

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Tuberculous destroyed lung (TDL) results from inadequate treatment of pulmonary tuberculosis and progressive destruction of one or both lungs1. In Korea, TDL is a common cause of pulmonary disability and respiratory failure, and the reported mortality rate is as high as 61%2. A previous study by Ryu et al.3 revealed that TDL was an independent predictor of mortality in patients with acute respiratory failure requiring mechanical ventilation.
Several studies aimed to identify factors predicting mortality in TDL patients24. Park et al.2 evaluated a cohort of 38 TDL patients requiring mechanical ventilation due to acute respiratory failure. The authors found that a positive acid-fast bacilli (AFB) smear or culture was associated with a higher mortality rate, while a higher arterial partial pressure of carbon dioxide (PaCO2) level was associated with increased survival. Ryu et al.4 evaluated 169 patients with TDL and found that extensive lung destruction was the only independent predictor of reduced survival, although only 50 patients (30%) in the cohort had required mechanical ventilation. Acute respiratory failure secondary to TDL is associated with high rates of intensive care unit (ICU) admission, which may burden the limited resources of developing countries56. Early identification of patients with a high risk of mortality, and the selection of individuals who might benefit from ICU care, would therefore facilitate health care planning. However, no scoring system for mortality risk is available for TDL patients on mechanical ventilation.
The aims of the present retrospective study were to (1) develop a mortality prediction model termed the TDL on mechanical Ventilation (TDL-Vent) score using clinical variables obtained at the time of ICU admission; and (2) compare the ability of the TDL-Vent score to predict mortality with that of two widely used illness severity scores.
Materials and methods
1. Study design and cohort
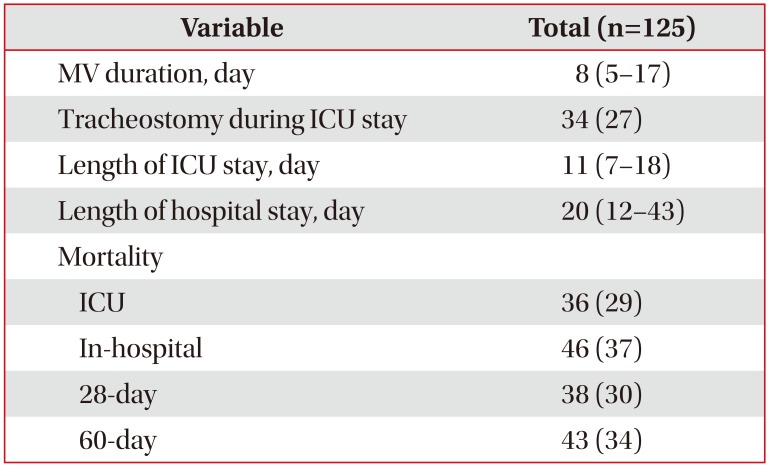
The study was conducted at the Pusan National University Hospital, which is a 1,100-bed university-affiliated hospital in Busan, Korea. Data from consecutive TDL patients who had been admitted to the medical ICU for mechanical ventilation between January 2005 and December 2016 were analyzed. Patients with destroyed lung secondary to other causes were excluded. The primary study outcome was ICU mortality. Secondary outcomes were duration of mechanical ventilation, tracheostomy during ICU stay, length of ICU and total hospital stay, and in-hospital, 28-day, and 60-day mortality. The study protocol was approved by the Institutional Review Board of Pusan National University Hospital (C-1708-028-058). The requirement for informed consent was waived, since the study was retrospective and all patient records were anonymized and de-identified prior to analysis.
2. Data collection and definitions
Baseline demographic and clinical characteristics included age, sex, body mass index, smoking status, comorbidities, and the major diagnosis leading to mechanical ventilation. Disease severity was assessed using the Acute Physiology and Chronic Health Evaluation (APACHE) II score7 and the Sequential Organ Failure Assessment (SOFA) score8. Clinical status within 24 hours of ICU admission (i.e., vasopressor use, renal replacement therapy, and active infections) was also assessed. Laboratory data included complete blood cell count, blood chemistry, and arterial blood gas analysis. Baseline chest X-ray and/or computed tomography scans from the day of ICU admission were reviewed to evaluate the degree of parenchymal lung destruction. To identify potential risk factors for mortality, results from pulmonary function tests conducted within the preceding 12 months, and echocardiography findings and brain natriuretic peptide (BNP) values from the day of ICU admission, were evaluated.
