

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transient ischemic attacks (TIAs) are a medical emergency and may precede ischemic stroke that causes permanent neurological deficits. It is important to distinguish true ischemic events from nonischemic etiologies that mimic TIA, particularly in patients who have transient neurological deficits.12 Several neuroimaging-based evaluations and risk stratification scoring systems have been proposed to help identify patients at high risk of true ischemic events.34 However, these scoring systems have limitations in that they are unable to directly demonstrate the corresponding topographical area causing the neurological deficit or the underlying pathophysiology. Diffusion-weighted imaging (DWI) is a sensitive imaging modality that has a high predictive value in diagnosing true ischemic insults. A true vascular event is confirmed when the location of a lesion on DWI corresponds to the area suggested by the clinical presentation, and the lesion pattern on DWI can be used to determine the pathomechanism of TIA.56 However, if the severity or duration of ischemia is not sufficient to cause permanent damage, the DWI findings may be negative, making early diagnosis of true TIA or nonischemic etiologies difficult.7
We previously showed that multimodal magnetic resonance imaging (MRI) increases the probability of finding traces of an ischemic insult, thereby improving the ability of physicians to predict the prognosis of TIA. Furthermore, the prevalence of follow-up DWI lesions was higher in patients with initial perfusion-weighted imaging (PWI) abnormalities than in those without lesions in initial PWI.8 However, that study involved a small population, and we did not separately analyze individuals according to their initial PWI patterns in detail. In the current study, to confirm the kind of perfusion abnormalities than are more indicative of a true vascular event, we performed an additional analysis of a previous prospective cohort and a retrospective validation cohort in conformity with the detailed patterns of perfusion abnormalities.
METHODS
Patients
Two sets of TIA patients were analyzed in the current study: a previous prospective cohort and a retrospective validation cohort. The study was approved by the ethics committee of our center. For the prospective cohort we enrolled 162 consecutive TIA patients who visited Asan Medical Center (AMC) within 72 hours of symptom onset between July 2009 and December 2011.8 TIA was defined as a brief loss of brain function (lasting less than 24 hours) that was presumed to be due to cerebral ischemia. In the retrospective validation cohort, we retrospectively investigated records of TIA patients who visited AMC within 72 hours of symptom onset from the AMC Stroke Database. The purpose of this retrospective cohort study was to validate the prospective study using a different large population from the AMC Stroke Database in a more-recent time frame.
The retrospective validation study was performed immediately after completing the prospective cohort study from January 2012 to May 2015. We enrolled DWI-negative TIA patients in whom multimodal MRI [DWI, PWI, and fluid-attenuated inversion recovery (FLAIR) imaging, and magnetic resonance angiography (MRA)] of the extracranial and intracranial arteries had been performed, with follow-up DWI performed after 3 days. Except for the time period, the inclusion criteria for the two cohorts were identical.
In the retrospective validation study, in accordance with the aforementioned prospective cohort study, we assessed vascular risk factors, neurological examination findings, and ABCD2 and ABCD3-I. In our analysis of the retrospective validation series, we also integrated data with the prospective cohort study in order to verify the consistency of the results.
Imaging protocol
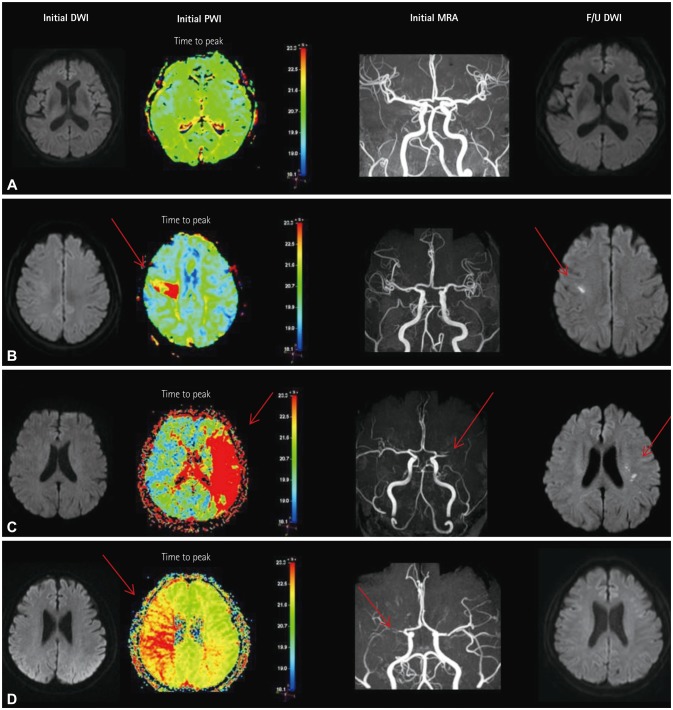
The patients underwent follow-up DWI at 2–4 days after the initial multimodal MRI. The detailed protocol and parameters of MRI have been described previously.8 The MRI images were assessed independently by two stroke neurologists who were blinded to clinical data, with discrepancies resolved by consensus. As shown in Fig. 1, focal perfusion abnormalities were confined to a specific region of the corresponding arterial territories, with an increased signal intensity in the time-to-peak (TTP) map. Territorial perfusion abnormalities were defined as large areas involving one or more vascular territories with increased signal intensity in the TTP map and steno-occlusive lesions in the corresponding arteries.9 The presence of relevant artery stenosis was evaluated from the intracranial and extracranial MRA data. Relevant vessel stenosis was defined as stenosis in the corresponding artery associated with perfusion abnormalities.
