

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast conserving surgery (BCS) has been approved to treat breast cancer, and this has an equivalent patient survival rate in comparison to mastectomy, and an acceptable cosmetic result can be obtained.(1) Women who undergo breast surgery want to have a better cosmetic outcome and there are several methods to satisfy the patient such as autogenous tissue reconstruction. Yet autogenous tissue reconstruction may require much skill and experience by the surgeon and there is the inevitable scar.
Wide local excision without immediate volume replacement is associated with cosmetic failure in about one third of these patients.(2) Particularly, in case of a small breast, immediate volume replacement is needed for improving the cosmetic outcome.
The absorbable synthetic polyglycolic acid mesh was proposed first as a filling material for the defect after breast surgery in 2003.(3) Thereafter, there were some reports about this technique with advantage of a simple procedure and satisfactory cosmetic outcome in Japan.(4-6) In the present study, we present our surgical methods and the esthetic results of volume replacement using absorbable surgical mesh (Polyglactin 910, Vicryl®, Ethicon, Norderstedt, Germany), which was expected to fill the postoperative defect by inducing reactive fluid and granulation as a foreign body reaction.
METHODS
Between May 2005 and November 2006, 25 patients underwent partial mastectomy for early breast cancer or benign breast disease with using absorbable surgical mesh reconstruction. In patients with benign breast disease, these operations were performed in patients who had the possibility of postoperative asymmetry due to small breast, underwent wide resection due to the possibility of malignancy, or had defect in the lower portion of the breast. The patients were all female and their median age was 46 (range: 32-62) yr. Endoscopy-assisted partial mastectomy with/without sentinel node biopsy was performed as described elsewhere.(7) In brief, the retromammary space of the quadrant to be excised was dissected gently through the axillary incision by using a Vein Harvest and Powerstar scissors (Ethicon, Somerville, USA) under the view of an endoscopic monitor. After completing the dissection of the retromammary space, we made the periareolar semicircular incision to create the skin flap and to resect the tumor-containing quadrant by using Visiport (5-11 mm, Auto Suture, Norwalk, USA). The whole skin of the breast and areola was conserved.
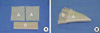
Absorbable surgical mesh reconstruction consists of 3 steps: 1) an absorbable surgical mesh (Polyglactin 910, Vicryl®) is folded several times to a 0.8 cm width and this is sutured at one end to become fan-shape; 2) it is wrapped up in oxidized regenerated cellulose (Interceed®, Ethicon, Somerville, USA) for prevent adhesion between the skin or the pectoralis muscle and the mesh (Figure 1); and 3) it is inserted into the postoperative defect and fixed to the breast tissue by one point of stitch (Figure 2).
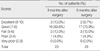
The cosmetic appearance was evaluated at 3 and 6 months after the operation. The cosmetic results of this study were measured using a simplified five-grade for five-items scoring system that consisted of two variables (by patient oneself and a male breast-specialty surgeon) at the time of follow up examination. We modified the five-item-by-four-step method designed by Yamashita.(8) The patients were questioned about five items that consisted of volume symmetry in relation to the other breast, shape, the nipple-areolar complex situation, scar and the overall satisfaction. Subjective patient satisfaction for each five items was scored as excellent,(9-10) good,(7-8) fair,(5-6) poor(3-4) or very poor.(0-2) A male breast-specialty surgeon also examined the patients for the same items. Photographs for presentation were taken at about 3 and 6 months after the operation in patients who agreed to be photographed (Figure 3).
RESULTS
The locations, size and pathologic types of the tumors are summarized in Table 1. The mean follow-up period was 11.5±5.1 months (range, 2-19 months) and no major complication was noted. Ultrasonography of the breast was performed at about 3 and 6 months to survey any possible event. The ultrasonographic findings showed a firm-walled seroma that contains some reactive fluid and granulation tissue. This finding was confirmed grossly and pathologically in one patient who underwent completion total mastectomy according to postoperative pathologic report; multifocal ductal carcinoma in situ. In five cases, the volume of the seroma was too small to obtain a cosmetic effect, and so sterile saline was injected into the cavity under ultrasonographic guide. In contrast, reactive fluid was aspirated in three patients because of too large a seroma volume. Aspiration of the seroma or injection of saline was performed in accordance with the patient's own cosmetic satisfaction.