TDL was diagnosed on the basis of a history of present or past pulmonary tuberculosis and radiological evidence of parenchymal lung destruction, lung volume loss, or secondary bronchiectatic changes1. Active infection was defined as the presence in a blood culture or adequate sputum culture, endotracheal aspirate, or bronchoscopy sample of a pneumonia pathogen (bacteria, including tuberculosis; a virus; or a fungus). To evaluate the extent of disease involvement, baseline chest X-rays were graded on a 4-point scale (field score 1–4) using a radiographic scoring method described elsewhere4910. First, four zones were demarcated by dividing each lung into two equal-sized zones (upper and lower) on a frontal radiograph. In each of the four zones, the following scoring system was then applied: (1) 0, no abnormality; (2) 1, when less than 25% of lung parenchyma showed destructive lung lesions; and (3) 2, 3, or 4, respectively, when destroyed lung lesions involved 25%–50%, 50%–75%, or >75% of lung parenchyma. The field score was then calculated as the mean disease involvement of the two lungs. Forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) were expressed as a percentage of the predicted normal values. The FVC and FEV1 values were calculated using Korean equations, which were based on data from a non-smoking population with normal chest radiograph findings and no history of lung disease or symptoms. In these equations, the predicted value is adjusted in accordance with age, sex, height, and weight11. Cor pulmonale was diagnosed on the basis of both clinical and echocardiographic findings12. Echocardiographic signs of cor pulmonale comprised right ventricular (RV) hypertrophy or dilation accompanying high RV systolic pressure (> 35 mm Hg)1213.
3. Statistical analysis
Continuous variables are presented as the median and interquartile range. Categorical variables are presented as percentages. Continuous variables were compared using a Mann–Whitney U test. Categorical variables were compared using a chi-square or Fisher exact test. The optimal cut-off values for potential predictors of ICU mortality were selected using either the median value or locally weighted scatterplot smoothing curves14, as appropriate. Binary logistic regression analysis was performed to identify factors predicting ICU mortality. Variables with p-values of <0.20 in the univariate analysis were included in the multivariate analysis. Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC), and model calibration was assessed using the Hosmer-Lemeshow test. The β coefficient values derived from multiple logistic regression were simplified to natural numbers >0, and the TDL-Vent score was calculated as the sum of these simplified values. To predict 60-day survival, Kaplan-Meier estimates were stratified according to the TDL-Vent score, and curves were compared using the log-rank test. The AUC for the TDL-Vent score predicting ICU mortality was compared with that for the APACHE II score and the SOFA score. Identification of an optimal cut-off value for the score was based on the maximum Youden's index15. All tests of significance were two-tailed, and p-values of <0.05 were considered significant. All analyses were performed using SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA) and MedCalc Statistical Software version 16.8.4 (Med-Calc Software bvba, Ostend, Belgium).
Results
During the study period, 125 patients fulfilled the study inclusion criteria. Of these, 89 (71%) survived ICU admission. The remaining 36 (29%) patients died on the ICU.
