

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Behavioral variant frontotemporal dementia (bvFTD) is the most common clinical syndrome of frontotemporal dementia (FTD) and it may have different subtypes: the pathological subtypes include tau, transactive response DNA-binding protein 43 kDa (TDP-43), and fused in sarcoma (FUS) inclusions,1 while the clinical phenotypes can be dichotomized into disinhibited- and apathy-predominant types.2 Neuroimaging studies have also revealed several anatomical subtypes.34 However, only a few studies have investigated the relationship between these subtypes and disease progression or prognosis.5678
We often encounter patients with bvFTD who show one of two patterns of frontal lobe atrophy on axial magnetic resonance imaging (MRI) scans: 1) diffuse frontal atrophy (D-type) or 2) focal or circumscribed frontal atrophy (F-type). However, little is known about whether the clinical manifestations and prognoses differ between D- and F-type patients. Pick's disease (PiD) is characterized by marked circumscribed prefrontal lobe atrophy.9 Based on previous neuroimaging studies, we presumed that 4R-tau-positive disorders such as progressive supranuclear palsy (PSP) and corticobasal degeneration (CBD) result in less prefrontal atrophy than in PiD.1011 Given that motor symptoms are more common in patients with CBD or PSP than in those with PiD,1112 we hypothesized that D-type patients are more likely to be associated with motor symptoms, while F-type patients are less likely to exhibit parkinsonism or motor symptoms. In addition, since there are often more focal signs for localized injury than for diffuse injury, we hypothesized that F-type bvFTD patients have a more favorable outcome than D-type patients.
The objectives of this study were 1) to classify patients with bvFTD into the D- and F-types based on axial MRI scans, and 2) to compare the baseline characteristics, progression in motor and cognitive symptoms, and survival time between these two groups.
METHODS
Participants
In total, 81 patients were retrospectively recruited from 8 dementia clinics across Korea. All patients enrolled in this study met the clinical criteria for probable bvFTD as proposed by the International Behavioural Variant Frontotemporal Dementia Criteria Consortium.13 Of the 81 initial patients, 2 with motor neuron disease and 5 with incomplete clinical information were excluded, and hence 74 patients were finally enrolled in this study.
This study was conducted as part of the Clinical Research Center for Dementia of South Korea-Frontotemporal Dementia (CREDOS-FTD) registry study,14 a government-funded dementia research project conducted by dementia specialists from neurological and psychiatric clinics.15 All patients were evaluated with comprehensive interviews, neurological examinations, and neuropsychological assessments. In brief, caregivers were interviewed in depth by neurologists and neuropsychologists. Blood tests to exclude secondary causes of dementia included a complete blood count, blood chemistry tests, thyroid function tests, vitamin B12/folate, and syphilis serology. Conventional brain MRI scans confirmed the absence of structural lesions such as brain tumors, traumatic brain injuries, hydrocephalus, or severe white matter diseases (cap or band ≥10 mm and deep white matter lesion ≥25 mm). A committee that included 5–10 dementia specialists held a quarterly meeting to review the clinical histories and brain imaging results of all cases enrolled in this study and to reach a consensus which ascertained the clinical diagnosis.
Standard protocol approvals and registration
The Institutional Review Boards at all of the participating centers approved this study. Written informed consent was obtained from all participants or their caregivers prior to conducting any study procedures.
