

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cephalometric images have become a vital part of orthodontics, since their introduction by Broadbent1 in 1931. Both posteroanterior (PA) cephalograms and lateral (LA) cephalograms are needed for assessment of lateral problems such as facial asymmetry.2345 Precise identification of landmarks using these cephalograms is important for appropriate diagnosis and planning of treatment.
El-Mangoury et al.6 analyzed identification errors at several landmarks and reported that each landmark has its own characteristic error pattern. Major et al.7 analyzed identification errors at 52 landmarks on 33 dry skulls and 25 patients in the vertical and horizontal directions, and reported more intra-observer errors than inter-observer errors. Similarly, Athanasiou et al.8 investigated landmark identification errors at 34 landmarks on 30 PA cephalograms and reported various error patterns between these landmarks.
There have been a number of attempts to reduce landmark identification errors. Legrell et al.9 attached markers on the skin before obtaining LA cephalograms in order to reduce errors in identification of the gonion and antegonion on PA cephalograms, and reported that the errors were reduced when this method was used. However, the landmarks used in that study only included the mandibular angles and newer methods to reduce identification errors in other areas of the face are needed.
Biplanar radiography101112 is used to acquire PA and LA projections perpendicular to each other, and has long been suggested as a way of overcoming the shortcomings of two-dimensional radiographs. However, this technique requires two cephalometric imaging devices and was not widely used because of spatial limitations. Kim and Hwang13 developed a head posture aligner (HPA) that uses the principle of fluid level sensors to reproduce uniform vertical head rotations. This device has enabled the acquisition of LA and PA cephalograms that are perpendicular to each other in an identical head position, even while using a radiographic device with a single cassette and radiation source. Obtaining LA and PA cephalograms in the clinical setting became easier with the advent of biplanar radiography. This method could potentially reduce landmark identification errors. In the present study, the LA and PA cephalograms were obtained using an HPA and the principles of biplanar radiography. The purpose of the present study was to investigate whether the use of LA cephalograms can reduce errors in landmark identification on PA cephalograms.
MATERIALS AND METHODS
The study included 32 patients aged 20 years or older, and without severe dentofacial deformities. The study was approved by the Institutional Review Board of Chonnam National University Dental Hospital, Gwangju, Korea (CNUDH-2016-020), and the informed consent was obtained from all participants. The PA and LA cephalograms were obtained for each patient using a Cranex 3+ imaging system (Soredex Corp., Helsinki, Finland). An HPA was used to obtain PA and LA cephalograms for the same head position (Figure 1). The distance between the patient and the radiation source was 150 cm, and the target film distance was 15 cm. For the PA cephalograms, the tube current was set at 7 to 8 mA, the tube voltage at 80 kVp, and the exposure duration at 1.2 to 1.7 seconds. For the LA cephalograms, the tube current was set at 10 mA, the tube voltage at 75 to 85 kVp, and the exposure duration at 1.6 seconds.
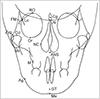
Sixteen landmarks were used in our investigation of PA landmark errors, with or without the use of LA cephalograms. They comprised the crista galli (Cg), nasion (N), anterior nasal spine (ANS), genial tubercle (GT), and menton (Me) for the median landmarks, and the roof of the orbit (RO), latero-orbitale (Lo), frontomalar suture point (FM), zygomatic suture point (Z), orbitale (Or), zygoma (Zyg), condylion (Cd), nasal cavity (NC), mastoidale (Ms), molar point (M), and antegonion (Ag) for the bilateral landmarks. Landmarks on the right side were used for the landmarks that were bilateral (Figure 2).
