

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Migraine is a recurrent primary headache disorder with a prevalence of 8.6% in males and 17.5% in females.1 Migraines are among the most disabling and burdensome conditions.2 The Global Burden of Disease Study ranked migraine as the seventh most common disabling pathology among 289 diseases, being referred to as the 7th disabler.3 Migraine has a significant impact on both mental and physical health, since it can impair school or work performance so as to substantially decrease the quality of life, leading to social isolation.34 The problem becomes even more significant when various comorbidities such as autoimmune, gastrointestinal (GI), and psychiatric diseases are taken into account.356 Nevertheless, the pathophysiological mechanism of migraine remains elusive.7 Several mechanisms such as inflammation, pain mediators such as calcitonin-gene-related peptide (CGRP), and neurotransmitters such as serotonin89 are currently discussed; indeed, serotonin agonists such as triptans can relieve migraine, and selective serotonin-reuptake inhibitors and tricyclic antidepressants have been used successfully as prophylactic treatments.8
There is emerging research evidence for the GI system playing an important role in the pathophysiology of migraine.5810 A possible connection was initially prompted by the observation that GI symptoms such as nausea, vomiting, and gastroparesis constitute clinical hallmarks of migraine.1112 Moreover, abdominal migraine, a condition that presents with both migrainous and abdominal symptoms, suggests that a common mechanism underlies both affected systems.131415 Furthermore, migraines can often coexist with GI disorders (GID) such as inflammatory bowel disease (IBD), celiac disease (CD), irritable bowel syndrome (IBS), and Helicobacter pylori (H. pylori) infection (HPI).816171819 Moreover, GI tract (GIT) microbiota have been implicated in the pathogenesis of more than 25 diseases with CNS effects, for which multiple mechanisms have been discussed, such as bacterial translocation secondary to an impaired intestinal barrier, migration of stimulated immune cells, and the systemic diffusion of microbial products or metabolites.820 This complex interplay between the brain and GIT is referred to in the literature as the gut-brain axis, which involves immune, neuroendocrine, and metabolic pathways, although the precise pathophysiology linking the different GI entities with migraine remains unclear.810
This paper is aimed at clinicians due to there being little awareness in the broader medical community regarding this relationship.1 We believe that a better understanding of this association is likely to lead to a GID being considered a potential cause of migraine headache, in turn leading to prompt diagnoses and in fundamental migraine treatments changing from being pure symptomatic to curative.
METHODS
A PubMed search was conducted that included all papers reporting on headache associated with GI symptoms. No time restraint was set. The search was based only on papers written in English, and the keywords used were “headache,” “gastrointestinal diseases,” “migraine,” and “hemicrania.” Using these keywords in various combinations yielded the following results: “headache” AND “gastrointestinal diseases” identified 308 papers, “headache” AND “gastrointestinal disorders” identified 84 articles, “migraine” AND “gastrointestinal diseases” identified 126 articles, and “hemicrania” AND “gastrointestinal diseases” identified 1 article. Further articles were identified through a manual search of the initially revealed literature. Only original studies and case reports/series on possible mechanisms between migraine and GI symptomatology were included.
