

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Enamel demineralization is a significant consequence of orthodontic treatment in patients with poor oral hygiene and its prevention is one of the greatest challenges faced by clinicians despite recent advances in caries management. Fixed orthodontic appliances not only make conventional oral hygiene procedures difficult but also increase the number of plaque-retentive sites on the surfaces of teeth that are normally less susceptible to caries development.1 After such appliances are introduced into the oral cavity, the microbial flora of plaque exhibits a rapid shift toward acidogenic bacteria, most notably Streptococcus mutans and Lactobacilli.2,3 Therefore, caries progression is faster in patients with fixed orthodontic appliances. In particular, the development of white spot lesions (WSLs) around brackets is attributed to prolonged plaque accumulation.4,5,6,7,8 WSLs become noticeable within 1 month of bracket placement, whereas caries development usually takes at least 6 months.9 These lesions are commonly seen on the buccal surfaces of teeth with brackets, especially in the gingival region.4,8,10
Fluoridated toothpastes are considered the most effective agents for preventing enamel demineralization. The efficacy of the conventional toothpaste (1,000-ppm fluoride) has been documented in many studies; evidence suggests that toothpaste containing 5,000 ppm fluoride can further reduce demineralization and enhance remineralization.11,12 However, complete elimination of WSLs is unlikely because of rapid remineralization of the enamel surface in the presence of high fluoride concentration, which restricts the passage of ions into the deeper, more affected layers. Therefore, direct application of a high concentration of fluoride is not recommended.13
Another preventive method is application of low levels of fluoride and calcium ions, which can penetrate deep into WSLs, such as in the form of a casein phosphopeptide. amorphous calcium phosphate complex (CPPACP). CPP-ACP maintains a supersaturated state of calcium and phosphate to enhance enamel remineralization.14 At present, CPP-ACP is available in a variety of gels, creams, and mousses and can also be incorporated into chewing gum.
Some initial reports have shown that Clinpro™ Tooth Creme (3M ESPE, St. Paul, MN, USA), a 0.21% (w/w) sodium fluoride (950-ppm fluoride) anticavity toothpaste containing functionalized β-tricalcium phosphate (fTCP), is useful for reducing WSLs. fTCP is produced by milling TCP with sodium lauryl sulfate. This process prevents undesirable interactions between calcium and fluoride, which could render both inactive. fTCP stabilizes fluoride in solution and maintains high concentrations concentrations of calcium phosphate and fluoride in WSLs. Therefore, it could prevent and resolve enamel demineralization during orthodontic treatment.
Quantitative light-induced fluorescence (QLF™; Inspektor Research Systems, Amsterdam, Netherlands) is a validated instrument for assessing the mineral contents of smooth-surface lesions.15 The aim of this in vitro study was to examine the effects of fluoridated, CPP-ACP-containing, and fTCP-containing toothpastes on remineralization of WSLs by using QLF-D Biluminator™ 2 (Inspektor Research Systems), which is a new QLF™ system used in combination with high-definition digital single-lens reflex (DSLR) imaging.
MATERIALS AND METHODS
Specimens
Forty-eight premolars extracted for orthodontic reasons from 12 patients at Wonkwang University Dental Hospital were used as the specimens. The teeth had no visible cracks, hypoplastic areas, and buccal-surface caries. Calculus and remaining soft tissue were removed with a scaler and periodontal curette. The specimens were stored in distilled water until use.
Specimen preparation
The enamel surfaces of the specimens were cleaned with a rubber prophylaxis cup at slow speed by using a mixture of nonfluoridated pumice and water. Afterward, the teeth were rinsed with distilled water and thoroughly dried. Then, the root part of each tooth was embedded in self-curing acrylic resin (Orthocryl®; Dentaurum, Ispringen, Germany). The enamel surfaces were painted with an acid-resistant nail varnish, except for a window of 2 × 3 mm2 at the center of the buccal surface, to prevent contact with the demineralizing and remineralizing agents.
When the varnish dried, each tooth was soaked in demineralizing solution at 37℃ for 96 hours to create WSLs. The demineralizing solution consisted of 0.1-mol lactic acid (Sigma-Aldrich, St. Louis, MO, USA) and 0.2% Carbopol® ETD 2050 polymer (Lubrizol, Wickliffe, OH, USA) saturated with calcium and phosphorus. The solution was changed daily during this experiment.
