

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary breast sarcomas are rare tumors that originate from the mesenchymal tissue of the breast. In a study conducted at the Mayo Clinic, the prevalence of primary breast sarcomas among breast cancers was found to be 0.0006% [1]. Primary leiomyosarcoma of the breast is more rarely observed, and only 24 cases have been reported in the English medical journals. In the present study, we present a case involving primary leiomyosarcoma of the breast and we discuss optimal treatment options.
CASE REPORT
A 48-year-old female patient was referred to our hospital because of pain and a mass in the breast. She noticed a lump in her right breast 8 months earlier. In the following months, this lump had grown rapidly and led to a tightening of the skin of the right breast.
A physical examination revealed a tender mass that was 10 cm in size and extended from the upper outer quadrant of the right breast to the lower outer quadrant. There was neither retraction of the nipple nor palpable axillary or supraclavicular lymphadenopathy. The contralateral breast was normal. Mammography and ultrasonography revealed a well-circumscribed tumor mass that was 8×6 cm in size and located in the upper and lower outer quadrants of the right breast (Figure 1). Because of evidence of malignancy in the fine needle aspiration biopsy, the patient underwent total mastectomy of the right breast, total excision of the pectoralis major muscle due to invasion in the pectoral muscle, and axillary lymph node dissection.
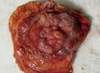
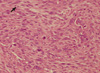
In the macroscopic pathological examination of the mastectomy specimen, a necrotic tumoral mass that was 10×9×6 cm in size was observed and invasion into the overlying breast skin and pectoralis major muscle was evident (Figure 2). Microscopically, the tumor was composed of pleomorphic spindle cells showing frequent mitoses and necrosis. Tumor cells demonstrated diffuse immunohistochemical staining with smooth muscle actin (SMA) (Figures 3-5). No staining was observed with desmin, S100, CD117. According to the histopathological and immunohistochemical analysis, the tumor was diagnosed as leiomyosarcoma.
None of the 31 excised lymph nodes exhibited metastasis, and the surgical margins showed no trace of tumor tissue.
A follow-up thoracoabdominal computed tomography scan and bone scintigraphy performed 1 month after the operation were normal.
DISCUSSION
Primary leiomyosarcoma of the breast is rare and is considered an uncommon breast tumor. Only around 30 cases have been reported in English medical journals. Because of the rarity of the tumor more patient data should be presented for the development of a proper treatment strategy.
Leiomysarcoma of the breast may originate from the muscular blood vessels or from the smooth muscle of the nipple [2,3]. It is quite difficult to diagnose leiomyosarcoma preoperatively [4].
Differantial diagnosis includes leiomyoma, spindle cell myoepithelioma and spindle cell sarcomatoid carcinomas as seen in spindle cell purely epithelial metaplastic carcinomas (spindle cell squamous metaplastic carcinoma and adenocarcinoma with spindle cell differentiation). In leiomyomas the tumor cells bland, without evidence of atypia and mitoses. Tumoral necrosis is also not observed. Malign myoepithelioma often lacking significant atypia, few mitosis, and at the periphery of the lesion, more epitheloid cell population is evident emanating from the myoepithelial cell layer of the entrapped ductules. In myoepithelioma tumors cells are SMA (+) and S-100 (+). Metaplastic carcinomas of the breast is a general term referring to a heterogeneous group of neoplasms. Leiomyosarcoma of the breast should be distinguished from spindle cell purely epithelial metaplastic carcinomas (spindle cell squamous metaplastic carcinoma and adenocarcinoma with spindle cell differentiation). In spindle cell squamous metaplastic carcinomas, tumor cells are epithelial in origin and positive for cytokeratins and negative for SMA. In adenocarcinoma with spindle cell metaplasia, the tumor is composed of tubules admixed with neoplastic spindle cells. These spindle cells immunoreact with epithelial markers including Cytokeratin 7 and are negative for SMA. In these case the tumor cells demonstrated diffuse immunohistochemical staining with SMA. No staining was observed with desmin, S100, CD117, pancytokeratin, and cytokeratin 7. According to the histopathological appearance and immunohistochemical staining, the tumor was diagnosed as leiyomyosarcoma.
Establishing an accurate diagnosis is crucial in planning treatment. To date, this type of tumor has been observed to affect middle-aged women (mean age, 56 years) and manifests as a mass in their breast over a long period of time. The average tumor size is 4.7 cm [2,4]. Because two of the reported cases were in males, the involvement of endocrine factors in this tumor appears to be unlikely [2]. This type of tumor tends to show local recurrence and distant metastasis has been observed in 25% of patients [5,6]. Metastatic spreading usually occurs via the hematogenous route. Tumor size is believed to have no significant correlation with metastasis [5]. The studies published to date show that the tumor presents itself as a long-standing and slow-growing mass. The duration of symptoms varies between 2 weeks and 5 years, confirming those characteristics [5]. Local recurrence and distant metastases can arise even after 15-20 years [7]. Chen et al. [8] and Nielsen [9] lost their patients 16 and 20 years, respectively, after the operation due to hepatic and multiple metastases.
The tumor is usually observed as a dense, well-circumscribed, fibroadenoma-like mass. It is difficult to reach a diagnosis based on fine needle aspiration (FNA) cytology. However, preoperative diagnosis can be achieved using a combination of FNA cytology and immunohistochemistry [3,10].
Leiomyosarcoma is characterized by spindle-shaped cells with pleomorphic, hyperchromatic and elongated nuclei; eosinophilic cytoplasm; large nucleoli; and significant mitoses. Definitive diagnosis is established through histological examination, in which positive staining is observed immunohistochemically with desmin, vimentin, and muscle-specific actin, whereas negative staining is seen with cytokeratin, myoglobin, and S-100 [2]. Because leiomyosarcoma often invades peripheral tissues, such as the skin and fascia, curative surgery requires a wide resection. Because there has been no reported cases of lymph node metastasis in which dissemination occurred via the hematogenous route, axillary lymph node dissection is unnecessary if leiomyosarcoma diagnosis can be achieved before or during the operation [4-6]. In the present case, there was no axillary lymph node involvement. Wide resection was performed due to the invasion of the pectoralis major muscle by the tumor. The benefits of chemotherapy and radiotherapy have not yet been confirmed [3,5].
The prognosis of leiomyosarcoma is better than that of other breast sarcomas [5]. The prognostic factors are not fully known because of the limited number of studies. However, large tumors with frequent atypia and mitoses appear to be malignant [2].
Based on the published case reports, the characteristics of primary leiomyosarcomas of the breast are well-circumscribed, slow-growing tumors showing a tendency for skin and muscle invasion. In cases where diagnosis can be achieved before or during the operation, wide resection should be performed. There is no need for axillary lymph node dissection. They require long-term follow-up because local recurrence and distant metastasis can occur long after the operation. The benefits of chemotherapy, radiotherapy, and hormonal therapy are still controversial. It has a better prognosis than other breast sarcomas. However, there is a need for further studies to determine the prognostic factors.



 XML Download
XML Download