Baseline clinical evaluation
We used the FTD Evaluation Package developed by CREDOS-FTD, which comprises a clinical evaluation form and a caregiver questionnaire form. The clinical evaluation form was designed to obtain the following information: 1) the history of cognitive decline as reported by the caregiver, 2) the results of a neurological examination, and the scores for the 3) Korean Mini-Mental State Examination (K-MMSE),16 4) Frontotemporal Lobar Degeneration-Clinical Dementia Rating Sum of Boxes (FTLD-CDR SB),17 5) Global Deterioration Scale (GDS),18 6) Hachinski Ischemic Scale (HIS),19 and 7) Geriatric Depression Scale-Short Form (GDS-SF).20
The caregiver questionnaire form was designed to obtain the following information: 1) basic demographic data about the patient and caregiver, 2) the lifestyle and family history, 3) the past medical history including vascular risk factors, 4) Korean Dementia Screening Questionnaire (KDSQ) score,21 5) Barthel Activities of Daily Living (ADL) index,22 and scores for the 6) Seoul Instrumental Activities of Daily Living (SIADL),23 7) Caregiver-Administered Neuropsychiatric Inventory (CGA-NPI),24 and 8) Frontal Behavioral Inventory (FBI).25
Neurologists evaluated the baseline motor signs and symptoms of 64 patients with bvFTD using the score on the Unified Parkinson's Disease Rating Scale (UPDRS) Part III.26
Baseline neuropsychological assessment
All patients underwent a standardized neuropsychological test battery known as the cognitive test battery for frontotemporal dementia (FTD-Cog), which assesses the subdomains of attention, language and related functions, visuospatial function, memory, and frontal/executive function. The FTD-Cog is described in detail elsewhere.14
Visual rating of diffuse versus focal frontal lobe atrophy on axial MRI scans
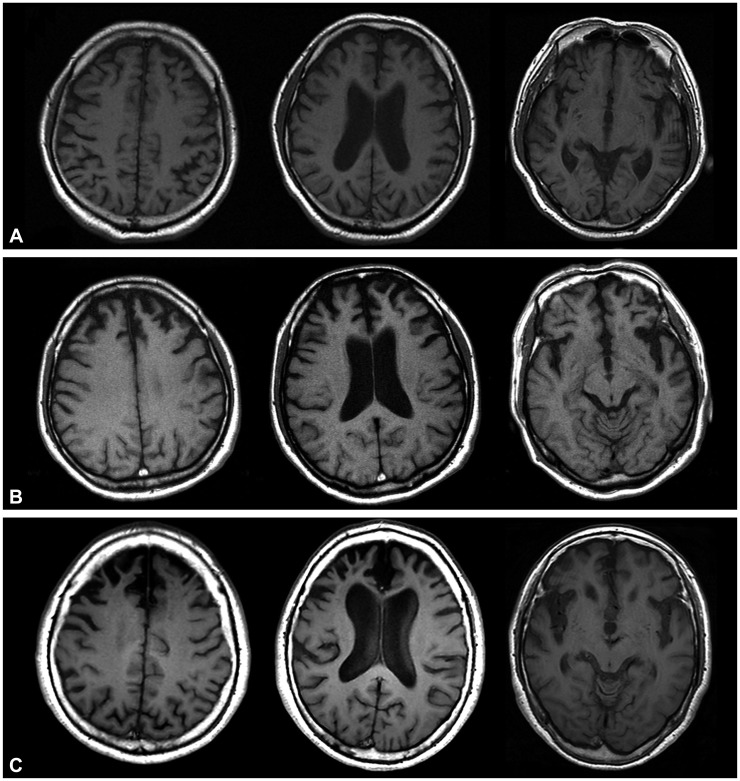
We used an MRI visual rating scale to rate brain images in this study, which involved assessing anterior frontal lobe atrophy at the following three axial levels in T1-weighted MRI or fluid-attenuated inversion recovery MRI scans: 1) the slice just superior to the lateral ventricle on either side of the brain, 2) the slice just superior to the last view of the insular cortex on either side of the brain, and 3) the slice with the most complete view of the orbitofrontal cortex around the interpeduncular cistern (Supplementary Fig. 1 in the online-only Data Supplement). These three axial slices in MRI scans were referenced and modified based on previous studies.272829
The ratings were performed by comparing a single selected image with three standard images (Fig. 1). The overall rating for each case was the highest (worst) atrophy rating score recorded among the three defined axial levels on the MRI scans. The lateralization of brain atrophy was recorded when the ratings for any region were not symmetric.
Ratings were based on the following scale: 0=no atrophy or diffuse atrophy (D-type), equal to standard no. 1 (Fig. 1A) and less than standard no. 2 (Fig. 1B); 1=mild-to-moderate focal atrophy (F1-type), equal to or more than standard no. 2 and less than standard no. 3; and 2=severe focal atrophy (F2-type), equal to or more than standard no. 3 (Fig. 1C). This rating process was rapid, with each case taking 2–3 min, and was based on standard clinical-quality axial MRI scans.
