

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The term nontuberculous mycobacteria (NTM) generally refers to mycobacteria species other than the Mycobacterium tuberculosis complex and M. leprae12. Although, NTM were first identified in the late 19th century, NTM were not widely recognized as a cause of human disease until the late 1950s3. They have been called by various names including “atypical mycobacteria,” “environmental mycobacteria,” and “mycobacteria other than tuberculosis.” As these names imply, NTM disease have received less attention than tuberculosis (TB) and were considered as a minor disease.
Currently, NTM, which are evidently different from M. tuberculosis, have emerged as important pathogens worldwide45. The incidence and prevalence of NTM diseases are increasing, and their impact on human health has been a topic of interest. The diagnosis and treatment of NTM lung disease remains challenging for clinicians6. Microbiological eradication using the currently available dugs is difficult7. Furthermore, microbiological recurrence is common even after a successful treatment, with a substantially high reinfection rate8910. Therefore, to appropriately prevent and treat NTM diseases, the infection sources and epidemiology of NTM infection should be understood.
Infection Source
1. Environmental source of infection
1) Natural environment
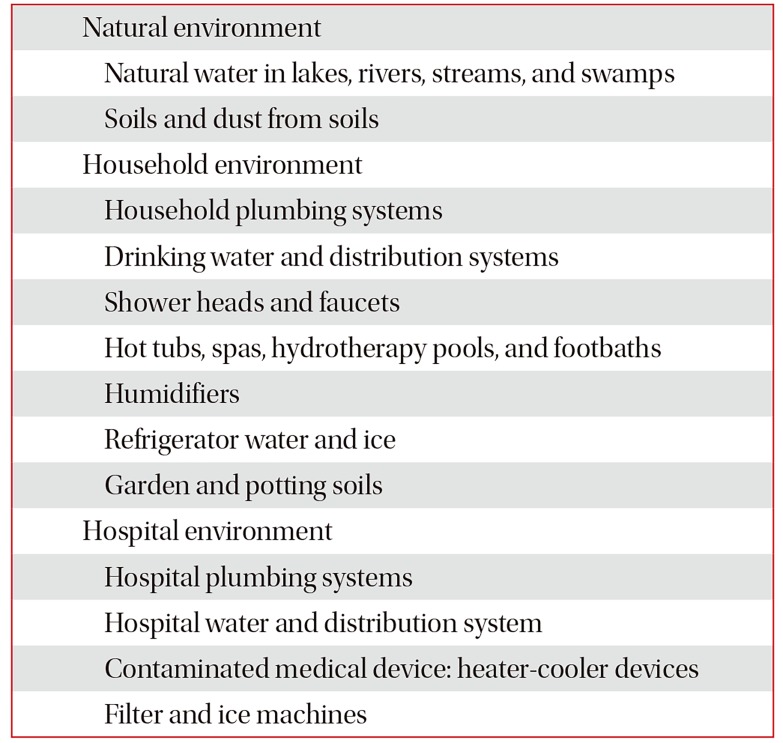
NTM are naturally occurring environmental pathogens. These organisms have been isolated from natural water, including rivers, lakes, swamps, and streams, as well as soil (Table 1)1112. NTM have a lipid-rich outer membrane13, which is a key factor in its survival and proliferation in the natural environment11. As an effect of the lipid-rich outer membrane, these organisms are resistant to acid14, antibiotics15, disinfectants16, and high temperature17. NTM can survive within amoebae18. These pathogens are quite hydrophobic due to their lipid-rich outer membrane and prefer to attach to surfaces and subsequently form biofilms19. NTM are readily aerosolized from natural water and soils due to its surface hydrophobicity20. Naturally occurring aerosolization and subsequent inhalation were the major route of NTM lung disease.
Epidemiology studies have supported the claims that environmental factors could affect the risk for NTM lung disease. In the United States, eight of 55 states were identified as hot spots, with a high incidence of NTM lung disease21. The eight states had a higher mean daily potential evapotranspiration levels and percentages covered by surface water and were more likely to have greater copper and sodium levels in the soil21. Another study on a registry of patients with cystic fibrosis has reported that high saturated vapor pressure is associated with the increased prevalence of NTM lung disease22.