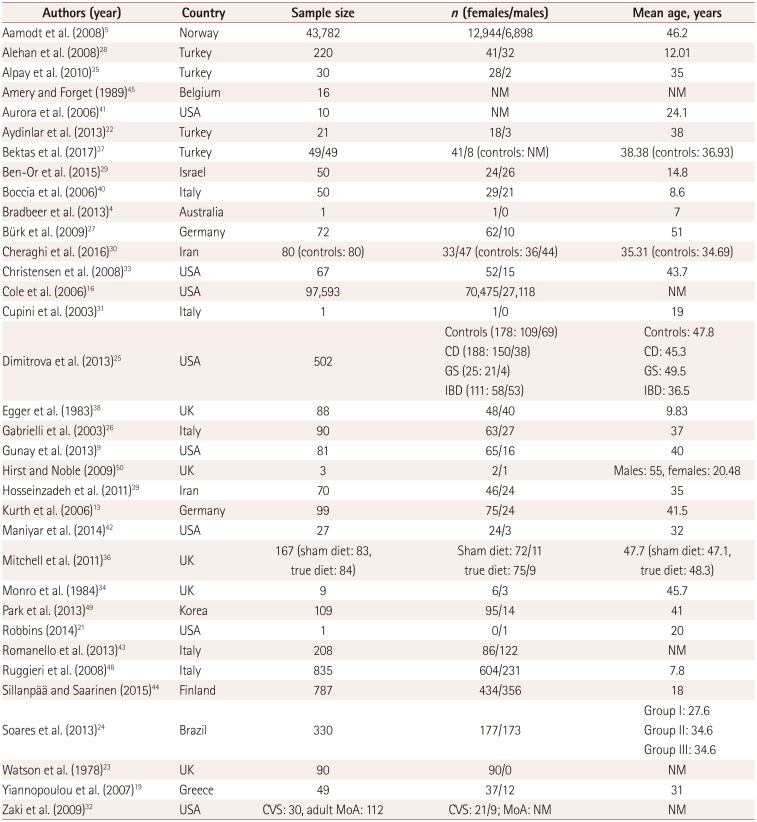
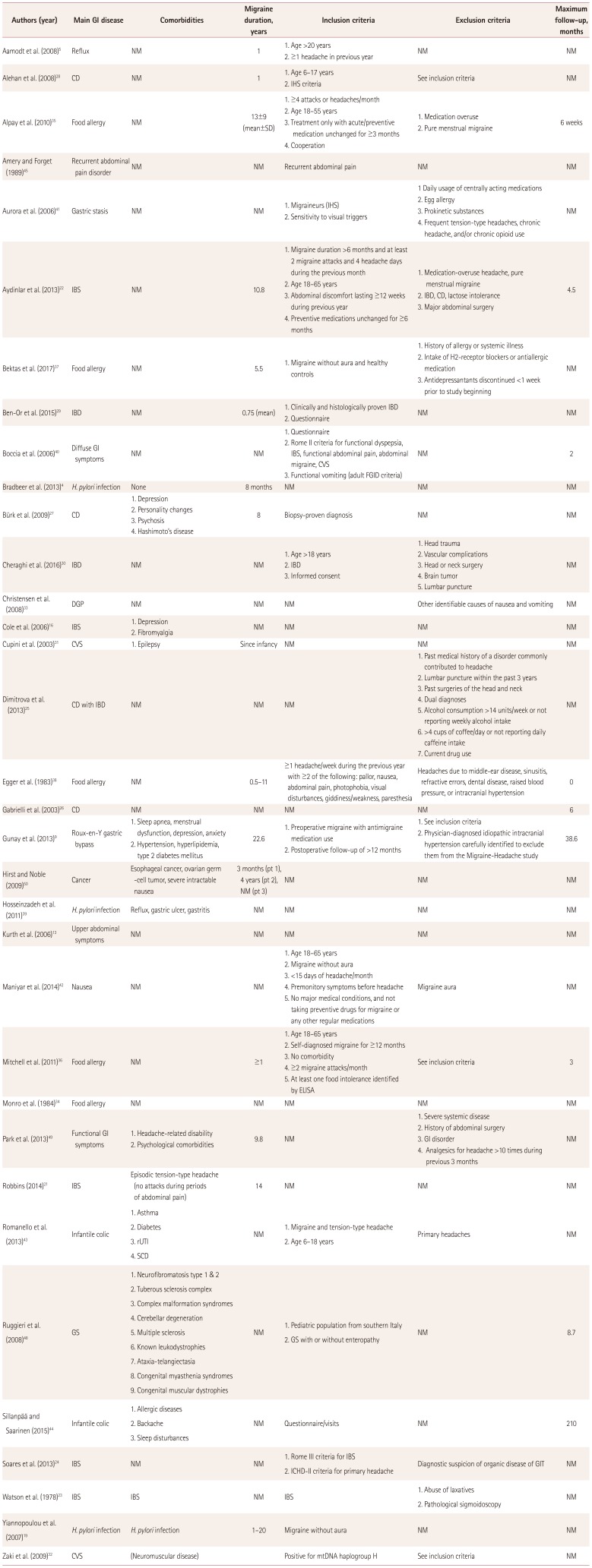
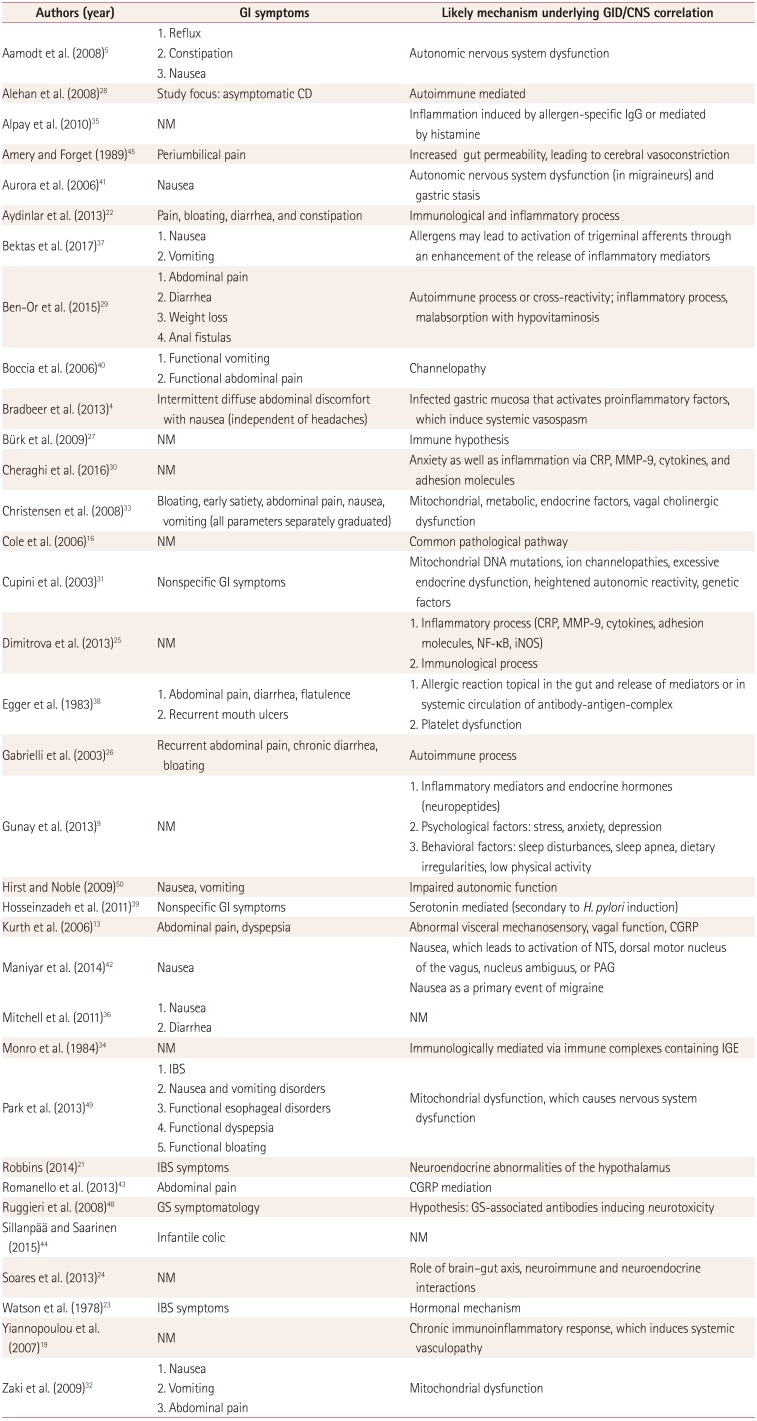
In total, 29 papers were included for the purposes of this review. Since a common pathophysiological mechanism for migraine associated with GID could not be identified, since the literature searched yielded too many findings of GID concomitant with migraine headache that each had its own pathophysiology, in the Discussion section we present in more detail the reviewed studies and report for each study the potential pathophysiological mechanisms offered by the authors. Since migraine is associated with multiple GI entities rather than a single GID, we have regrouped migraine studies in the Results section according to the associated GID in order to facilitate the overview. Further details on each reviewed study regarding demographics, study characteristics, and pathogenicity-associated parameters are tabulated in Table 1, 2, and 3.
