

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Tuberculosis (TB) remains to be one of the world's deadliest transmissible diseases1. In 2015, an estimated 10.4 million people developed active TB and 1.8 million died of it1. The most widely accepted measure of treatment response in patients with pulmonary TB is the disappearance of acid-fast bacilli (AFB) from sputum smear and culture2. Non-conversion of sputum smear at the end of the second month of treatment has been documented to be associated with unfavorable outcomes, more specifically with failure and relapse within 2 years of follow up34.
Various factors that correspond to heavy initial bacillary load (higher sputum smear and culture grading at diagnosis, shorter time to detection (TTD) of Mycobacterium tuberculosis on liquid cultures, radiologically extensive disease, cavitation) have been associated with sputum smear and culture non-conversion at the end of the second month of TB treatment 5678. Among other factors, increasing age, male sex, smoking, diabetes mellitus (DM), malnutrition, anemia, and thrombocytosis have also been linked with persistent sputum positivity before the end of second month of treatment5910.
Knowledge of these factors can be helpful in predicting which patients will remain infectious for a longer period of time and will have worse outcomes. Therefore, taking this information into account can assist in improving TB control. This information could also have an impact on evaluation of the effectiveness of new drugs.
Materials and Methods
This study was performed by retrospective analysis of the database of the Vilnius University Hospital Santariskiu Klinikos, Adult Tuberculosis Unit. Data on demographic, clinical, radiological and bacteriological characteristics of all patients with newly diagnosed culture-positive drug-susceptible pulmonary TB admitted between September 2015 and September 2016 were reviewed.
Culture-negative and human immunodeficiency virus (HIV)-positive patients were excluded from the study. Patients with drug resistant strains, TB relapse, defaulted patients and those who did not finish the intensive phase of the treatment were also excluded. All patients were hospitalized for a period of at least 2 months and received the intensive phase treatment as inpatients. Eighty-seven patients were included for the analysis (Table 1).
Baseline assessment consisted of three sputum samples from each patient, collected over a period of 1 week. All samples were tested in local TB laboratory for AFB smear microscopy and cultures on solid and liquid media. For AFB positive samples, Xpert MTB/RIF test was performed to detect rifampin-resistant strains. If patients were smear-negative or unable to expectorate sputum, fiberoptic bronchoscopy with bronchoalveolar lavage (BAL) was performed. BAL fluid was tested for microscopy, solid and liquid cultures and Xpert MTB/RIF test. Posteroanterior (PA) and lateral chest X-rays were performed for all patients before treatment and repeated at the end of the second month of treatment. The extent of disease was evaluated as number of lobes affected and presence of cavitation. Laboratory blood tests, including C-reactive protein (CRP), whole blood count (WBC), hemoglobin (Hb), platelet count (PLT), and erythrocyte sedimentation rate (ESR) were performed initially and at the end of the second month of treatment.
All patients received weight-based daily anti-TB therapy and the medical staff observed each drug administration according with the guidelines of the National Tuberculosis Treatment Program, which is based on the directly observed treatment, short-course strategy as per World Health Organization (WHO) guidelines for the management of TB patients13.
Intensive phase treatment consisted of rifampicin (RMP, 600 mg), isoniazid (INH, 300 mg), pyrazinamide (PZA 2,000 mg), and ethambutol (EMB, 1,200 mg). Doses were reduced if patient weighed less that 50 kg or was older than 70 years of age. The reduced doses were as follows: RMP 450 mg, INH 300 mg, PZA 1,500 mg, and EMB 800 mg. The intensive phase of treatment was prolonged to 3 months if smear conversion had not occurred at the end of the second month of treatment. The continuation phase of treatment consisted of RMP and INH. Dosing was equivalent to that of the intensive phase treatment.
Two sputum samples were obtained from each patient at the end of the second month of treatment: one sample was tested for smear microscopy and another one, for microscopy and solid culture. Treatment outcomes were defined as per WHO recommendations14. Sputum positivity after 2 months of treatment was defined as positive sputum smear sample or positive culture if smear sample was negative, collected at the end of second month of treatment.
All respiratory specimens (sputum and BAL) were processed using internationally established standard methods and used for smear preparation and culturing using liquid (Bactec MGIT 960; Becton Dickinson, Sparks, MD, USA) and solid Löwenstein-Jensen (LJ) media. LJ cultures were incubated for 8 weeks at 37℃ and checked weekly for visual growth. Positive cultures were verified on the base of colony morphology and/or Ziehl-Neelsen staining. On liquid media time to positivity, defined as the number of days and hours between sample inoculation and detection of mycobacterial growth, was recorded; specimens displaying no growth on day 42 were considered as negative.
