 2.0 cm, and the lateral margin width was relatively wider than that of the other directions. Among the 5 subgroups, the LIQ subgroup had the highest rate of positive resection margins (4.2%), especially with respect to the superior and medial margins (5.6%). The LIQ subgroup also had the narrowest mean resection margin width as the superior, medial, and lateral resection margin widths were all narrowest in the LIQ subgroup. In the UOQ, UIQ, and central subgroups, the mean resection margin width was found to be significantly different in different directions. This was because the lateral resection margin width was found to be relatively wider than the width of the other margins. For detailed results relating to the positive resection margin rate see Table 4; results pertaining to resection margin width are shown in Table 5.
DISCUSSION
We aimed to evaluate the re-excision rate after BCS and to identify factors associated with re-excision. The re-excision rate at our institution was 10.0%. Univariate analysis indicated that younger age, the presence of NMLE at MRI, a non-palpable lesion, multifocal lesions noted in pathologic reports, the presence of a DCIS component, and an infiltrative tumor border were significantly associated with re-excision, and no visible lesion, microcalcification upon MMG, and a daughter nodule upon breast USG tended to be associated with a higher rate of re-excision. However, multivariate analysis revealed that only the factors of younger age, non-palpable lesions, multifocal lesions, and the presence of a DCIS component were independently associated with re-excision after BCS.
Reported re-excision rates vary widely [7-10]. The 10% re-excision rate at our institution is comparable with the rates reported previously, despite an intraoperative frozen section for resection margin not being performed at our institution. Studies that involved an assessment of intraoperative frozen sections have reported re-excision rates ranging from 11.3% to 20% [16,17]. Of the 51 patients who underwent a second BCS for the first re-excision, 12 (23.5%) required a second re-excision. This is a very high rate compared with the first re-excision rate. This tendency was also found in a previous study of multiple re-excisions after BCS [18]. Given this finding, the performance of a second BCS for re-excision requires more careful consideration than the performance of the first BCS. Especially when planning a second BCS for re-excision, the patient should be informed of the possibility that the risk of a further re-excision is higher than that associated with the first re-excision. On the other hand, 96.3% of cases for which BCS was initially planned achieved breast conservation in this study, and previous studies have reported that multiple re-excisions do not affect local recurrence or systemic failure [18,19]. Overall, when breast surgeons are planning a re-excision surgery, they must consider the possibility of a second re-excision, the patient's general condition, the desired cosmetic result, the patient's preference, and cost effectiveness.
Univariate analysis identified several risk factors for re-excision. Most of these factors have been studied previously; our findings are both consistent and different from those reported in other studies. Aziz et al. [10] reported that younger age, the presence of a DCIS, larger tumor size, and LVI were significantly associated with a positive resection margin upon univariate analysis, but age was the only factor found to be significant upon multivariate analysis. Cabioglu et al. [13] found, through multivariate analysis, that multifocality was a risk factor for a positive margin, whereas Kurniawan et al. [9] reported that microcalcification upon MMG, multifocal disease, and a larger tumor size were associated with a positive margin upon multivariate analysis. Ramanah et al. [20] identified multifocality, the presence of a DCIS, and the absence of a preoperative positive histologic diagnosis as factors predicting re-excision. Miller et al. [11] also reported the presence of a DCIS as a predictor of a positive margin. Lovrics et al. [21] reported that palpability, the absence of multifocality and LVI, a preoperatively confirmed diagnosis, a small tumor, ductal histology, cavity margin dissection, and larger volumes of excision were predictors of negative margins. NMLE upon MRI was found to be a significant factor associated with re-excision in the univariate analysis performed in the present study. In previous studies, DCIS, invasive lobular carcinoma, focal adenosis, and fibrocystic changes can appear as a NMLE upon MRI, and estrogen receptor-negative invasive ductal carcinoma can also be seen as a NMLE in less than 20% of cases [22,23]. NMLE has also been reported to have various positive predictive values for malignancy based on enhancement patterns [24] and has been reported as the major cause of false-positive breast findings [25]. More definitive and specific studies of NMLE, as viewed by MRI and resection margins, are needed. Daughter nodules upon USG and microcalcification with no visible lesion upon MMG showed a tendency to be associated with re-excision. These preoperative radiologic findings were not found to be significantly associated with re-excision in multivariate analysis. NMLE observed by MRI and daughter nodules seen by USG were significantly associated with pathologic multifocal disease in the present study, and no visible lesion and microcalcification upon MMG were associated with non-palpability. These factors must thus be considered together when planning BCS. A pathologic infiltrative tumor border was also identified as significant in univariate analyses, but was not significant in multivariate analysis. Large tumor size, LVI, and lobular histology have been reported to be significant in several previous studies [8,9,13,14,21], but no significant association between these factors and re-excision was found in the present study.
Multivariate analysis indicated that 4 factors were significantly associated with re-excision. In younger patients, the re-excision rate was high. Many previous studies have reported similar results [7,9,10,13,14]. Because the cosmetic result is thought to be more important in young patients, the extent of excision might be minimized for cosmetic reasons in such patients [26]. Non-palpable tumors were also identified as a risk factor for re-excision in multivariate analysis. Some previous studies have reported a high re-excision rate with non-palpable tumors due to potential technical difficulties [21,27]. Many methods of reducing the positive resection margin rate of non-palpable tumors have been proposed. Needle localization is the most popular and traditional method. A study of needle localization reported the same positive resection margin rate for palpable tumors and needle-localized non-palpable tumors, but the rate remained high (38%) [28]. USG-guided resection has also been suggested for reducing the resection margin positive rate [29]. Radio-guided occult lesion localization and radioactive seed localization have also been performed at some institutions. These radio-guided techniques reportedly have better resection margin outcomes [30]. Multifocal tumors were also identified as a risk factor for re-excision. Although multifocality was identified based on pathological reports in our study, the number of preoperatively suspected multifocal tumors was not very different from the number observed. If a multifocal tumor is suspected, careful planning and performance of BCS are always required. The presence of a DCIS component was identified as an independently associated risk factor in the present study, supporting the findings of a number of previous studies [9-11,20].
At our institution, tumor involvement of the resection margin relative to the total resection margin was 2.6%. As can be seen in Table 4, the positive resection margin rate was highest in LIQ tumors. In particular, the superior and medial margin of LIQ tumors showed a tendency toward a higher involved resection margin rate. The width of the resection margin was relatively narrow in LIQ tumors, especially the width of the superior and medial margins. This finding was due to the relatively small volume of the LIQ. Given these findings, ensuring a wider resection margin at the superior and medial sides of LIQ tumors is worth considering, but this could cause poor cosmetic results. Oncoplastic surgery, such as the use of a partial flap and the insertion of a prosthesis, could be an option for obtaining both a clear resection margin and a better cosmetic result.
This study had several limitations. First, as it was a retrospective study it may be subjected to selectional bias. Second, some of the identified risk factors, such as the presence of a DCIS component and pathologic multifocality, were only noted postoperatively and cannot be considered when planning surgery.
In conclusion, the re-excision rate at our institution was low, even though intraoperative frozen section was not performed. When we plan a BCS for early-stage breast cancer, non-palpable tumors, multifocal tumors, the presence of a DCIS component, and the age of the patient should be considered to ensure proper surgical management and to lower the re-excision rate. We also identified a tendency for the positive resection margin rate and width to differ based on tumor location; for example, a high positive resection margin rate and a relatively narrow width of the superior and medial margins were observed for LIQ tumors, and these factors could have a great impact on surgical planning.



 XML Download
XML Download