At the end of the demineralization phase, the relative fluorescence loss (ΔFinitial) was calculated as the pretreatment (baseline) fluorescence value. Light-induced fluorescent images were captured by using an intraoral fluorescence camera (Inspektor Research Systems BV), stored on a personal computer with image-capturing software (C3 version 1.16; Inspektor Research Systems), and examined with analyzing software (QA2 version 1.16; Inspektor Research Systems).
Treatment groups
For the treatment phase, the specimens were randomly and equally divided into four groups.
Control group
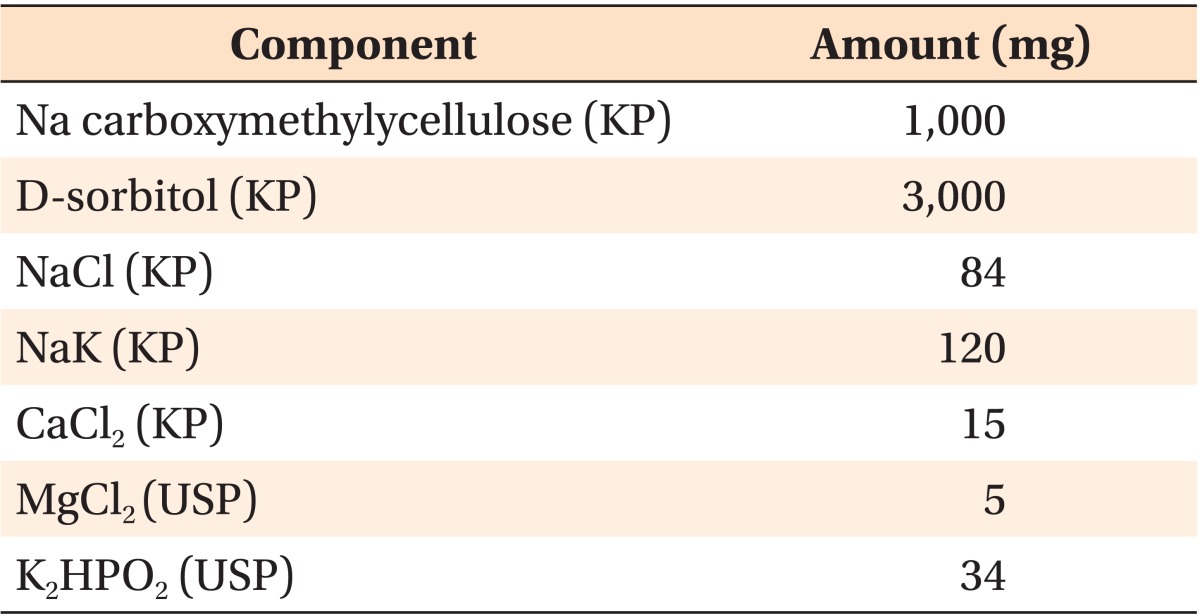
The specimens were rubbed with deionized water by using cotton swabs twice daily for 2 weeks. At other times, they were immersed in a 1:1 mixture of artificial and human stimulated saliva (saliva solution) to reproduce the oral environment. Taliva® solution (Hanlim Pharm, Seoul, Korea) was used as the artificial saliva; Table 1 shows its composition. Stimulated saliva was collected from men in their twenties with no medical history and was centrifuged. Only the upper layer of the centrifuged saliva was used for the experiment.
Fluoride group
On each specimen, 1,000-ppm fluoride-containing toothpaste (2080®; Aekyung Industrial, Seoul, Korea) was applied for 3 minutes twice a day over 2 weeks by using a toothbrush. The specimens were otherwise soaked in the saliva solution after rinsing. The saliva solution was changed daily.
CPP-ACP group
CPP-ACP.containing toothpaste (GC Tooth Mousse®; GC, Tokyo, Japan) was applied for 3 min to each tooth twice a day for 2 weeks by using a fingertip. The specimens were soaked in the saliva solution without rinsing at other times. The saliva solution was changed daily.
fTCP group
fTCP-containing toothpaste (Clinpro™ Tooth Creme) was applied for 3 minutes to each tooth twice a day for 2 weeks by using a toothbrush. The specimens were soaked in the saliva solution without rinsing. The saliva solution was changed daily.
The fluorescence value of each specimen measured with QLF-D Biluminator™ 2 after the 2 weeks of treatment (post-treatment) was recorded as ΔFfinal. The difference between ΔFfinal and ΔFinitial (ΔF) was calculated to quantify the change in fluorescence of each specimen.