Microscopy and growth on solid media grading was performed on all specimens according to International Union Against Tuberculosis and Lung Disease/WHO recommendations15.
The association of various factors with persistent sputum positivity at the end of 2 months of treatment was analyzed. Data processing and analysis were performed using IBM SPSS version 20 (IBM Corp., Armonk, NY, USA) and Microsoft Excel 2010 software. Univariate analysis was performed in search for differences between independent groups. Continuous variables were inspected for normal distribution by Kolmogorov-Smirnov statistic and compared by the parametric Student's t-test when normally distributed or by the nonparametric Mann-Whitney or Wilcoxon test for non-normally distributed variables. The Dependent t-test was used to compare the means of two continuous variables for a single group. The Pearson chi-square Test was used for categorical variables. A probability of 0.05 was considered significant. The odds ratios (OR) and 95% confidence intervals were calculated. Logistic regression analysis was performed to identify which of the above factors were independently and significantly associated with the dependent variable. The Spearman's and Kendall's tau-b correlation was applied to study the correlation of various factors associated with persistent sputum positivity.
The study was approved by the regional bioethics committee. As data collection were retrospective, informed consent was not obtained.
Results
A total of 255 eligible patients were screened and 168 patients were excluded for the following reasons: drug resistant TB (n=58), previously treated (n=46), did not finish the intensive phase of treatment in hospital (n=39, of whom 13 died), bacteriologically unconfirmed TB (n=12), culture-negative TB (n=9), non-pulmonary TB (n=3), and HIV infection (n=1).
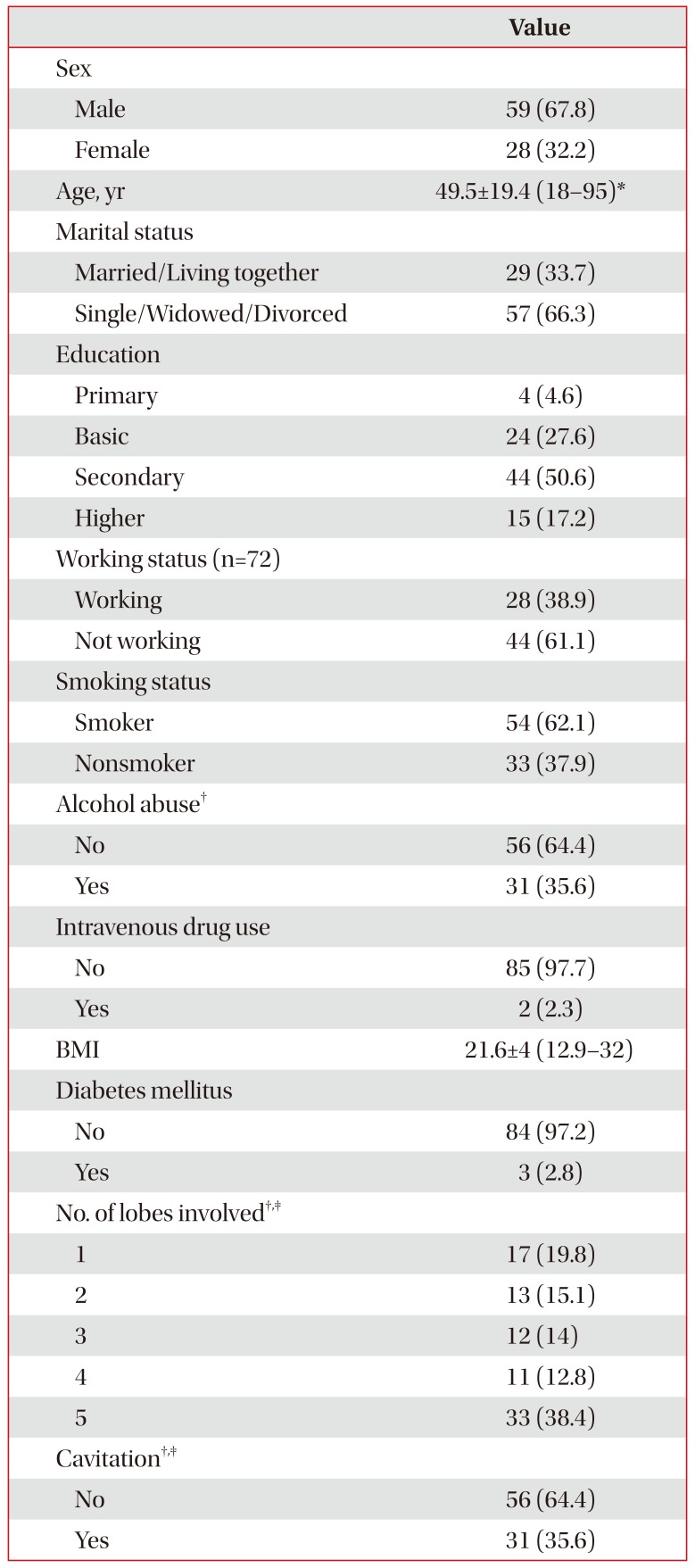
The remaining 87 patients were included for the analysis. The majority (n=59, 67.8%) of patients were male and the mean age (±standard deviation) was 49.5 years (±19.4). Overall the patients had a normal body weight, with a mean body mass index (BMI) of 21.6 (±4). Most of the patients had at least secondary education (n=59, 67.8%), were single, widowed or divorced (n=57, 66.3%), current tobacco smokers (n=54, 62.1%), and alcohol consumers (n=53, 60.9% of which 31 [58.4%] were alcohol abusers). The majority of 72 working age patients were unemployed (n=44, 61.1%). Parenchymal disease was extensive with more than two lobes affected on pretreatment chest X-rays in 56 patients (64.4%) and the same number of patients had cavities on chest X-rays (n=56, 64.4%).
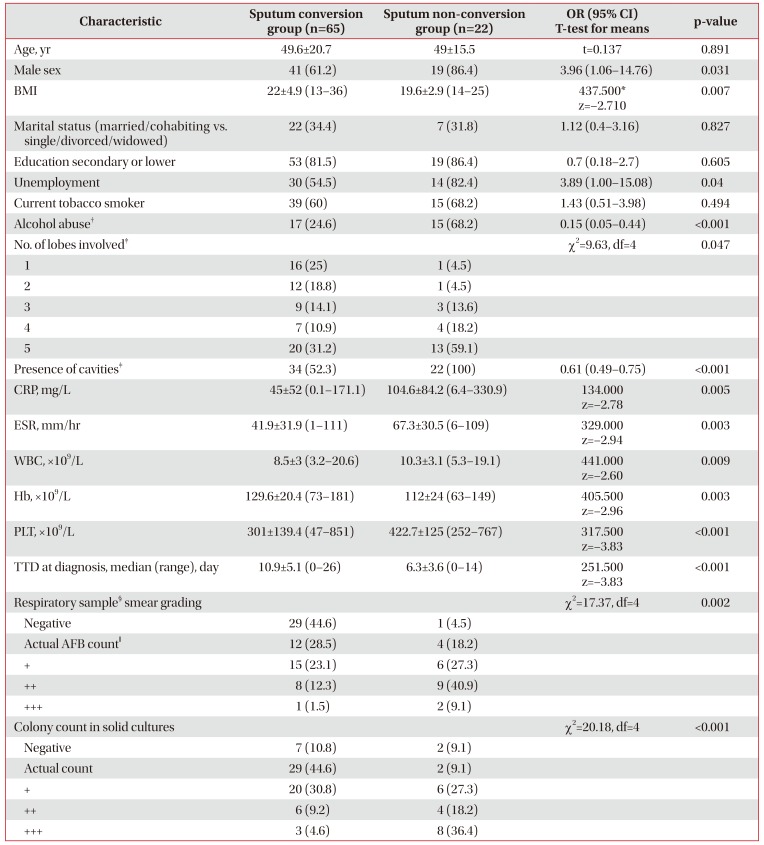
Twenty-two patients (25.3%) remained sputum smear and/or culture positive at the end of the second month of TB treatment. Various demographic, clinical and radiological characteristics were found to be associated with persistent sputum positivity (Table 2). A 100% of non-converted patients had cavities detected on pre-treatment chest X-rays. Patients treated with reduced doses of medication did not have a statistically different outcome after 2 months of treatment (p=0.819).