In this study, the scans were anonymized and their order randomized prior to rating. The ratings were performed by two neurologists who were blinded to the identity of each subject and the clinical features. The responses of the raters could have been biased if they were aware that the MRI scans they were going to rate were only from bvFTD patients, and so we included 20 MRI scans from age-matched normal controls and presented all of the MRI scans in a random order. These 20 MRI scans were from normal controls with no history of neurological or psychiatric illness, no abnormalities on neurological examinations, no subjective memory complaint, and normal cognition according to the K-MMSE. Any discrepancies identified after all of the scans had been rated were resolved by consensus between the two raters.
Comparison of baseline variables between the D- and F-types
The following variables were compared between D- and F-type patients: age at symptom onset, age at diagnosis, duration of education, disease duration at diagnosis/time of MRI scan, disease duration to final follow-up, family history of dementia, Parkinson's disease, psychiatric disorders, vascular risk factors, Barthel ADL index, and scores for the K-MMSE, FTLD-CDR SB, GDS, HIS, GDS-SF, KDSQ, SIADL, CGA-NPI, FBI, UPDRS Part III, and FTD-Cog.
Comparison of motor and cognitive progression between the D- and F-types
The longitudinal progression of motor and cognitive symptoms was also compared between the two groups. A retrospective review of the full medical records was conducted by an independent neurologist who had not been involved in designing this study. The medical records were investigated for newly observed motor symptoms and disease duration. Motor symptoms were defined as significant if at least one of four cardinal signs had been observed by clinicians: rigidity, tremor, bradykinesia, or postural instability. Antipsychotics are widely applied to treat abnormal behavior symptoms in bvFTD patients, and so it is crucial to differentiate between motor symptoms with underlying neurodegenerative pathology and drug-induced parkinsonism (DIP). We therefore also investigated whether patients were taking antipsychotics as well as the causality of motor symptoms.
We were unable to apply the FTD-Cog at the follow-up to most of the participants due to their poor cooperation in these tests. Therefore, the final K-MMSE scores were used in this study to evaluate cognitive function at the follow-up.
Comparison of survival time between the D- and F-types
Survival analyses were performed in 62 of the 74 bvFTD patients, with the vital status of each confirmed using the database of the Korea Ministry of Government Administration and Home Affairs or via a telephone interview during June 2015.
Statistical analyses
Comparisons were performed across MRI visual rating subtypes and clinical data. Student's t-test and the chi-square test were used as appropriate to compare the demographic and clinical characteristics of the groups. The three groups (D-, F1-, and F2-types) were compared using analysis of variance (ANOVA) with Tukey post-hoc tests. A multiple linear regression model adjusted for covariates (age at onset, sex, UPDRS Part III score at baseline, and disease duration at the time of MRI scanning) was used to evaluate the relationship between the subtypes and the disease duration without motor symptoms. Repeated-measures ANOVA with Bonferroni post-hoc test was used to compare K-MMSE scores at baseline and follow-up. In addition, we used Kaplan-Meier survival analysis grouped by MRI visual rating subtypes and with log-rank post-hoc testing. Multivariate Cox proportional-hazards regression analysis was used to identify factors that influenced survival. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. SPSS (version 20, SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
RESULTS
Inter- and intrarater agreements for the MRI visual rating scale
The intrarater reliability determined for all 94 scans was excellent, with Cohen's kappa values of 0.79 and 0.71 for raters 1 and 2, respectively. The interrater reliability analysis also showed substantial agreement, with a Cohen's kappa value of 0.82.
Based on an axial MRI visual rating scale, the 20 MRI scans from age-matched normal controls were classified into 16 D- and 4 F1-types (i.e., mild-to-moderate focal atrophy), while the 74 MRI scans from bvFTD patients were classified into 35 D- and 39 F-types. Subclassifying the 39 F-type was into two types by severity revealed 22 of the F1-type (mild-to-moderate focal atrophy) and 17 of the F2-type (severe focal atrophy). Most (n=57, 77.0%) of the 74 bvFTD patients had symmetric atrophy, while most (n=11, 64.7%) of the 17 asymmetric scans indicated left-sided atrophy.