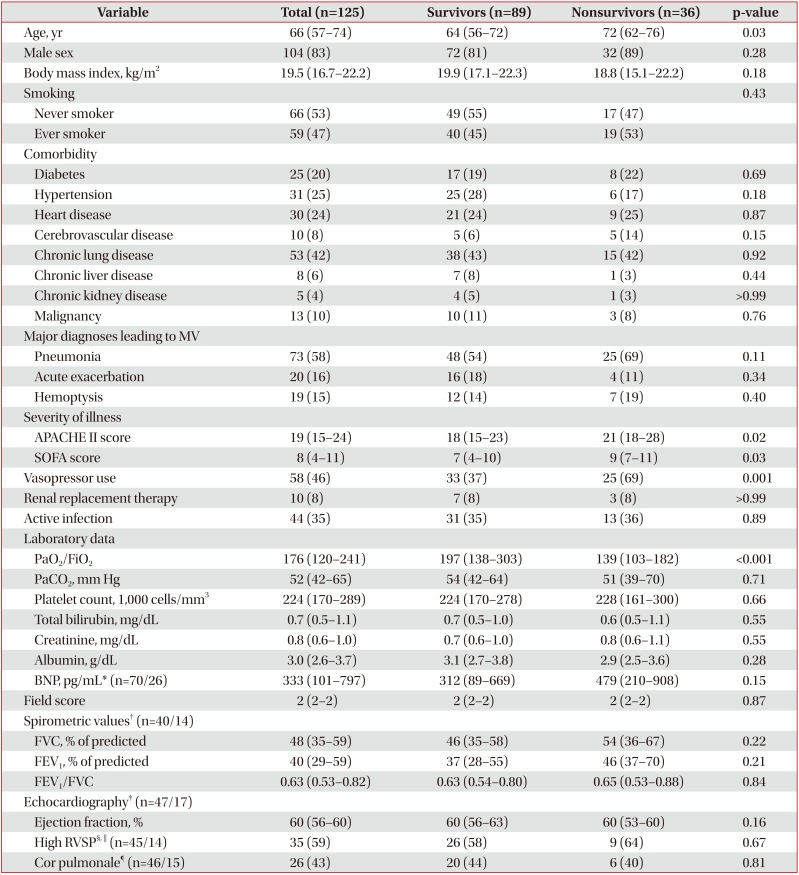
Baseline characteristics of the study cohort are shown in Table 1. Nonsurvivors were older. No significant difference was found between survivors and nonsurvivors in terms of sex, body mass index, smoking status, or comorbidities. Mechanical ventilation was primarily due to pneumonia in 54% (48/89) of survivors and 69% (25/36) of non-survivors (p=0.11). Nonsurvivors had significantly higher APACHE II and SOFA scores and had a higher rate of vasopressor use within 24 hours of ICU admission. Active infection was found in 44 (35%) of the cohort, with no significant difference being found between survivors and non-survivors. The following pathogens were considered to be associated with pneumonia: methicillin-resistant Staphylococcus aureus (n=14); Acinetobacter (n=9); Mycobacterium tuberculosis (n=6); Pseudomonas (n=5); extended-spectrum beta-lactamase-producing organism (n=4); Klebsiella pneumoniae (n=3); Stenotrophomonas (n=3); and Aspergillus species (n=3). The median arterial partial pressure of oxygen (PaO2)/fraction of inspired oxygen (FiO2) ratio was significantly lower in non-survivors. Compared with survivors, non-survivors had numerically lower serum albumin and higher BNP, although the results were not statistically significant. Survivors and non-survivors had similar median field scores. Pulmonary function test results were available for 54 (43%) of the cohort. The median FEV1/FVC ratio was <0.70, and no significant differences between survivors and nonsurvivors were found for median FVC and FEV1. Echocardiographic findings were available for 64 (51%) of the cohort. Cor pulmonale was diagnosed in nearly half of the patients. However, the survivor and non-survivor groups showed no difference in terms of left ventricular systolic function or the proportion of patients with high RV systolic pressure. Clinical outcomes in the cohort are shown in Table 2.