RESULTS
While the pathophysiological mechanism(s) underlying migraine and GID remain(s) elusive, the clinical observations-although being largely anecdotal-suggest that there is an important relationship between these two conditions.
Irritable bowel syndrome
Robbins21 reported the case of a 20-year-old male experiencing periodic episodes of abdominal pain resembling cluster headache (CH), which lasted 30–120 minutes and manifested in the evenings at intervals of 2–8 weeks. He had also experienced infrequent episodic tension-type headache that did not occur during periods of abdominal pain. A diagnosis of IBS was made, and the eventual relationship between CH and IBS was supported by the observation of the effectiveness of CH prophylaxis (e.g., verapamil) in the treatment of IBS.21 Food elimination for the therapeutic management of patients with migraine and IBS was evaluated by Aydinlar et al.22 in a double-blind, randomized, controlled, cross-over clinical trial involving 21 patients. Food allergy seems to play an important role in migraine pathophysiology due to a hypothesized inflammatory response.22 Those authors reported that the tailored elimination diet resulted in significant improvements in both migraine and IBS symptoms, possibly by reducing the inflammatory response. Watson et al.23 postulated a hormonal cause relating headache and IBS, since 50% of their IBS patients had headache. A neuroendocrine mechanism as a common pathophysiological mechanism underlying IBS and migraine was also postulated by Soares et al.24 Cole et al.16 found that the likelihood of migraine was 40–80% higher in subjects with IBS than in those without IBS.
Celiac disease
Dimitrova et al.25 showed in 502 patients that the prevalence of migraine was higher in patients with CD and IBD than in healthy controls. Some patients reported significant migraine improvement or resolution after consuming a gluten-free diet, and similar findings were also reported by Gabrielli et al.26 Bürk et al.27 reported on 20 patients with biopsy-proven CD and migraine, finding that a gluten-free diet reduced migraine symptoms in many cases. Alehan et al.28 measured serum tissue transglutaminase IgA (tTGA) antibodies (an indicator for the presence of CD) in their cases (73 children with migraine) and controls (n=147). The prevalence of tTGA antibodies was higher in migraine patients, suggesting a relationship between migraine and CD. The pathophysiology underlying these two conditions remains unclear, but the authors suggested that multiple nutritional, immunological, and inflammatory factors could be involved in triggering migraine attacks.28
Inflammatory bowel disease
In a case-control study, Ben-Or et al.29 examined the prevalence of neurological diseases with GID in 50 patients and 42 healthy subjects, and found that the prevalence of headache was higher in IBD patients than in the control subjects (46% vs. 7.1%). The authors hypothesized an autoimmune/inflammatory mechanism or even malabsorption as possible pathophysiological components. In a cross-sectional study involving 160 subjects (80 with IBD and 80 controls without IBD, with a mean age of 35 years), Cheraghi et al.30 found that the prevalence of migraine was significantly higher in subjects with IBD (21.3% vs. 8.8%, p=0.027). A potential inflammatory pathophysiological mechanism underlying these two conditions was postulated by the authors.