2) Household environment
NTM are widely distributed in human engineered and household environment. Water distribution systems are thought to be a main transmission route from natural surface water reservoirs to the household. NTM have been isolated from drinking water pipelines2324 and water tanks25. The number of NTM increases by 2-fold in a drinking water distribution system, that is, from the treatment plant to the end user26. Cell surface hydrophobicity is a major determinant of the survival and proliferation of NTM in the water distribution systems. These organisms can attach to pipe surfaces and form biofilms, which prevents them from being flushed from the water distribution system. Furthermore, NTM are more resistant to common water disinfectants, such as chlorine, than other microorganisms. Therefore, the use of disinfects kills off competitors and selects NTM.
Household and building plumbing systems provide a stable, nutrient-limited, disinfectant-containing habitat that is ideal for NTM growth and persistence. As NTM are relatively resistant to high temperature, these organisms can survive in water heaters and hot water pipes. Households with water heater temperatures <50°C were more likely to yield NTM (17/20, 85%) than those with water temperature >55°C (6/15, 40%)27. Numerous studies have shown that showerheads and tap water as well as the end points of drinking water distribution systems are the reservoirs of NTM in the household28. Studies that used genotyping have shown that NTM isolates from patients are identical to those in the environment, that is, from shower water2930, showerheads31, and household tap water32.
NTM species have been isolated from house dust33 and soils34. Dry potting soil is a problem because the soil particles can be aerosolized during gardening, and thus, an individual can inhale these particles. DNA fingerprinting methods have shown that NTM isolates from a patient and those from the patient's dried potting and garden soil were identical34.
3) Hospital environment
NTM are also found in hospital environment. Hospital water distribution system may serve as a reservoir of NTM. These organisms contaminate hospital materials and can cause nosocomial outbreaks and pseudo-outbreaks35. Recently, several outbreaks due to M. chimaera have occurred from heatercooler devices used during open-heart surgery3637.
2. Transmission
NTM are generally acquired from the environment via ingestion, inhalation, and dermal contact12. These organisms are everywhere in the human environment and can be readily aerosolized. NTM in household plumbing systems are readily aerosolized from taps, showerheads, and hot tubs. Home humidifiers filled with household water could be a potential generator of a high number of NTM in aerosols12. Use of indoor swimming pools has been associated with NTM lung disease among individuals with cystic fibrosis38. Dusts generated during potting of plants or gardening are also likely sources of NTM infection. Humans are likely to be exposed to NTM in their homes through simple daily activities, such as drinking, showering, or gardening39. The most common routes for pulmonary NTM infection involve the inhalation of aerosols generated by hot tubs and showerheads. Indeed, the global increase in NTM infections may reflect the use of showers rather than bathing40.
1) Human to human transmission
Traditionally, it was believed that human-to-human NTM transmission is not possible. Whole genome sequencing, a new molecular technique, has provided the first genetic evidence of human-to-human transmission of M. abscessus complex among patients with cystic fibrosis4142. Bryant et al.42 have performed a whole genome sequencing analysis of 1,080 clinical isolates of M. abscessus complex obtained from 517 patients from cystic fibrosis centers in seven countries. Results have shown that most M. abscessus complex infections were acquired via human-to-human transmission, potentially via fomites and aerosols.
3. Preventive measure
Strategies that are effective in preventing NTM lung disease are still limited. Vaccines and prophylaxis medications are not available. Unlike TB, preventive therapy is only recommended in patients with advanced human immunodeficiency virus (HIV) disease. A more comprehensive understanding of NTM transmission can help in establishing targeted prophylactic measures. Some preventive measures are recommended to avoid NTM exposure and reduce the number of NTM in the household12. Although the efficacy of these recommendations has not yet been validated via clinical trials, these are still helpful for vulnerable individuals with a high risk for infection.
Preventive measures recommended by experts are the following12: (1) raise hot water temperature to 55°C; (2) use bacteriologic filters (pore size <0.45 mm) on taps and showerheads; (3) utilize well water rather than piped utility supply; (4) clean and disinfect showerheads regularly to remove the biofilm; (5) use showerheads with large holes to reduce mist formation; (6) avoid spas and hot tubs or any water with an aerator; (7) increase bathroom exhaust rate; (8) boil drinking water for 10 minutes to kill NTM; (9) wear mask when gardening; and (10) moisten garden and potting soils.