Statistical analysis
The demographics and risk factors were compared between patients in the prospective cohort and the retrospective validation cohort. The baseline characteristics of patients with and without a DWI lesion in follow-up MRI were then recorded (the DWI+ and DWI- groups, respectively). Categorical variables were analyzed using chi-squared tests and Fisher's exact tests. Differences in continuous variables were assessed using Student's t-test. Binary logistic regression was used to determine the independent association between the perfusion abnormality and acute lesion in follow-up DWI, and between this abnormality and the stenosis in corresponding arteries. We assessed odds ratios (ORs) of three patterns of perfusion abnormalities for categorical variables (no abnormality, focal abnormality, and territorial abnormality) with no abnormality being used as the reference. The cutoff for significance was a probability value of p<0.05. All statistical analyses were performed using SPSS (version 18.0, SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
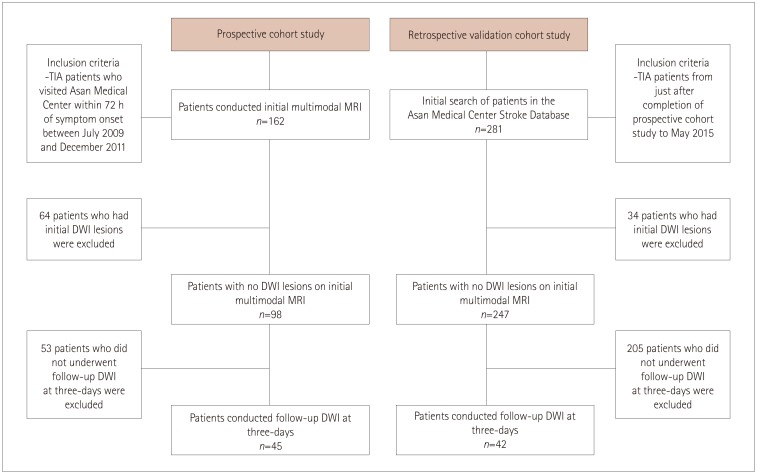
In the prospective cohort, 162 TIA patients visited AMC within 72 hours of a TIA event, of which 98 did not have an acute ischemic lesion on DWI. Forty-five of these 98 patients with DWI-negative TIA underwent follow-up DWI. In the retrospective validation cohort, 281 patients were registered as having TIA in the AMC Stroke Database. Initial multimodal MRI showed no DWI lesions in 247 patients, among which 42 underwent follow-up DWI after 2–4 days (Fig. 2). If patients with an initial DWI lesion were at risk of symptomatic recurrence or recurrent lesions due to a high atherosclerotic burden, they underwent follow-up DWI. Patients with initial negative DWI underwent follow-up DWI only if they agreed to a subsequent MRI evaluation.
Table 1 presents the demographic characteristics in the prospective cohort and the retrospective validation cohort. There were no significant differences between the cohorts except in hypertension, smoking status, and ABCD2 score. However, there was no significant difference based to the ABCD3-I score, which has a higher predictive value than the ABCD2 score. Additionally, according to the associated etiology of TIA using the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification, there were no significant between-group differences.