Comparisons of baseline demographic data and dementia rating scales between the D- and F-types
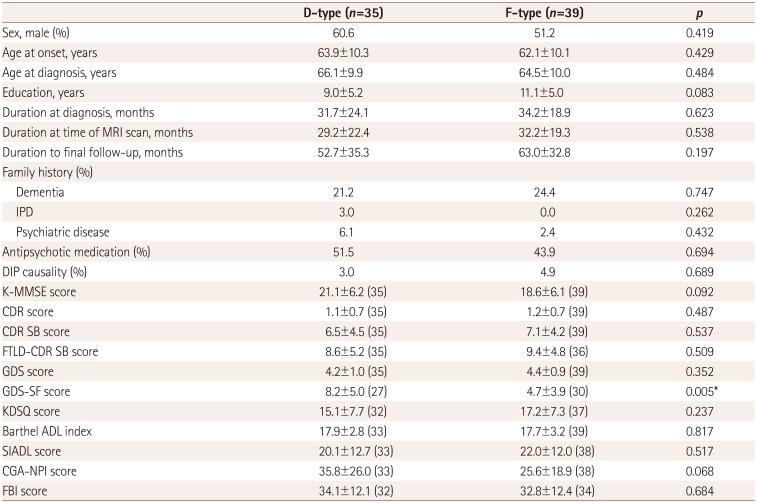
The demographic and clinical data at baseline between the D- and F-types are compared in Table 1. The only significant difference between these two subtypes at baseline was in the total GDS-SF score, which was significant higher in the D-type than in the F-type [8.2±5.0 vs. 4.7±3.9 (mean±SD), p=0.005]. There was a tendency for the CGA-NPI total score to be higher in the D-type than in the F-type, but the difference was not statistically significant (35.8±26.0 vs. 25.6±18.9, p=0.068). However, comparing the subscale scores revealed that those for agitation and disinhibition were significantly higher in D-type patients than in F-type patients (Supplementary Table 1 in the online-only Data Supplement).
Comparisons of UPDRS Part III score and neuropsychological performance at baseline between the D- and F-types
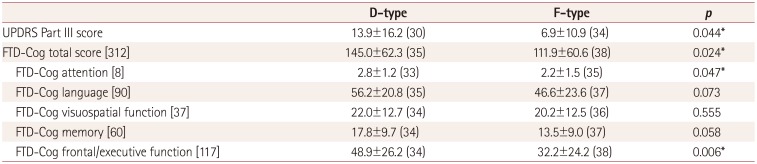
Table 2 presents the results of comparisons of the UPDRS Part III score and neuropsychological tests between the two subtypes of bvFTD. The score for UPDRS Part III at baseline was significantly higher in the D-type (13.9±16.2) than in the F-type (6.9±10.9, p=0.044). D-type patients exhibited better neuropsychological performance than F-type patients, as indicated by significantly higher mean scores for the FTD-Cog total (p=0.024), attention (p=0.047), and frontal/executive function (p=0.006) components.
We also compared the FTD-Cog and UPDRS Part III scores among the D-, F1-, and F2-types. The mean scores for the FTD-Cog total (p=0.036), memory (p=0.016), and frontal/executive function (p=0.011) components differed significantly among the three subtypes. Post-hoc analyses revealed that FTD-Cog total, memory, and frontal/executive function scores were significantly higher for the D-type than the F2-type, but not the F1-type. The UPDRS Part III scores did not differ significantly among the three subtypes (p=0.114).
Comparisons of motor and cognitive progression between the D- and F-types
We used the mean disease duration without motor symptoms (i.e., the period after the baseline measurements during which the patient was free of motor symptoms) to analyze the occurrence of incident motor symptoms in patients with bvFTD. Based on a retrospective review of the medical records and the UPDRS Part III scores, 23 of the 74 patients were excluded because they already had prominent motor symptoms (including 3 patients with DIP). Ten patients with absent baseline UPDRS Part III scores were also excluded, leaving 41 patients without prominent motor symptoms at baseline in this analysis: 17 with the D-type and 24 with the F-type.
The disease duration to the final follow-up was 65.1±35.8 months. Motor symptoms appeared in 9 (52.9%) of the 17 D-type patients and in 6 (25.0%) of the 24 F-type patients. The incidence rate of motor symptoms was higher in those with D-type, but the difference was not statistically significant (p=0.067). Table 3 compares the disease durations without motor symptoms across the subtypes. Multiple linear regressions were performed after controlling for age at onset, sex, UPDRS Part III score at baseline, and disease duration at the time of MRI scanning across the subtypes. The MRI subtype (from D-type to F-type) was positively correlated with the increased motor-free period (β=16.423, standard error=5.826, p=0.008). We observed that the disease duration without motor symptoms was significantly longer for the F-type (61.0±27.1 months) than for the D-type (46.3±30.1 months).