The examinations were performed by five graduate students of the dental college who had attended lectures on orthodontics and knew the definitions of the landmarks listed in Table 1. Landmarks were identified on each photograph using CS5 Photoshop (Adobe Systems Inc., San Jose, CA, USA). The landmarks on the PA cephalograms were displayed on a 23-inch (16:9) monitor with a resolution of 1,920 × 1,080 (SyncMaster S23A350H; Samsung, Seoul, Korea). The examiners could enlarge the images when necessary. When LA cephalograms had to be used, both LA and PA cephalograms were displayed on the monitor so that the examiner could refer to the LA cephalograms while identifying landmarks on the PA cephalograms.
In this study, landmarks were identified twice on 32 PA cephalograms—once with the help of LA cephalograms, and once without it. The 32 images were initially divided into two groups to avoid the possibility of a rehearsal effect contributing to a decrease in identification errors after review of a large number of cephalograms. The 16 images in each group were further subdivided so that they could be analyzed with and without LA cephalograms (n = 8 each). Two weeks later, the landmarks were identified again with LA cephalograms for the PA cephalograms on which landmarks had been identified without LA cephalograms, and without LA cephalograms for those on which landmarks had been identified with LA cephalograms. Two weeks after identifying the landmarks on the first 16 cephalograms, the same step was repeated for the remaining 16 cephalograms. The five examiners identified landmarks in a total of four sessions every two weeks (Figure 3).
V-ceph 7.0 (Osstem, Seoul, Korea) was used to output the x and y coordinates of the landmarks located on each PA images. The mean of the sets of x and y coordinates recorded by the five examiners for each landmark was used as the reference point. The reference point was referred to the best estimate in the previous study of Leonardi et al.14 A landmark identification error was defined as a difference between the location of the landmark and the reference point.14 The vertical and horizontal components of the difference were calculated to clarify the patterns of error more precisely.
Statistical analysis
An identification error was defined as the mean error for each landmark between the five examiners. The mean and standard deviation were calculated for each landmark location found with PA cephalograms alone and for each location identified using both LA and PA cephalograms. These values were tested for statistical significance using the paired t-test. Each error in identification was subdivided into horizontal and vertical components to understand the patterns of error and tested for statistical significance using the paired t-test. To assess method error using Dahlberg's formula as recommended by Battagel,15 10 cephalograms were randomly selected and the reference point for all the landmarks were reassessed after the original recordings. Dahlberg's values demonstrated that random error ranged from 0.21 to 0.54 mm for landmark identification. Additionally, intra-examiner error was assessed by calculating the intraclass correlation coefficient (ICC) and the ICC measurement showed a mean of 0.826 (ICC = 0.74 – 0.91). All statistical analyses were performed using IBM SPSS Statistics version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Landmark identification errors on PA cephalograms
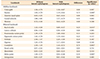
Errors of a wide range of magnitude were found for the 16 landmarks identified on PA cephalograms without LA cephalograms. While these errors were relatively small for ANS, Me, Ms, and Ag, large errors were noted for N and GT landmarks (1.92 mm and 1.88 mm, respectively). Relatively large errors were found bilaterally for Z, Or, and Cd (1.42 mm, 2.50 mm, and 2.19 mm, respectively) (Table 2).
There was no significant difference between the vertical and horizontal errors for Z and Or, when the vertical and horizontal errors were calculated. Large vertical errors were found for N, GT, and Cd. On the other hand, while N, GT, and Cd had small horizontal errors of 0.34 mm, 1.66 mm, and 0.99 mm, respectively, their vertical errors were larger (1.83 mm, 1.6 mm, and 1.74 mm, respectively) (Table 3 and Figure 4A).
Error reduction using LA cephalograms
Identification errors were compared between the landmarks identified on PA cephalograms with and without referral to LA cephalograms. A positive value was obtained when the errors for the landmarks identified with the help of LA cephalograms were subtracted from those identified without LA cephalograms. Errors were reduced when LA cephalograms were used. This error reduction was markedly significant for N, RO, Cd, and M. When compared to cases where the LA cephalograms were not used, large error reductions were observed for the median landmarks, N and GT (0.73 mm and 0.31 mm, respectively), and for the bilateral landmarks, Z, Or, and Cd (0.23 mm, 0.24 mm, and 0.75 mm, respectively), when these landmarks were identified while referring to LA cephalograms. The error reductions were statistically significant for N and Cd (Table 2).