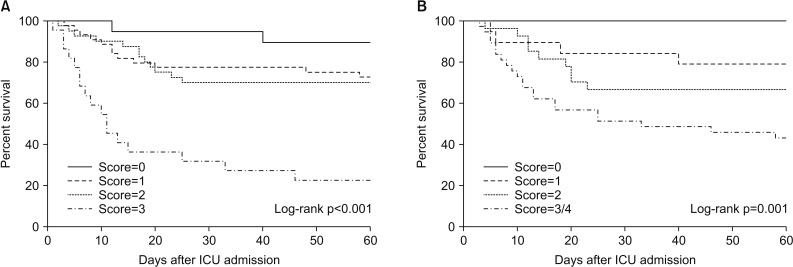
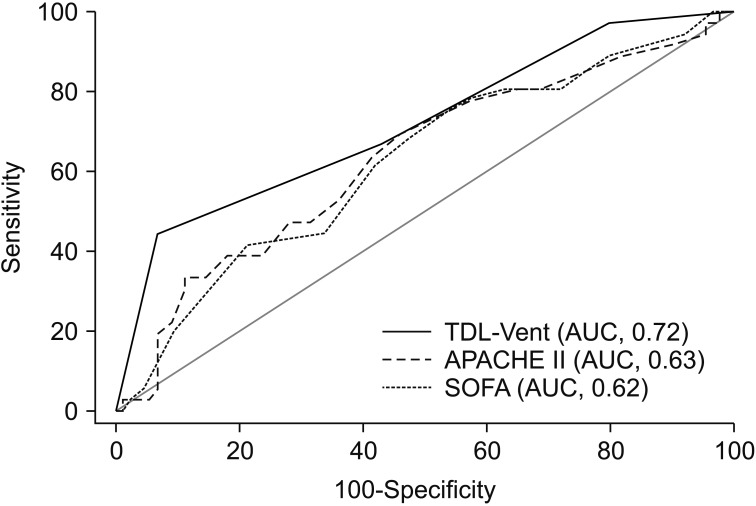
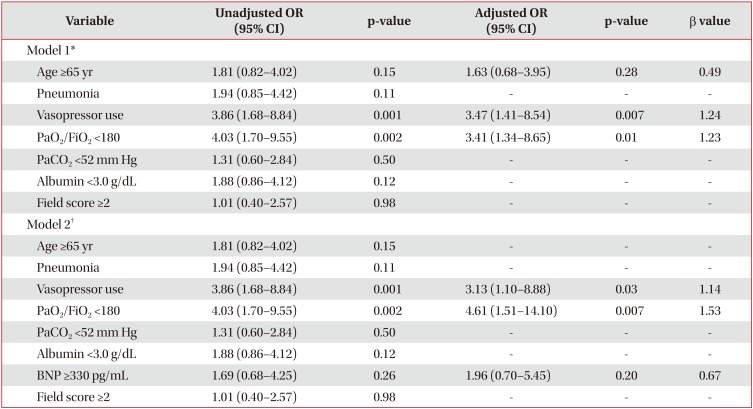
Table 3 shows the results of the univariate and multivariate analyses of risk factors predicting ICU mortality. The following cut-off values were identified via inspection of locally weighted scatterplot smoothing curves: age ≥65 years, PaO2/FiO2 ratio <180, PaCO2 <52 mm Hg, serum albumin <3.0 g/dL, BNP ≥330 pg/mL, and field score ≥2 (Supplementary Figure S1). Based on the β coefficient values observed in model 1, a TDL-Vent score comprising the following factors was proposed: (1) age ≥65 years (+1 point); (2) vasopressor use (+1 point); and (3) PaO2/FiO2 ratio <180 (+1 point). This model had acceptable discrimination (AUC, 0.74) and calibration (Hosmer and Lemeshow chi-square, 14.74; p=0.06). Figure 1A shows the Kaplan-Meier survival curves, as stratified according to the TDL-Vent score. The 60-day mortality rates for scores ranging from 0 to 3 were 11%, 27%, 30%, and 77%, respectively (log-rank test, p<0.001). The AUC of the TDL-Vent score for predicting ICU mortality was 0.72 (95% confidence interval [CI], 0.63–0.80). This was larger than the AUC for the APACHE II score (0.63; 95% CI, 0.54–0.72) and SOFA score (0.62; 95% CI, 0.53–0.71) (Figure 2). The cut-off score for predicting mortality based on the maximum Youden's index was ≥2, with a sensitivity of 44% and a specificity of 93%.