Differences in baseline cognitive function, as evaluated using the FTD-Cog, were consistently seen in the follow-up cognitive assessments. Although the mean K-MMSE score at baseline did not differ significantly between the two subtypes (p=0.092) (Table 1), repeated-measures ANOVA showed that the K-MMSE score at follow-up was significantly higher in the D-type than the F-type (18.4±7.8 vs. 11.3±8.7, p=0.010) (Table 3) after adjusting for the duration from disease onset to the final follow-up. In addition, the K-MMSE score was significantly higher in the D-type than the F2-type (7.8±7.8, p<0.001), but not the F1-type (14.1±8.5, p=0.205).
Survival analyses
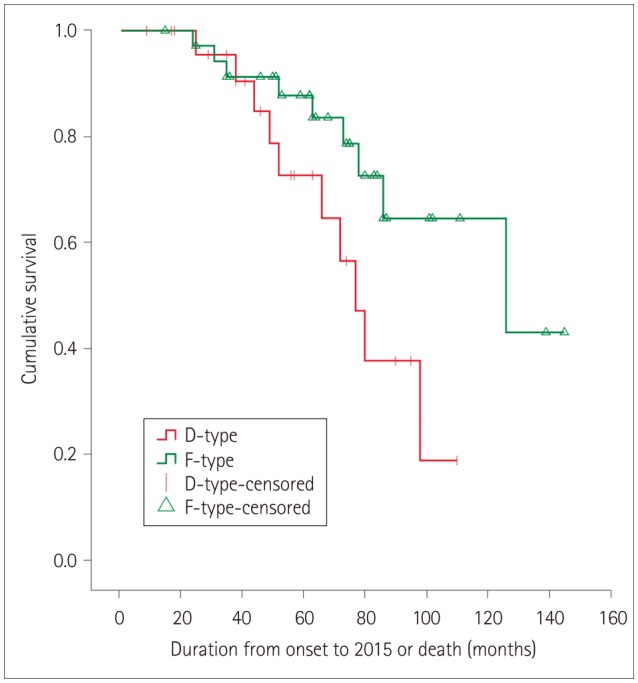
In total, 19 deaths were confirmed in survival analyses for 62 members of this cohort. The overall median survival from the onset of the first symptom was about 8.5 years. The median survival time was shorter for the D-type (6.9 years, 95% CI=5.6–8.4 years) than for the F-type (9.4 years, 95% CI=8.0–10.8 years). Kaplan-Meier plots showed a significant difference between the D- and F-types (p=0.048) (Fig. 2).
We performed a multivariate Cox proportional-hazards regression analysis to further determine the factors associated with survival. This analysis included the age at onset, sex, MRI visual rating subtypes, occurrence of motor symptoms, and the mean CDR SB, FTLD-CDR SB, and UPDRS Part III scores at baseline. The Cox regression showed that CDR SB score (HR=1.308, 95% CI=1.014–1.686, p=0.038) and UPDRS Part III score (HR=1.062, 95% CI=1.019–1.108, p=0.004) influenced the survival time after the onset of the disease, with higher scores increasing the risk of mortality.
DISCUSSION
We developed a reliable scheme for classifying 74 patients with bvFTD into the diffuse (35 patients) and focal (39 patients) types of frontal lobe atrophy using axial MRI scans. The two subtypes differed in both the prevalence of motor symptoms and survival time.
Our first major finding was that the mean UPDRS Part III score at baseline was higher (indicating greater abnormality) in the D-type than the F-type. Moreover, follow-up analyses of motor progression in patients without motor symptoms at baseline showed that the motor symptoms developed earlier in D-type than in F-type patients. Together these results suggest that extrapyramidal motor symptoms appear earlier and may progress more rapidly in D-type than in F-type patients.