Cyclic vomiting syndrome
Cupini et al.31 observed in a 19-year-old woman with cyclic vomiting syndrome (CVS) and migraine that calcium-channel antagonists such as flunarizine led to a significant improvement of the vomiting syndrome, which led the authors to postulate a common pathogenic mechanism underlying both conditions. A genetic, mitochondrial dysfunction in migraine pathogenesis was postulated by Zaki et al.32 Those authors found mitochondrial polymorphisms to be strongly associated in migraine and CVS patients; CVS is considered a migraine-like condition presenting with similar prodromal symptoms of nausea and vomiting that is responsive to antimigraine medications. Likewise, Christensen et al.33 found that the incidence of migraine headaches was higher in patients with CVS and diabetic gastropathy.
Food allergy
Monro et al.34 described nine patients with food-provoking migraine who were refractory to conventional migraine therapy, and found that dietary exclusion of the offending food resulted in improvement of the migraine. Alpay et al.35 showed in a double-blind, randomized, controlled, cross-over trial involving 30 patients (28 females and 2 males with a mean age of 35 years) that diet restriction in migraineurs based on IgG antibodies reduced the frequency of their migraine attacks (from 9.0±4.4 to 6.2±3.8, p<0.001, mean±SD; p<0.001). The authors speculated that inflammatory mechanisms could play a role in migraine. In a randomized controlled trial, Mitchell et al.36 investigated the use of food elimination based on the presence of IgG antibodies for the prevention of migraine. The 167 participants had migraine and intolerance to at least one foodstuff, and they were randomized to a sham diet (n=83) or the intervention diet (n=84). The authors noted a significant decrease in the number of migraines at 4 weeks, but only a small decrease (not statistically significant) over the 12-week study period.
The relation between migraine and allergens was also investigated by Bektas et al.,37 who enrolled 98 subjects (49 with migraine and 49 healthy subjects, with mean ages of 38.3 and 36.9 years, respectively). The rate of positivity in the allergy test was 55.1% in the migraine group and 32.7% in the control group (p<0.05). Allergy positivity was associated with the frequency but not the severity of attacks. An inflammatory mechanism triggered by allergens leading to the vasodilator phase of migraine and local meningeal inflammation was postulated by the authors.
In 1983, Egger et al.38 reported that 98% of 88 children with severe frequent migraine recovered on an appropriate diet. The authors concluded that since a wide range of foods can provoke an attack, an allergic rather than a metabolic mechanism might be the underlying cause. However, the authors noted that the patients did not show greatly increased levels of IgE or IgE antibodies.
Helicobacter pylori infection
A link between HPI and headache was suggested by Bradbeer et al.4 after they observed that HPI eradication treatment improved the headache but not diffuse abdominal symptoms in a young girl. A particularly interesting finding was that the patient's mother-who was suffering equally from recurrent migraine and GI discomfort-exhibited H. pylori positivity; eradication therapy also led to the resolution of her symptoms. In a case-control study, Hosseinzadeh et al.39 found that the IgG and IgM antibody titers against H. pylori differed significantly between 70 patients with migraine headache and control groups: the optical densities for IgG and IgM antibodies to H. pylori were 60.08±7.70 and 32.1±8.7 in the case group and 21.82±6.20 and 17.6±9.4 in the control group.34 A serotonin-based pathophysiological mechanism underlying both H. pylori infection and migraine was hypothesized by the authors, and they emphasized the need to investigate H. pylori infection actively in migraine patients.
Equally, Yiannopoulou et al.19 suggested a potential relationship between H. pylori infection as an independent environmental risk factor for migraine without aura. In their case-control study, 49 patients with migraine without aura were compared with 51 control subjects without a history of primary headache. They showed that the prevalence of H. pylori infection was significant higher in patients with migraine headache than in controls (p=0.016).