Table 2 documents the scores of the parameters of cosmesis as assessed by the patients and surgeon at 3 and 6 months after surgery. The overall cosmetic satisfactions at the same time are presented in Table 3. When a discrepancy in scores between the patients and surgeon was present, then the lower score was adopted. Two (at 3 months) and two (at 6 months) patients were excluded because of the short follow-up period or completion of total mastectomy. The excellent or good cosmetic results were 82.6% (19/23) after 3 and 6 months. Some skin reactions of the breast were noted in those patients treated with radiation therapy, such as erythema or mild to moderate hyperpigmentation; however, there were no patients with deformities such as skin retraction or contracture of breast during the follow up periods.
DISCUSSION
Breast conservation has become a standard strategy for early breast cancer.(9) However, BCS does not always have an acceptable cosmetic result, and the tumor characteristics, tumor size, location and nipple-tumor distance are factors that affect cosmesis.(10) A small to modest volume of the breast could disturb the postoperative breast contour and symmetry. Many women who undergo breast surgery may be more intolerant of their breast asymmetry and loss of volume than any nipple and scar deformity; therefore, the technique of seroma formation without reconstruction of the defect results in good or excellent cosmesis.(11) We have applied this seroma technique to local excision of benign tumor. However, in the case of large defects owing to large benign tumors or cancers in an effort to obtain clear margins, these defects to fill in with serum may be difficult to maintain the space for a seroma without somewhat deformity. Therefore, we modified this technique for women who underwent partial mastectomy to immediately repair the defect. Reconstruction using absorbable surgical mesh has not been published worldwide as yet, although there were some introductions about this thechnique with satisfactory cosmetic outcome in Japan.(3-6)
The implantation of absorbable surgical meshes always initiates a perifilamentary inflammation, resulting in a chronic foreign body reaction. Therefore, it provides a fibrosis reaction in order to create a resistant lining structure that is sufficient to maintain the space for reactive fluid and granulation without postoperative dimpling or deformity. The ideal prosthesis should favor the development of a dense fibrosis, keep its resistance features with time and be easy to use, yet it should not favor the development of infection. Absorbable surgical mesh, like a polyglactin prostheses, results in the creation of collagen-rich connective tissue.(12,13) Polyglactin loses half of its tensile strength within 2-3 weeks, and is fully absorbed after 3 months.(14,15) Therefore, we evaluated the cosmetic outcome at the time of full absorption of mesh. The tissue support is temporary, and any connective tissue resulting after implantation will remodel over time. The reaction will eventually resolve with no remaining connective tissue. Moreover, the polyglactin 910 mesh is part of the knit construction and its use results in improved intraoperative handling characteristics. Non-absorbable meshes can prolong the resistant lining structure, but it may result in scarring, contracture and distortion of a defect because of the formation of a linear neofascia and the increased risk for late-onset deep prosthetic infection.(16) In reality, the postoperative seroma is somewhat of a complication of mesh insertion.(17) When mesh incorporation is disordered, the result is a fluid collection. Therefore, oxidized regenerated cellulose (Interceed®) interferes with complete attachment of the mesh, and this may promote the formation of seroma.
The volume of seroma is difficult to adjust in accordance with the native breast volume. However, it is possible that the seroma can be aspirated or sterile saline is injected according to the volume until the formation of granulation tissue into the seroma cavity. We performed this procedure without any complications in eight patients. However, long-term cosmetic evaluation should be performed about aspiration of the seroma or injection of saline in future.
Other many methods of autogenous tissue-based reconstruction have been described, but these reconstructions have disadvantages including longer duration of anesthesia, more blood loss, a longer recovery period, risk of necrosis of portions of the transferred tissue, and problems at the donor site.(18-20) Our technique was the simplest; can be easily performed by general surgeons without major complication.




 XML Download
XML Download