Epidemiology
1. Incidence and prevalence of NTM
The identification of the epidemiology of NTM lung disease has been challenging because reporting of cases is not mandatory in most countries. Furthermore, diagnosis is difficult because simple isolation of the organism does not necessarily indicate the actual lung disease. Various epidemiological methodologies have been used, including surveillance, population-based studies, analysis of large linked datasets, studies that used laboratory-based convenience samples, and combinations of these approaches43.
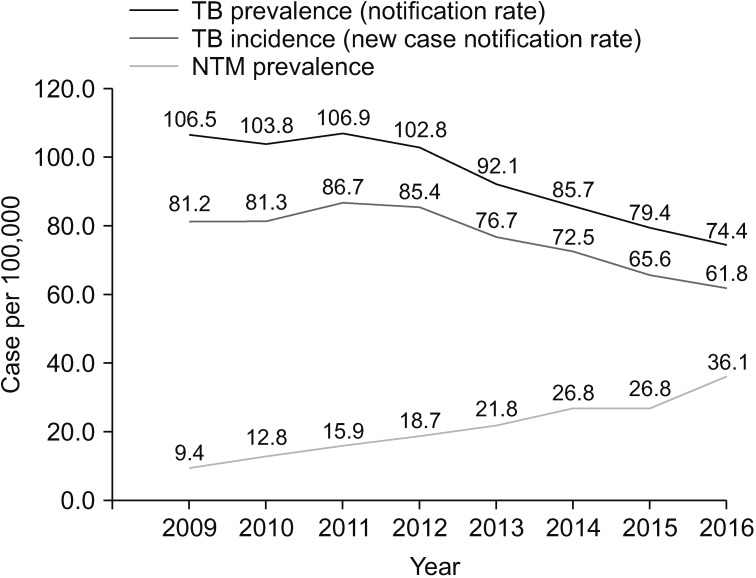
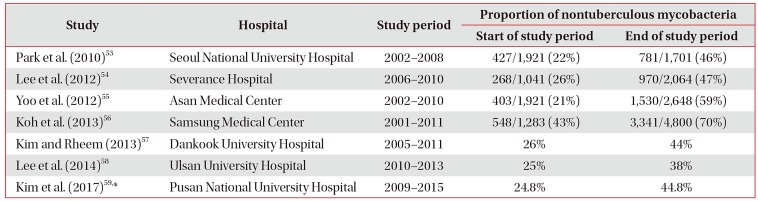
Numerous studies have shown that the incidence and prevalence of NTM lung disease are increasing worldwide44. Population-based data from the United States45, Canada46, the United Kingdom47, and Australia48 have shown that the prevalence of NTM lung disease has been increasing. Large tertiary care facility-based studies in East Asian countries, including Japan49, Taiwan50, and South Korea5152, have also suggested an increasing prevalence of NTM lung disease. In South Korea, no population-based study on the epidemiology of NTM lung disease was conducted. Most studies were conducted in a single institution using laboratory-based convenience samples. Those studies have consistently shown that the proportion of NTM among positive mycobacterial cultures is increasing (Table 2)53545556575859. In a 10-year observational study56, the proportion of NTM among all positive mycobacterial cultures increased from 43% in 2001 to 70% in 2011. Furthermore, the recovery rate of NTM isolates from acid-fast bacilli smear-positive specimens increased from 9% in 2001 to 64% in 2011. This finding has suggested that early differentiation between pulmonary TB and NTM lung disease has become a clinically important issue in South Korea due to the increasing incidence and prevalence of NTM lung disease. Recently, Yoon et al.60 have reported a nationwide increasing trend in the prevalence of NTM disease from 2009 to 2016 in South Korea based on the claims data of the Health Insurance Review and Assessment Service (Figure 1). Interestingly, the increase in the proportion of NTM lung disease may be associated with a simultaneous decrease in the incidence of TB in most countries61, including South Korea60.