Statistical analysis
All measurements were performed and repeated twice by the same investigator. The measurement error was assessed by Dahlberg's formula and intraclass correlation. The first set of measurements was used for analysis. The Shapiro.Wilk test showed that the measurements were normally distributed. The measurements of the treatment groups were compared by using the Mann-Whitney U-test. Statistical analyses were performed by using SPSS program (version 14.0; SPSS Inc., Chicago, IL, USA). The level of statistical significance was established as p < 0.05. At the pretreatment and post-treatment time points, the measurement errors by Dahlberg's formula were 0.2177 and 0.2220, respectively, and the intraclass correlation coefficients were 0.994 and 0.995, respectively.
RESULTS
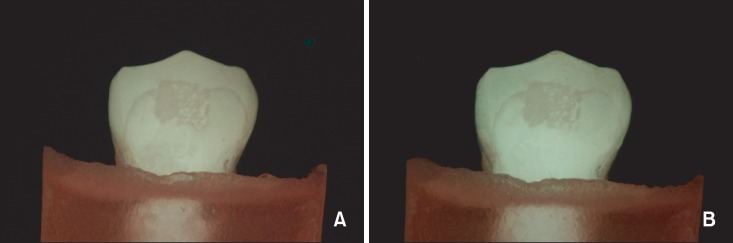
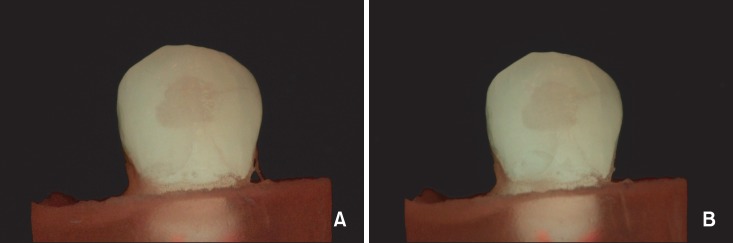
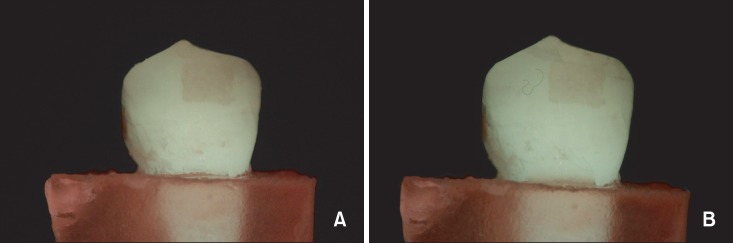
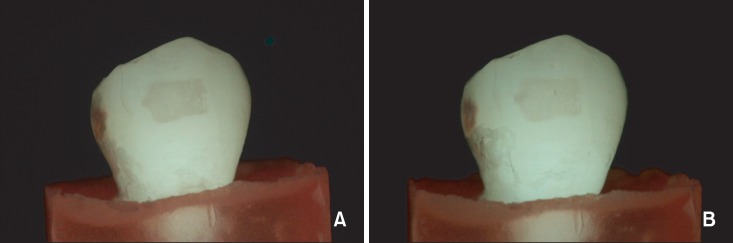
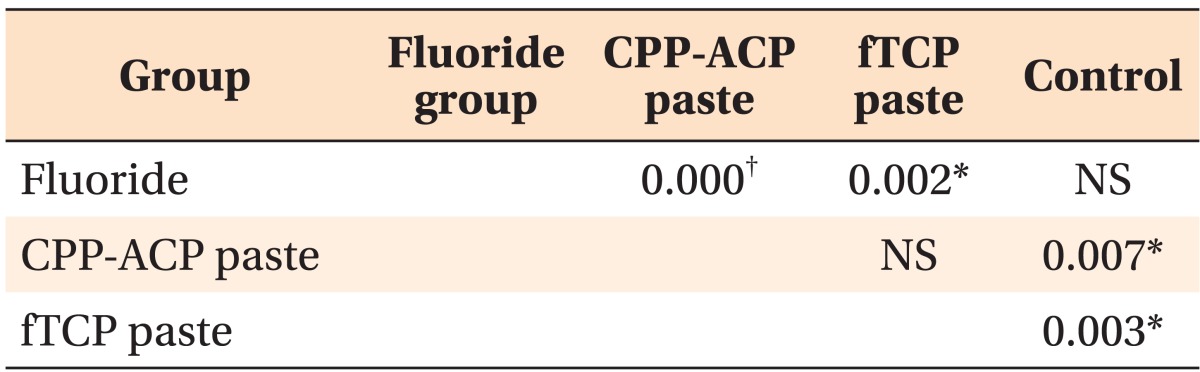
Mean ΔFinitial was not significantly different among the groups. However, mean ΔF was higher in the fTCP and CPP-ACP groups than in the fluoride and control groups. The fluoride group did not show a significant difference from the control group (Table 2). The percent increase in fluorescence after the treatment was 0.480%, 0.500%, 0.940%, and 1.446% in the control, fluoride, CPP-ACP, and fTCP groups, respectively. Figures 1,2,3,4 show the pretreatment and post-treatment light-induced fluorescent images of one specimen from each group.