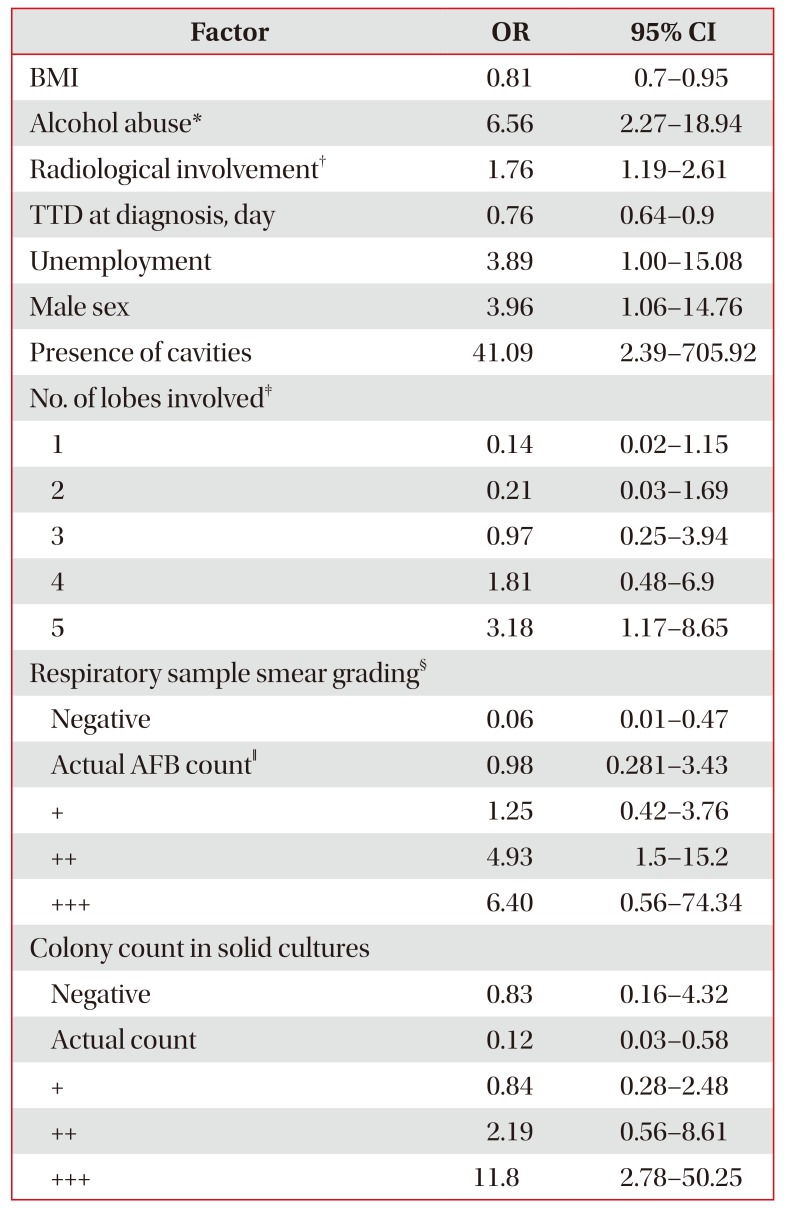
In the logistic regression analysis, it was found that male sex, BMI, alcohol abuse, radiological involvement, presence of cavities, respiratory sample smear grading, TTD at diagnosis and colony count in solid cultures were independently significant factors (Table 3). Although all analyzed blood tests (CRP, ESR, WBC, Hb, and PLT) were also found to be independently statistically significant, ORs in this group were all nearing 1. Higher TTD at diagnosis lowered the risk of persistent sputum positivity by 24.3%. Age, smoking, unemployed status, and reduced doses of medications were not found to be significantly associated with persistent sputum positivity. Additionally, patients with negative smear microscopy and the lowest possible count of colonies (actual colony count) detected in solid cultures before treatment were respectively 17 and 8 times more likely to achieve sputum conversion by the end of the second month of TB treatment.
Discussion
In this study, we investigated the factors influencing sputum conversion at the end of the second month of newly diagnosed, drug-susceptible pulmonary TB treatment. Our study had strict exclusion criteria resulting in homogenous study population. All cases of TB were culture-confirmed and patients were treated in hospital for all study period.
Twenty-two patients (25.3%) remained sputum smear and/or culture positive at the end of the second month of TB treatment. This number initially appears to be higher in comparison with other studies5610. However, in studies that assess culture negativity for sputum conversion, the non-conversion group percentage can be notably higher1617. It is worth noting that almost two-thirds (64.4%) of the patients had radiologically extensive disease, defined as more than two lobes affected on pre-treatment chest X-rays.
We found male sex, BMI, alcohol abuse, radiological involvement (higher number of lobes affected), presence of cavities, shorter TTD, higher respiratory sample smear grading and higher colony count in solid cultures to be independently associated with persistent sputum positivity. These findings are consistent with other studies791618. In contrast with other studies91019, laboratory blood tests (CRP, ESR, WBC, Hb, and PLT), although were found to be statistically significant, all had OR's nearing 1. CRP, ESR, WBC, and PLT are markers of systemic inflammation. All of these markers and the presence of anemia correspond to the severity of the disease but may vary significantly between patients.