2. Species distribution
The distribution of NTM species varies by region and country. This geographical diversity can provide important clues to identify factors associated with the acquisition of NTM infection, such as geographic factors, population density, or host factors. In 2008, the NTM-Network European Trials Group provided species identification data for 20,182 patients from 62 laboratories in 30 countries62. This study has shown that the Mycobacterium avium complex (MAC) predominated in most countries. However, there were important differences in the geographical distribution of M. xenopi, M. kansasii, and other rapid-growing mycobacteria. M. xenopi and M. malmoense were extremely rare in East Asia. However, they are predominantly found in Europe.
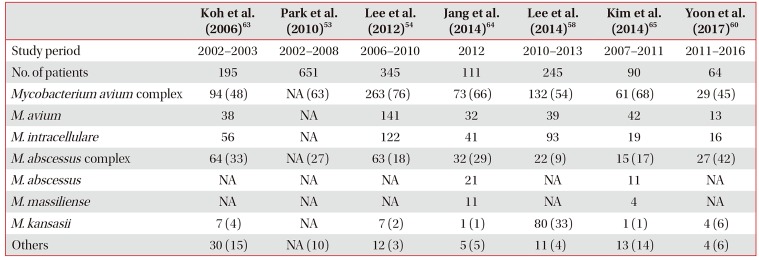
In South Korea, the MAC is the most common organism causing NTM lung disease (Table 3)53545860636465, which is similar to other countries. M. abscessus complex is the second most common organism, whereas M. kansasii does not commonly cause the disease. However, M. kansasii was the second most common NTM species in Ulsan58.
3. Risk factor
Exposure to NTM is quite common. However, NTM disease is relatively rare. This observation suggests that host susceptibility likely plays a key role in the development of NTM lung disease. Patients who develop NTM lung disease usually have some degree of host impairment that make them vulnerable to these infections. NTM lung disease is more prevalent in patients with structural lung disease, such as cystic fibrosis, non-cystic fibrosis bronchiectasis, primary ciliary dyskinesia, chronic obstructive pulmonary disease (COPD), previous TB, and pneumoconiosis66. An immunosuppressed status, which is related to HIV infection, transplantation, or the use of tumor necrosis factor α inhibitor, is also associated with NTM disease66.
However, patients can develop NTM lung disease without any obvious underlying cause. These patients are typically postmenopausal women who have a unique body morphotype6768. Recently, a whole-exome sequencing study has begun to identify genetic predispositions for those patients and found an increased prevalence of genetic mutations that control the function of the immune system, ciliary body, and connective tissues69. This suggests that NTM lung disease is a multigenic disease, which is characterized by a combination of variants across gene categories and environmental exposures that increase susceptibility to infection.
4. Impact on public health
The impact of NTM infection on public health has been underestimated. Generally, NTM have been considered to have a low pathogenicity, and it was believed that these organisms cannot be transmitted from person to person. However, NTM lung disease is associated with a substantially impaired quality of life70, increased morbidity and mortality71, and high medical costs43. Huang et al.72 have shown that patients with COPD who have NTM isolates had a greater decline in lung function and more frequent exacerbation than those with no isolate. Park et al.73 have shown that treatment failure was associated with a substantial decline in lung function in individuals with NTM lung disease. A recent study in Germany have revealed that a higher mortality, direct costs, and indirect costs were observed among patients with NTM lung disease than in matched controls74. Considering the increasing burden of NTM lung disease globally, this disease may soon become a significant health and economic burden.
Conclusion
NTM are generally found not only in the natural but also in the human engineered environment. Remarkable changes in the human environment and lifestyle habits were observed during the past several decades. These changes have made humans more comfortable but also resulted in a more favorable environment for NTM growth. In addition, with the development of medicine, an aging population with multiple comorbidities who are vulnerable to NTM infection is growing rapidly. As a result, the incidence and prevalence of NTM lung disease are increasing worldwide, and this disease is rapidly becoming a major public health problem. NTM lung disease is more difficult to treat and prevent than TB. The elimination of NTM from environmental sources and the destruction of the transmission route are critical issues that must be urgently addressed. Further comprehensive works to investigate the source, transmission route, and epidemiology of NTM are needed to develop new strategies that can prevent and control NTM infection.
 XML Download
XML Download