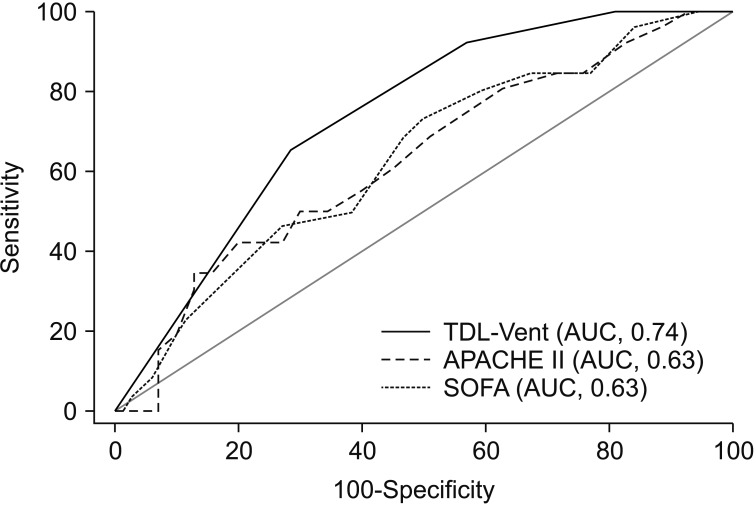
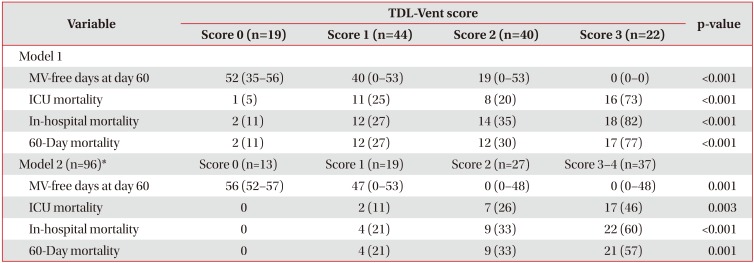
In model 2, BNP was included as an additional variable in the regression model, since pulmonary hypertension is associated with poor prognosis in chronic pulmonary tuberculosis1617 and BNP is a non-invasive marker of pulmonary hypertension1819 (Table 3). In accordance with the β values in this model, the following modified TDL-Vent score was developed: (1) vasopressor use (+1 point); (2) PaO2/FiO2 ratio <180 (+2 points); and (3) BNP ≥330 pg/mL (+1 point). The model had acceptable discrimination (AUC, 0.76) and calibration (Hosmer and Lemeshow chi-square, 54.66; p=0.69). For modified TDL-Vent scores ranging from 0 to ≥3, 60-day mortality rates were 0%, 21%, 33%, and 57%, respectively (log-rank test, p=0.001) (Figure 1B). The AUC of the modified TDL-Vent score for predicting ICU mortality was 0.74 (95% CI, 0.64–0.82) (Figure 3). The cut-off score for predicting mortality was ≥2, with a sensitivity of 65% and a specificity of 71%. Table 4 shows the clinical outcomes of study patients, as stratified according to the TDL-Vent scores from models 1 and 2.
Discussion
The present analyses indicated that age, vasopressor use, PaO2/FiO2 ratio, and BNP were reliable predictors of ICU mortality in TDL patients on mechanical ventilation. These factors were therefore included in the TDL-Vent score. This simple scoring system was more effective than either the APACHE II or the SOFA score in terms of predicting ICU mortality. To our knowledge, the present study is the first to evaluate a mortality risk scoring model for TDL patients on mechanical ventilation.
