

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Fetal adenocarcinoma is a very rare subtype of malignant lung cancer. It was first described by Kradin et al.1 as one subtype of pulmonary blastoma resembling the epithelial component of the fetal lung without a sarcomatous component. The updated World Health Organization (WHO) classification lists four rare variants of invasive adenocarcinoma of the lung: invasive mucinous adenocarcinoma (formerly known as mucinous bronchioloalveolar carcinoma), colloid adenocarcinoma, fetal adenocarcinoma, and enteric adenocarcinoma2. Although an estimate of the incidence of fetal adenocarcinoma in Korea is unavailable, it is reported to be the cause of approximately 0.1% of all primary lung cancers2. Moreover, most of the reported cases in Korea were diagnosed in early stages, which enabled complete resection of the tumor3,4.
Histologically, fetal adenocarcinoma is generally well-differentiated (low grade) and consists of columnar, glycogen-rich cells growing in squamoid morules2. It is a low-grade malignancy and mortality is only 15%5. Although most fetal adenocarcinomas reported to date were operable2,6,7, we describe a case of inoperable advanced fetal adenocarcinoma extending to the proximal airway causing dyspnea and multiple lymph node metastasis. We treated this case with endobronchial stent insertion via an endoscopic procedure followed by concurrent chemoradiation therapy, which was successful in improving the patient's symptoms.
Case Report
A 48-year-old man was referred to our hospital due to a lung mass of unknown origin. The patient had a 60 pack-year smoking history. Prior to admission, the patient visited an outside hospital with a one-month history of dyspnea, cough and sputum. Chest imaging studies demonstrated a lung mass (initial size, 7.7×6.4 cm) at the right mediastinal border with deviation of the trachea. After placing an endobronchial stent in the left main bronchus from the carina, the patient was transferred to our hospital.
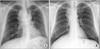
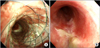
Chest X-ray (Figure 1A) showed a large mass in the right paratracheal area, causing tracheal deviation to the left with mild bronchopneumonia in the right lower lobe. The stent in the left main bronchus remained patent. Computed tomography (CT) revealed a 7.7×6.4 cm lobulated, heterogeneous enhancing mass abutting the trachea, carina, and both main bronchi, as well as multiple enlarged lymph nodes in the subclavian, right hilar, subcarinal, upper and lower paratracheal areas (Figure 2A). A metallic stent was placed in the left main bronchus and irregular narrowing of the right main bronchial wall was also observed. Flexible bronchoscopy (FBS) showed the placement of a stent from the carina to the left main bronchus, extending to the left second carina (Figure 3A). The left upper and lower bronchi appeared normal. A white fungating mass obstructing the right main bronchus and a pin-point opening due to a mass-like lesion were detected.
Thoracoscopic biopsy of the mediastinal lymph node was performed. Gross examination revealed a single, 2 cm, white, well-defined mass that bled easily. Histopathologically, the mass was composed of numerous glands showing an endometrioid morphology, occasional squamoid morules (×400), and relatively clear cytoplasm (Figure 4). Based on these histopathological findings, we finalized the diagnosis as fetal adenocarcinoma.
Due to the locally advanced state of the lung cancer in this case, concurrent chemoradiation therapy (Tomo-Helical; 5,500 cGy) was administered. Treatment was comprised of 25 mg/m2 docetaxel weekly for six weeks with concomitant radiation therapy; the patient completed the planned treatment regimen. Repeat CT performed at a 1-month follow-up visit (Figure 2B) showed the mass in the right paratracheal area had decreased in size (5.8 cm decreased to 4.6 cm), indicating a stable disease. Additional follow-up chest CT and FBS were scheduled at 3-month intervals. On follow-up studies at 4 months, positron emission tomography-CT showed significantly decreased size and activity (5.5×4.6 cm to 4.5×3.4 cm) of the mediastinal mass, which was considered a favorable response to the treatment, and no other newly developed hypermetabolic foci to suggest distant metastasis were seen. Bronchoscopy (Figure 3B) showed relief of the airway obstruction of the right and left main bronchi, with increased ease of passing the scope. Compared with the previous chest X-ray (Figure 1A), the airway obstruction and tracheal deviation were improved (Figure 1B). We were able to remove the stent from the left main bronchus. Previous symptoms of dyspnea and cough were also improved. A further partial response was noted on the 7-month follow-up studies, and another CT follow-up is planned in 3 months.
Discussion
Fetal adenocarcinoma was formerly classified as a subtype of pulmonary blastoma termed well-differentiated fetal adenocarcinoma (WDFA)6. Because WDFA is characterized by a monophasic pattern consisting of an epithelial component alone, distinct from other pulmonary blastoma subtypes, the WHO in 1999 removed WDFA tumors from the pulmonary blastoma category and classified them as a variant of adenocarcinoma7.
Our understanding of fetal adenocarcinoma is derived from case reports or small case series. It is estimated that approximately 0.1% of lung neoplasms are fetal adenocarcinomas. It is generally found in young patients with a unimodal age peak in the third decade, has a slight female predominance, and is most commonly early stage disease at diagnosis with no lymph node involvement. It is generally treated and frequently cured by surgical resection, and has better survival compared with similarly staged and treated adenocarcinoma of the lung2,7. According to a study of 25 cases of fetal adenocarcinoma by Sato et al.7, cases in which the tumor was detected on a chest radiograph as part of routine health maintenance accounted for 76% of the total. The tumor size at resection was comparatively small, with a median size of 3.5 cm (range, 1.4-12.0 cm). The tumors tended to be localized in the right lung, especially in the upper lobe. Among the 24 cases in which the pathological stage was reported, there were two cases with N1 lymph node metastasis at the time of resection, and only one had a distant metastasis to the eye at the time of diagnosis. There were no N2-positive cases, and the vast majority of cases were N0 (22 cases, 88%)7,8.
Contrasting with other cases, we described a 48-year-old male patient with locally advanced lung cancer in this paper. The lung mass was found by chest imaging performed due to the patient's symptoms rather than through routine health maintenance screening. Operative intervention was impossible because of the degree of local advancement and the presence of multiple lymph node involvement and tracheal deviation.
The standard treatment for fetal adenocarcinoma is surgical resection. However, there have been no established treatment guidelines for inoperable cases up to this point. Van Loo et al.6 previously reported that among 63 cases of pulmonary blastoma, 9 were classified as WDFA. Of these nine WDFA cases, three were beyond T3 stage and underwent postoperative chemotherapy or radiation therapy. However, the benefit of this therapy was unclear6. In our case, after ameliorating the airway obstruction with stent insertion via bronchoscopy, concurrent chemoradiation therapy (CCRT) was performed with docetaxel for inoperable fetal adenocarcinoma. A partial response was observed on follow-up chest CT at 1 month and 4 months after treatment, and follow-up chest CT and FBS were scheduled at 3-month intervals.
Patients with fetal adenocarcinoma tend to have a better prognosis than those with other types of adenocarcinoma. Surgical resection is the treatment of choice for operable cases; however, no treatment guidelines have been established for inoperable cases. We encountered an inoperable case of fetal adenocarcinoma of the lung, and a favorable response was achieved with docetaxel-based CCRT. Therefore, surgical resection following tumor down-staging with neo-adjuvant chemotherapy or radiation therapy is one option for effective treatment.


 XML Download
XML Download