DISCUSSION
WSLs are not unique to orthodontic patients: they are observable in 3-82% of the children who have not received orthodontic treatment.16,17,18,19 In the orthodontic population, however, the prevalence rate of WSLs ranges from 8.5% to 44% on the anterior teeth and 7.7% to 71% on the posterior teeth.20 The results of the present study indicate that application of fTCP- or CPP-ACP-containing toothpaste may reduce WSLs, compared with use of 1,000-ppm fluoride-containing toothpaste.
In the present study, the application of CPP-ACP-containing toothpaste resulted in a significant increase in fluorescence. The remineralization of WSLs with CPP-ACP has been previously studied with conflicting results. Bröchner et al.,21 in a prospective clinical trial, found that WSL regression was comparable between CPP-ACP-containing and traditional toothpastes. They reported that application of CPP-ACP-containing toothpaste after debonding of orthodontic appliances resulted in significantly increased fluorescence and reduced lesional area after 4 weeks of treatment, as assessed by QLF™. The improvement was however not superior to "natural" regression occurring with daily use of fluoridated toothpaste. By using laser fluorescence, Bhat et al.22 found that application of CPP-ACP-containing cream with and without fluoride for 14 and 21 days, respectively, led to significant differences in remineralization of incipient enamel lesions. However, by using a pH-cycling model of early caries in bovine enamel, Ogata et al.23 reported insufficient remineralization of enamel subsurface lesions with CPP-ACP. Polarized light photomicrographs and microradiographs did not reveal significant differences in mineral gain between CPP-ACP-treated and control groups; addition of low levels of fluoride was needed to observe lesional regression. The conflicting results of these studies may be related to the different methods of specimen preparation, treatment periods, and additional application of fluoride.
In the fTCP group, we used 950-ppm sodium fluoride toothpaste containing fTCP, which, according to the manufacturer, is an innovative calcium-based additive that can help to remineralize enamel. By in vitro pH-cycling experiments designed to mimic remineralization of incipient enamel lesions, Karlinsey and Mackey24 reported that the combination of sodium fluoride with fTCP in a simple aqueous solution produces significantly greater surface and subsurface rehardening of WSLs than use of fluoride alone. This result is similar to our findings.
Use of higher-concentration (1,500-5,000 ppm) fluoride toothpastes and gels twice daily during orthodontic treatment has a demineralization-inhibiting tendency.25 However, such high doses of fluoride have negative effects, so the Korea Food and Drug Administration has recommended that the total fluoride content of toothpaste should be less than 1,000 ppm. Further, although use of high doses of fluoride completely arrests the carious process, which is ideal for posterior carious lesions, WSLs of orthodontic origin present a cosmetic challenge and regression is the therapeutic goal. If a high dose of fluoride is used locally, the arrested lesion will remain the same size and frequently becomes stained with organic debris. Moreover, natural remineralization produces greater resistance to further dissolution because components are replaced with less-soluble substances having larger crystals during remineralization.26 This phenomenon has been reported as plugging of the diffusion pathways of enamel by hydroxyapatite crystals and as hyper-remineralization.6
To the best of our knowledge, this study is the first direct comparison of the remineralization effects of 1,000-ppm fluoride-, CPP-ACP-, and fTCP-containing toothpastes on WSLs, although quantitative assessment of fluoridated and CPP-ACP-containing toothpastes has been reported. The better findings in the CPP-ACP and fTCP groups than in the fluoride group may be attributable to the lack of rinsing in the former groups. Further, the CPP-ACP- and fTCP-containing toothpastes were applied for longer than the actual clinical usage and the saliva solution was changed once a day. This study improves our understanding of the preventive potential of the products, but it cannot reproduce all the complexities of the living oral cariogenic environment. Well-designed controlled clinical trials studies are required to examine the potential benefits of CPP-ACP with fluoride and microabrasion with fTCP on remineralization.
 XML Download
XML Download