Comparison according to the presence of new ischemic lesions in follow-up DWI
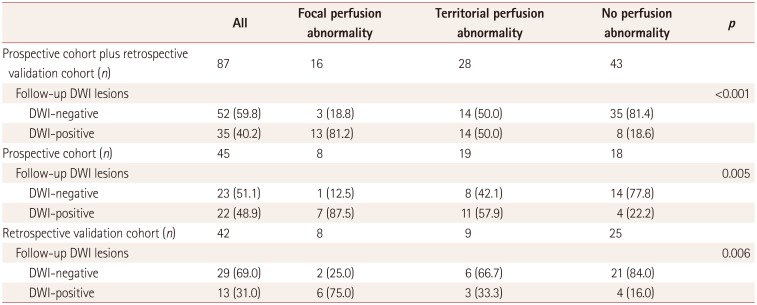
We first analyzed integrated data from the prospective cohort and the retrospective validation cohort. Eighty-seven patients with negative initial DWI lesions were analyzed, among which 35 (40.2%) demonstrated acute lesions in follow-up DWI. Each new acute ischemic lesion in the follow-up DWI corresponded to the location of an initial PWI abnormality. As indicated in Table 2, the initial PWI status differed significantly (p<0.001) between the DWI+ and DWI- groups. Thirteen out of 16 patients (81.2%) with a focal perfusion abnormality demonstrated new lesions in follow-up DWI.
We then conducted separate analyses of the prospective cohort and the retrospective validation cohort, which revealed significant differences in the initial PWI status (p=0.005 and p=0.006, respectively) between the follow-up DWI+ and DWI- groups. In the prospective study, seven of eight patients (87.5%) with a focal perfusion abnormality manifested new lesions in follow-up DWI, while this was present in six of eight patients (75.0%) in the retrospective validation study. In the prospective study, a PWI abnormality demonstrated a high sensitivity (81.8%) and specificity (60.8%) for the detection of follow-up DWI lesions in patients with TIA; the corresponding values in the retrospective validation study were 69.2% and 72.4%. In the integrated data (i.e., from both the prospective cohort and the retrospective validation cohort), PWI abnormality exhibited the largest area under the receiver operating characteristic curve, with a sensitivity of 77.1% and a specificity of 67.3%. On the other hand, the only demographic characteristic that differed significantly between follow-up DWI-negative and follow-up DWI-positive patients with TIA was perfusion abnormality (Supplementary Table 1 in the online-only Data Supplement).
The integrated data were analyzed based on recurrent TIA symptoms (Supplementary Table 2 in the online-only Data Supplement). Recurrent TIA occurred in 6 of 87 patients (6.9%) with TIA who were initially DWI-negative before the follow-up DWI. There were no significant differences in the initial PWI status and follow-up DWI lesions between patients with and without recurrent TIA symptoms.
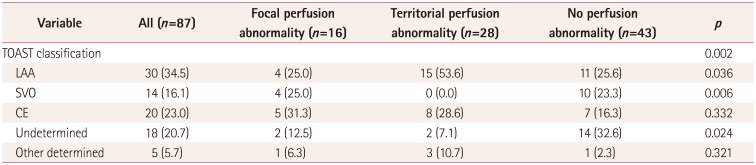
We analyzed the associated etiology of TIA according to initial PWI patterns using the TOAST classification. As indicated in Table 3, territorial perfusion abnormality was significantly associated with large-artery atherosclerosis (p=0.036), while focal perfusion abnormality was significantly associated with small-vessel occlusion (p=0.006). Additionally, no perfusion abnormality was associated with undetermined causes (p=0.024).
Multivariate analysis (Table 4) showed that focal perfusion abnormality [OR=15.1, 95% confidence interval (CI)=3.6–62.9] and territorial perfusion abnormality (OR=3.7, 95% CI=1.2–11.5) were independently associated with DWI lesions at follow-up after adjusting for potential confounders. Logistic regression analysis showed that the follow-up DWI patterns did not differ significantly between the prospective cohort and the retrospective validation cohort (OR=1.9, 95% CI=0.7–5.3, p=0.21).
Focal and territorial perfusion abnormalities and relevant vessel stenosis
After adjusting for confounding variables, relevant vessel stenosis were found to be associated with territorial perfusion abnormalities (OR=31.0, 95% CI=7.0–137.9) but not focal perfusion abnormalities (OR=3.8, 95% CI=0.8–18.3). Acute lesions in follow-up DWI were not associated with the presence of a relevant stenosis (OR=1.8, 95% CI=0.5–7.1, p=0.38) (Table 4).
DISCUSSION
This study investigated the association between perfusion abnormalities and the occurrence of new acute lesions in follow-up DWI. PWI abnormalities, and especially focal perfusion abnormalities, were independently associated with new acute lesions in follow-up DWI after adjusting for potential confounders. In addition, territorial perfusion abnormalities were independently associated with the presence of stenosis in a corresponding artery.