Several previous investigations of patients with active pulmonary tuberculosis and acute respiratory failure reported high rates of in-hospital mortality. Risk factors associated with mortality vary between studies. However, the most frequently reported risk factors are the requirement for mechanical ventilation, sepsis, organ failure, nosocomial pneumonia, and delayed treatment32021. TDL patients presenting with acute respiratory failure have a poor prognosis. However, few studies have investigated prognostic factors in such patients. Previous studies show that AFB-positive TDL patients have more severe lung destruction and higher mortality rates than AFB-negative patients222, while a higher level of PaCO2 has been associated with increased survival2. Ryu et al.4 found that a high field score was the only predictor of reduced survival, although patients with high field scores showed higher PaCO2. The aforementioned studies investigated small cohorts of mechanically ventilated patients, and their results were inconsistent. The main strength of the present study was its relatively large cohort, which was restricted to patients requiring mechanical ventilation. This enabled the development of an individualized mortality prediction score for this specific population. An interesting and unexpected finding of the present study was the lack of association between the degree of lung destruction, tuberculosis activity, or the level of PaCO2 and increased mortality. Instead, the prognostic factors in the present cohort were age and evidence of organ failure (vasopressor use and PaO2/FiO2 <180), as suggested in other patient populations. These risk factors are consistent with those reported in previous studies of active pulmonary tuberculosis with acute respiratory failure32021, thus supporting the hypothesis that lower physiologic reserve and organ dysfunction, rather than the destroyed lung per se, are better predictors of mortality in mechanically ventilated TDL patients. A low serum albumin level also correlated with mortality in active pulmonary tuberculosis with acute respiratory failure23. In this study, nonsurvivors had lower levels of serum albumin than survivors, although this trend did not reach statistical significance. In the present cohort, the TDL-Vent score (both model 1 and model 2) was superior in terms of discriminating between survivors and non-survivors than either the APACHE II score or the SOFA score. In addition, the score from model 1 showed very high specificity in patients with the highest risk of mortality, thus limiting the possibility of misclassifying a patient as very high risk. This is crucial, as such a classification may result in the decision to withhold or withdraw life support. Lastly, the clinician is able to calculate the TDL-Vent score at the bedside, rather than relying on complicated formulas, smear tests, or chest X-rays.
In patients with TDL, pulmonary hypertension is associated with the severity of lung destruction24. In the present study, high RV systolic pressure and/or cor pulmonale were present in more than 50% of TDL patients who underwent echocardiography, although no contribution to ICU mortality was observed. Meanwhile, non-survivors had a numerically higher BNP. A BNP of ≥330 pg/mL tended to be associated with mortality and was included in the modified TDL-Vent score. These findings are consistent with the results of previous studies192526, which demonstrated that BNP levels were a prognostic factor in patients with idiopathic pulmonary arterial hypertension, idiopathic pulmonary fibrosis, and chronic cor pulmonale. Although BNP values were available for only 96 of the 125 TDL patients, the present results suggest that further studies are warranted to confirm the utility of BNP in terms of predicting mortality in these patients.
Previous reports show that TDL can cause chronic airflow obstruction2427. Proposed mechanisms include a reduction in lung volume, a residual limitation of expiratory flow, and a decrease in ventilatory muscle strength and exercise tolerance secondary to poor nutritional status172829. The present results, in which the median FVC, FEV1, and FEV1/FVC ratio of the cohort were 48% of predicted, 40% of predicted, and 0.63, respectively, are consistent with those of previous studies. However, as did most previous reports, baseline lung function was not associated with ICU mortality.
The present study had several limitations. First, the study was retrospective and conducted at a single center. Although the study enrolled more mechanically ventilated TDL cases than previous studies, the sample size was relatively small and likely to have been responsible for some of the insignificant results. Moreover, the relatively long study period (>10 years) may have introduced selection and information bias. Second, in attempting to identify risk factors for mortality, high specificity was obtained at the expense of lower sensitivity, as a substantial proportion of patients who died did not have a high TDL-Vent score. Third, a substantial number of patients were excluded from the echocardiography and pulmonary function analyses due to missing data. The inclusion of these patients might have influenced the study results. Lastly, the present study provided a development set only, and the results therefore require independent validation.
In conclusion, the TDL-Vent score is a simple model that may facilitate the prediction of mortality in TDL patients on mechanical ventilation. Prospective validation of the TDL-Vent score in a larger cohort is warranted.
 XML Download
XML Download