Error reductions (with or without use of LA cephalograms) were compared in the vertical and horizontal directions. In both directions, the difference in the number of errors had a positive value, indicating that the use of LA cephalograms reduced identification errors. Overall, the error reductions were larger in the vertical direction than in the horizontal direction, and the error reductions mostly occurred in the horizontal direction for landmarks identified with the help of LA cephalograms. Error reductions of 0.75 mm, 0.83 mm, and 0.35 mm were noted for N, Cd, and M, respectively; all of which were statistically significant. When identified without LA cephalograms, GT had a small error reduction from 1.66 mm to 1.38 mm, while N and Cd showed large reductions from 1.83 mm to 1.08 mm, and from 1.74 mm and 0.91 mm, respectively (Table 3 and Figure 4B).
DISCUSSION
Facial asymmetry may be defined as deviation of the mandible and maxilla to the left or right, or as differences in facial height or width between the two sides of the face.16 The PA cephalograms are needed to assess facial asymmetry,234 and precise identification of landmarks is crucial for appropriate diagnosis and treatment planning. However, identification of landmarks is more challenging on PA cephalograms than on LA cephalograms, and hence, PA cephalograms are not actively used in the clinical setting. The aim of the present study was to determine if errors in identification of landmarks on PA cephalograms could be reduced by using LA cephalograms, which are usually obtained along with PA cephalograms.
In this study, we used 14 of the landmarks included in the cephalometric studies already reported in literature,7,1718192021 and two additional landmarks (N and Or). The landmark N is considered as a stable landmark that is used during LA superimposition in growing children, and may be useful for PA cephalograms. Landmark Or was added with an expectation of it being helpful for tracing the vertical location of the infraorbital rim, which is drawn in an abstract manner during PA infraorbital tracing.
The combined use of LA and PA cephalograms would be useful if these cephalograms were generated in the same head position, and thus an HPA13 was used during acquisition of the biplanar radiographs to obtain LA and PA cephalograms (that were perpendicular to one another in the same vertical head rotational position). Both (LA and PA) cephalograms were displayed on the monitor next to each other during landmark identification. When using PA cephalograms alone, relatively small identification errors were noted for landmarks ANS, Me, Ms, and Ag, while relatively large errors were noted for N, GT, Z, Or, and Cd. El-Mangoury et al.6 investigated the identification errors for various landmarks, and reported the smallest error at Me and the largest at Z. Athanasiou et al.8 reported small errors for Lo, Ms, and Ag, and large errors for Cd, which is consistent with our results. However, unlike in our study, Legrell et al.9 reported that the location and shape of Ag was not uniform on PA cephalograms and lacked reproducibility. In this respect, their results are at variance with ours, in part because in our study we defined each landmark in detail prior to landmark identification, which reduced the intra-observer errors.
An analysis of identification errors in the vertical and horizontal directions for each landmark revealed no significant difference between the vertical and horizontal errors for Z and Or. However, the vertical errors were greater than the horizontal errors for the landmarks N, GT, and Cd. Further, Z had large errors in both the vertical and horizontal directions as the zygomaticofrontal suture was not clearly visible in some patients. The Or landmark also had large errors in both the vertical and horizontal directions, which could be attributed to the overlap of the landmark on the petrous part of the temporal bone. Vertical errors were larger than horizontal errors for N, Cd, and GT.
Although the horizontal position of the median landmarks, N and GT, were located accurately, their vertical positions were identified with lesser precision as the influence of vertical errors on identification of median landmarks was probably underestimated. Our finding that the directionality varied depending on the definition of the landmark is consistent with the report by Athanasiou et al.8 The large errors for Cd may be attributed to the overlap of the nodules on the joints that hindered landmark identification.