PWI and DWI are being increasing used to help determine stroke mechanisms and subsequent patient management.1011 Although DWI has been shown to be useful for the diagnosis and prognostication of TIA,9 little is known about the role of PWI in the diagnosis of patients with TIA. Benign oligemia is a challenge for all perfusion-imaging modalities,12 and PWI abnormality overestimates true vascular events, making it difficult to use PWI in TIA patients.
We found that the initial PWI abnormalities are significantly associated with follow-up DWI abnormalities. Furthermore, we observed that a focal perfusion abnormality is a stronger predictor than a territorial perfusion abnormality of a new DWI ischemic lesion. We speculate that the mechanism underlying focal perfusion abnormalities predicts a subsequent new ischemic lesion if an ischemic penumbra remains after reperfusion and the no-reflow phenomenon is present.
The penumbra is defined as a region of restricted blood supply in which the metabolism is preserved.13 The ischemic penumbra is vulnerable to progressing to infarcted dead tissue when the delayed perfusion exceeds a certain threshold.14 In other words, if the hypoperfused state persists after recanalization, tissue damage in the ischemic penumbra (which is initially observed to be a DWI-negative but PWI-positive lesion) may evolve into irreversible cell death and damaged tissue, which will manifest as a DWI-positive lesion in the follow-up MRI. Another possible explanation is a no-reflow phenomenon, in which blood flow to the ischemic tissue remains impeded after relieving the major-vessel occlusion.15 Focal ischemia is associated with the local activation of platelets, leukocytes, and coagulation signaling cascades in certain microvessels,1617 and extrinsic microvessel compression by edematous tissue, endothelial cell swelling, and endothelial microvillus formation can also occur.18 In spite of symptomatic improvement after recanalization, the no-reflow phenomenon may contribute to focal ischemia via collapse of the microvascular lumen (Fig. 3).19
Collateral circulation is another phenomenon that may underlie the origin of new DWI ischemic lesions after an initial abnormality in the territorial perfusion. Chronic hypoperfusion due to arterial flow restrictions such as intracranial stenotic disease promotes collateral development.20 Any condition that further reduces the cerebral perfusion may precipitate severe cerebral ischemia. Although reperfusion of ischemic regions improves blood flow, some areas will eventually progress to a true and irreversible infarction (Fig. 3). In addition, patients who suffer a stroke due to large-artery atherosclerosis have a higher risk of lesion recurrence during the early period (within several days) after their stroke.21 Recurrent embolization from a large-artery atherosclerotic burden leads to a hypoperfused state initially and can arouse recurrent ischemic lesions. In summary, we suggest that focal perfusion abnormalities are associated with a remaining ischemic penumbra and no-reflow phenomenon, whereas territorial perfusion abnormalities are associated with chronic hypoperfusion and artery-to-artery embolism. As indicated in Table 3, focal perfusion abnormalities were significantly associated with small-vessel occlusion in this study, while territorial perfusion abnormalities were significantly associated with large-artery atherosclerosis.
Our study was subject to some noteworthy limitations. First, the retrospective design of the retrospective validation study resulted in the prevalence of positive initial DWI lesions being significantly lower than that in the previous prospective study, since we could not strictly exclude patients who had a low probability of a true vascular event in the retrospective study. Second, at the start of the previous prospective study, we planned to perform 3-monthly follow-up FLAIR imaging in all of the DWI-negative patients. However, since this imaging method rarely detected new ischemic lesions in the interim analysis, we decided to perform follow-up DWI after 2–4 days; this was performed in 45 of 98 patients (50%). Third, 80% of the potentially eligible patients were excluded from the retrospective study because they did not receive follow-up DWI, which was due to their initial symptoms already being substantially or fully recovered, resulting in many patients not wanting to undergo follow-up MRI due to the associated economic burden. Fourth, the results of this study will be challenging to generalize due to its limitation of it being performed at a single center. However, the protocol of multimodal MRI including DWI and PWI is the most popular one, and the results must therefore also be applicable to other hospitals. Finally, the prospective cohort and the retrospective validation cohort of this study were analyzed separately. However, there were no significant differences in baseline characteristics between the two groups, and the obtained results were reproducible.
In conclusion, the presence of a focal perfusion abnormality is a strong predictor of new DWI lesions at follow-up in DWI-negative TIA patients. The presence of a corresponding perfusion abnormality in symptomatic TIA patients can provide objective evidence of true vascular events and be used to determine potential mechanisms underlying such events.



 XML Download
XML Download