Heavy initial bacillary load has been documented as an important risk factor of delay in sputum smear conversion at the end of intensive phase of TB treatment410161720. Our study shows that higher smear and culture grading, as well as shorter TTD were all significantly associated with persistent sputum positivity.
Radiological factors associated with high bacillary load (radiologically extensive disease, cavitation) were also found to be associated with persistent sputum positivity.
Cavitation is frequently associated with delayed sputum conversion7913141521. In our study 64.4% of all patients had cavities detected on pretreatment chest X-rays and this finding correlates with other studies718. Interestingly, patients with persistent sputum positivity at the end of the second month of TB treatment displayed cavitation unanimously.
The most accurate extent of TB lesions is depicted from evaluation of chest computed tomography scans. However, most of our study patients did not underwent this procedure. We performed PA and lateral chest X-rays for all patients for baseline evaluation which enabled an accurate evaluation of numbers of lobes affected but evaluation of small cavities may be underestimated.
TTD has been shown to be inversely related to the logarithm of inoculum size and has been proposed as a surrogate marker for evaluation of bacillary load18. Shorter TTD has been associated with delayed smear conversion in several studies71618. Our study adds to the data on this emerging marker.
We could not evaluate DM as a risk factor since only three patients had DM in our study. This number is relatively low, compared to previous studies69.
Alcohol consumption is often under-reported and under-reporting is greater among persons who consume more alcohol22. It is therefore probable, that alcohol abuse was under-reported in our study. High doses of alcohol consumption can directly suppress a wide range of immune responses and are associated with an increased incidence of a number of infectious diseases23. Alcohol abuse was found to be associated with TB relapse, default and death242526. However, it was not associated with persistent sputum positivity in several studies2728. We found alcohol abuse to be a serious risk factor for persistent sputum positivity (OR, 6.56; p=0.001). This variation may arise because of the cultural differences, as well as differences in alcohol consumption and reporting techniques in different countries.
Medication doses were reduced equally for all patients aged 70 years or more and all patients with body weight less than 50 kg in our study. No statistical difference was found in treatment response after 2 months between patients treated with reduced doses of medication and those who received full doses of treatment (p=0.821). There was also no serious drug related adverse events reported during study period.
Studies have shown various correlations between sputum smear and culture during TB treatment491720. If a patient is receiving treatment, positive smear test for AFB may show non-viable bacilli, which can be dead or unable to replicate. In such case, it is proposed that only negative cultures should be assessed for sputum sterilization. This method, however, is costly and therefore not viable in limited resource settings. It would also take too long for relevance in clinical practice. In our study, 11 of 22 patients (50%) with persistent sputum positivity at the end of the second month of treatment were smear positive, but culture negative. There were also two patients who were smear negative, but culture positive after 2 months of treatment. This discrepancy may be partially explained by sputum collection design in our study. Two sputum samples we collected at the end of second month of treatment: one only for microscopy and second one for microscopy and culture. Since most patients have trouble to expectorate after two months of treatment, sputum samples could have been of different quality.
Delayed sputum conversion prolongs the period of infectiousness and predicts higher relapse and failure rates718. Information about factors delaying sputum conversion is therefore important for public health. Our findings may assist in deciding which patients require to be isolated for a longer period of time. Since a lot of patients remain infectious even after two months of standard TB treatment, we propose that countries that use 2 weeks of isolation for most patients (e.g., United Kingdom) should re-evaluate this policy29. Also, patients with risk factors for persistent sputum positivity should require more thorough evaluation of sputum collection before the end of second month of treatment. Closer and longer period of observation for these patients should be recommended to prevent default and early relapse. Knowledge of factors delaying sputum conversion might also assist in clinical trials for new drugs and/or their combinations.
The limitation to this study is that it has a retrospective design and a relatively low number of patients. Study population, however, reflects most of the patients with a new-case pulmonary TB in Lithuania.
Factors associated with heavy bacillary load (radiologically extensive disease, presence of cavities, higher respiratory sample smear grading and colony count in solid culture, shorter TTD), as well as male sex, alcohol abuse and lower BMI were found to be independently associated with persistent sputum positivity at the end of the second month of TB treatment. These factors should be sought when distinguishing which patients will remain infectious for a longer period of time and possibly have worse outcomes.
 XML Download
XML Download