Errors were reduced for all landmarks when the landmarks were identified with LA cephalograms as opposed to when they were identified without them. Although an error reduction was observed for Or, this was not statistically significant. Generally, Or is a bilateral landmark, and its projection is different for the left and right sides, making it hard to distinguish the structures on the right side from those on the left. On the contrary, the projection for N, a median landmark, could be relatively precisely visualized, and a statistically significant error reduction was observed for this landmark. Errors were significantly reduced for the two landmarks (N and Or) that were newly added in the present study, and the characteristics of each landmark contributed to error reductions to a different extent.
A variation in the error values obtained was noted when the vertical and horizontal errors identified with or without using LA cephalograms were compared, indicating that the use of LA cephalograms helped to reduce errors in both the vertical and horizontal directions. Overall, error differences were greater in the vertical direction than in the horizontal direction, confirming that errors are mainly reduced in the vertical direction when LA cephalograms are used.
In this study, the use of LA cephalograms was conducive to overall reduction in vertical error. However, they were not helpful for landmark identification on PA cephalograms in situations where it was difficult to precisely locate landmarks on the LA cephalograms. Among the landmarks N, GT, and Cd, which had large vertical errors, GT cannot be identified on LA cephalograms based on its definition, and hence, there was no significant difference in error when it was identified with or without the use of LA cephalograms. In contrast, N and Cd are structures that can be relatively clearly visualized on LA cephalograms. They had large error reductions (from 1.83 mm to 1.08 mm and from 1.74 mm to 0.91 mm, respectively) when identified using LA cephalograms and the differences were statistically significant for both. Assessment of Cd in the vertical direction is particularly important since this measurement is used to assess the growth of the mandible, to measure the length of the mandibular ramus (which provides an insight into the causes and patterns of facial asymmetry), and to compare the preoperative and postoperative outcomes in patients who undergo orthognathic surgery.2223 A significant reduction in the identification error for Cd with the use of LA cephalograms suggests that Cd will be used in the clinical setting.
Major et al.7 reported that use of landmarks with errors > 1.5 mm should be avoided, while landmarks with errors larger than 2.5 mm are inappropriate for clinical use. In the present study, when landmarks were located on PA cephalograms without the aid of LA cephalograms, N, GT, and Cd had vertical errors of 1.83 mm, 1.66 mm, and 1.74 mm, respectively (all > 1.5 mm), and were hence considered inappropriate for use. However, their vertical errors were reduced to 1.08 mm, 1.38 mm, and 0.91 mm, respectively, after they were located on PA cephalograms while referring to LA cephalograms. Accordingly, these landmarks were considered valid in the vertical direction and appropriate for clinical use.
Our present findings suggest that the use of LA cephalograms during landmark identification on PA cephalograms can reduce identification errors, and is more effective when both LA and PA cephalograms are acquired in the same head position. The LA and PA cephalograms are conventionally obtained together in the clinical setting. A greater reduction in landmark identification error can be achieved by using an HPA aligner during the acquisition of cephalograms. The PA and LA cephalograms previously obtained using the principles of biplanar radiography may be useful for comparison of preoperative and postoperative conditions after the new PA and LA cephalograms are obtained. The head posture was maintained in LA and PA cephalograms taken using HPA, and this improved landmark identification. Thus, we recommend the use of HPA for maintaining the head posture and consistency during cephalometric analysis.
In the present study, the errors were reduced when landmarks were identified on PA cephalograms while using the LA cephalograms, and this was specifically applicable to the errors in vertical direction rather than the horizontal direction. Landmarks that are clearly visible in the vertical direction on LA cephalograms may be used as landmarks on PA cephalograms, and can be of significant assistance in the process of landmark identification during the diagnosis, treatment planning, and assessment of facial asymmetry in the clinical setting. Additional research to evaluate whether the use of submentovertex cephalograms can reduce identification errors on PA cephalograms is necessary.





 XML Download
XML Download