Functional gastrointestinal disorders
Boccia et al.40 conducted a case-control study involving 50 migrainous children with functional GID and 19 control subjects, as well as 10 migrainous children without such disorders and nine healthy children in order to evaluate the effects of gastric stasis on migraine attacks. The gastric emptying time was shortened by using a calcium-channel blocker (flunarizine), which has demonstrated efficacy in the treatment of migraine attacks. Flunarizine treatment resulted in a remarkable improvement of both the GI and headache symptoms; although the clinical findings could not be definitively explained, the authors postulated that ion-channel mutations play a role in the pathogenesis of migraine.
The relationship between gastric stasis and migraine was also evaluated by Aurora et al.41 in a case-control study involving 10 migraine patients along with 10 age- and sex-matched controls. The authors showed that gastric stasis is not only present ictally but also interictally (as measured by gastric scintigraphy). The finding of interictal gastric stasis suggests that nausea in migraine could be related to a central cause rather than to the gastric stasis-migraine may consequently not be an episodic manifestation in an otherwise healthy person, but rather represent the expression of a dysregulated autonomic system. This hypothesis was supported by the findings of Maniyar et al.,42 who performed a positron-emission tomography study in the premonitory phase of nitroglycerin-induced migraine. Their subjects with nausea showed activation in the rostral dorsal medulla and periaqueductal gray, while no activation of these central structures related to nausea were seen in the nonnausea group.
Infantile colic
In a case-control study, Romanello et al.43 investigated the association between migraine and infantile colic in 208 consecutive children aged between 6 to 18 years. Most (72.6%, n=151) of the children with migraine also suffered from infantile colic. The authors postulated a molecular link between these two conditions in the form of CGRP, which is released during migraine attacks and is potentially also involved in the pathogenesis of abdominal pain by causing inflammation of sensory GI neurons. In a multivariable analysis of a population-based, prospective 18-year follow-up cohort, Sillanpää and Saarinen44 showed that infantile colic was significantly associated with a nearly threefold increase in the risk of future migraine without aura.
Endocrine mechanisms
The involvement of CGRP was postulated by Kurth et al.13 in their study of 99 patients with upper GI symptoms and migraine. They found that the prevalence of idiopathic dyspepsia was higher in patients with migraine than in healthy controls (n=488). A nine-year prospective study of 81 obese patients with migraine headache by Gunay et al.9 showed improvement of migraine after bariatric surgery for weight loss. The resolution of migraine symptoms was independent of the improvement of migraine-associated comorbidities. Postoperative endocrine changes or reduction in the adipokine burden were discussed by those authors as potential contributing causes. Amery and Forget conducted a 51-Cr EDTA gut-permeability test, and found that gut permeability was significantly higher in 16 patients with recurrent abdominal pain than in 11 control children and 10 healthy young adults (p<0.0006).45 Recurrent abdominal pain in migrainous children may be due to increased gut permeability allowing compounds to pass the gut-blood barrier that induce cerebral vasoconstriction or exert damaging neuronal effects.
CONCLUSIONS
The clinical and pathophysiological relationships between migraine and GID are intriguing. However, the reported data suffer from great heterogeneity in their gathering and analysis techniques, making a meaningful comparison between studies impossible. Definitive conclusions can therefore not be drawn yet. Furthermore, since migraine is associated with multiple GI conditions rather than one particular GI disease, there is no single pathophysiology interpretation of the association. The pathophysiological mechanisms remain elusive regardless of the GI diseases associated with migraine. Since GI bacteria have repeatedly been implicated in shaping the character of the immune system, including at remote locations,4647 it would be interesting to investigate whether modifying the gut microbiota or even adding probiotics could affect migraines.8 For the time being, from a strict clinical point of view, an awareness of the potential relationship between these two disorders can lead to prompt diagnosis and appropriate therapy for a highly disabling condition.
 XML Download
XML Download