Various motor symptoms are seen in bvFTD (other than motor neuron disease). These symptoms may precede, coincide, or follow abnormal behaviors, and present as rigidity, bradykinesia, abnormal posture, and (in rare cases) tremor.30 The prevalence of motor symptoms in bvFTD patients has also varied markedly between studies, from less than 10% to 22.7%.31323334
Neuropathologically, bvFTD is most often one of the FTLD proteinopathies, characterized by the accumulation of abnormal protein inclusions (e.g., tau, TDP-43, and FUS) in the cytoplasm or nuclei of neuronal and glial cells. Some investigators have reported that in comparison with tau-negative bvFTD patients, tau-positive bvFTD patients are more likely to have motor symptoms suggestive of CBD or PSP, indicating that motor symptoms may predict an underlying tau pathology.12 However, the prefrontal atrophy in patients with PSP or CBD pathology may not be so remarkable: based on previous studies, we presumed that the MRI images of PSP patients will not indicate remarkable prefrontal atrophy to parallel the frontal dysfunction on neuropsychological tests and glucose hypometabolism evident in fluorodeoxyglucose-positron emission tomography;35 volumetric MRI studies have shown that CBD is associated with diffuse atrophy including the parasagittal and paracentral regions rather than prefrontal atrophy.1136 We therefore suggest that the D-type bvFTD in our study evident in axial MRI scans was related to 4R-tau-positive pathologies. On the other hand, in line with a pathology study that demonstrated a relationship between PiD and marked circumscribed prefrontal lobe atrophy,9 our F-type patients were more likely to have either 3R-tauopathy or TDP-43 pathology. However, future studies need to further investigate this suggestion because a voxel-based morphometry study found that PiD and TDP cases exhibited fairly diffuse atrophy, whereas this was more focal in the CBD group.37
Our second major finding was that the survival time differed significantly between the D- and F-types. The overall median survival time in bvFTD patients was 8.5 years from disease onset, which is similar to previous reports (7.6 to 8.7 years).3138394041 An unexpected finding was that the cognitive function at both baseline and follow-up was better in D-type than F-type patients. However, despite this better cognitive function, the median survival time was shorter in the D-type (6.9 years) than the F-type (9.4 years). This may indicated that the appearance of motor dysfunction is more relevant than cognition to survival in bvFTD.
We therefore presume that the shorter survival in the D-type might be associated with the earlier appearance of motor symptoms compared to the F-type. Indeed, the Cox regression analyses revealed that a high UPDRS Part III score at baseline contributed to an increased risk of mortality. Another explanation for the shorter survival in D-type patients might be related to our observation that the GDS-SF and CGA-NPI total scores at baseline were higher in the D-type than the F-type. Patients with neuropsychiatric symptoms are also more likely to be treated with antipsychotics or sedatives, resulting in worse prognosis and survival.42
While our simple dichotomization between the D- and F-types based on frontal lobe atrophy alone is practical in clinical settings, bvFTD can be divided into several subtypes when both frontal and temporal atrophy are considered.3 Furthermore, some bvFTD patients have right-temporal-predominant atrophy,43 which we did not initially consider in the present study. When we reanalyzed our data using temporal atrophy as a covariate, the differences between the D- and F-types in motor symptoms and survival time disappeared. In addition, the results we obtained from the data using frontal atrophy alone were not replicated when the same analyses were performed with either temporal atrophy alone or frontotemporal atrophy combined. Details of the associated methods and results, along with representative MRI slices from all patients, are provided as supplementary data (Supplementary Methods, Supplementary Tables 2, 3, 4, 5, 6, 7, 8, and Supplementary Figs. 2 and 3 in the online-only Data Supplement).
This study was subject to several limitations. First, the clinical diagnoses of our patients were not confirmed pathologically, and so some patients diagnosed with bvFTD might have had a frontal variant of Alzheimer's disease or a mixed pathology with other etiologies.12 Second, we did not perform follow-up evaluations of the scores for the UPDRS Part III, FTD-Cog, GDS-SF, and CGA-NPI. Finally, the causes of death were not verified in the survival analyses. Notwithstanding these limitations, this study was able to identify focal and diffuse subtypes of frontal lobe atrophy in bvFTD based on an axial MRI visual rating scale. This method was found to be rapid and reliable, and can be applied in a wide range of clinical settings. Compared with the F-type, the D-type was associated with the earlier appearance of motor symptoms, greater depressive moods and caregiver stress at baseline, and shorter survival time during the disease, even though the D-type exhibited better neuropsychological performance both at baseline and follow-up.

 XML Download
XML Download