

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Amyotrophic lateral sclerosis (ALS) is a rapidly progressing and devastating neurodegenerative disorder that leads to death within 3-5 years of diagnosis.1,2 Despite promising preclinical studies, most treatments have failed to improve clinical outcomes.3 Riluzole, a glutamate antagonist, is currently the sole medication approved by the United States Food and Drug Administration for this disorder,4 but its effects on survival are minimal.5
Erythropoietin (EPO) is a well-known hematopoietic cytokine. In vivo and in vitro studies have shown that it might be neuroprotective in various neurological disorders, including Alzheimer's disease,6,7 Parkinson's disease,8 multiple sclerosis, 9 traumatic head injury,10 schizophrenia,11,12 and ALS.13 EPO not only has neurotrophic features14 but it is also an endogenous agent that protects against neurodegeneration.15 The recent evidence for decreased EPO levels in the cerebrospinal fluid of ALS patients16 supports the idea that extrinsic supplementation with EPO could have a therapeutic effect in ALS.
Several studies of the non-hematopoietic effects of EPO have found no serious adverse events even when EPO was administered as a high-dose infusion.17,18 Therefore, we hypothesized that high-dose EPO is neuroprotective in ALS. As a first step, we performed a safety study in which three consecutive monthly infusions were delivered, and we observed the clinical changes after cessation of the EPO injections. We then performed a second case-control study to determine whether EPO could slow the disease progression over the course of 6 months.
Methods
Subjects
All of the subjects were recruited from Hanyang University Hospital between September, 2006 and February, 2010. The inclusion criteria were as follows: 1) diagnosis of either probable or definite ALS based on the El Escorial criteria of the World Federation of Neurology,19 2) age between 29 and 75 years, 3) ALS Functional Rating Scale-Revised (ALSFRS-R) score of ≥20 points, 4) forced vital capacity of ≥50%, and 5) symptom duration of ≤3 years. The exclusion criteria were the presence of 1) hemoglobin at ≥16 g/dL, 2) a baseline blood pressure of ≥150/90 mm Hg, 3) concomitant inflammatory disorders, 4) malignancies, 5) allergies against recombinant human EPO (rhEPO), and 6) history of myocardial infarction or angina. During the treatment and follow-up periods, complete blood cell counts were assessed monthly, and subjects whose hemoglobin increased to more than 15% above the baseline level were excluded from the study.
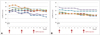
The study timelines are presented in Fig. 1. Protocols and consent forms were approved by the Institutional Review Board for Human Investigation of Hanyang University Hospital. All patients provided written informed consent to participate prior to the start of the study, which was conducted according to the provisions of the Helsinki Declaration.
Study I (a single-arm safety study)
Prior to receiving rhEPO, the natural course of the enrolled patients was assessed over the course of 3 months (lead-in period) using the ALSFRS-R. After this 3 month lead-in period, rhEPO (35,000 IU, Epoetin alpha, Dong-A, Seoul, South Korea) mixed with normal saline (50 mL) was infused intravenously once per month for 3 months. We monitored the ALSFRS-R scores of the subjects for an additional 3 months thereafter to evaluate the effects of discontinuing rhEPO. None of the subjects was allowed to change the dosage of riluzole during the 9 month study period. The ALSFRS-R raters were blinded to both the rhEPO treatment regimen and the clinical history of the subjects.
The primary outcome measures were the differences in the mean changes in the ALSFRS-R scores during the lead-in, treatment, and follow-up periods. The immediate responses and adverse events were evaluated by monitoring the initial 15 subjects at 1 week intervals for 3 months after the initial rhEPO injections using the ALSFRS-R; all individual functional changes after receiving rhEPO were documented.
The safety of the regimen was assessed by evaluating the adverse events related to rhEPO at each visit. Body weight, blood pressure, electrocardiography (ECG) findings, and concomitant medication were documented. Complete blood cell counts, blood urea nitrogen, creatinine, electrolyte, glucose, and liver function tests were checked monthly during the treatment period.
Study II (a controlled extended study)
After demonstrating in study I that a regimen comprising three successive monthly bolus infusions of rhEPO was safe and that their effect disappeared after discontinuation, we designed a case-control extended study that comprised a regimen of six injections. The selection criteria and the treatment regimen were the same as for study I, but there was no lead-in period, the experimental group were administered six injections at a rate of one per month (rhEPO group), and a control group was included.
The baseline patient characteristics and demographics were documented at the initial visit. The control and rhEPO groups used the same criteria and were age- and symptom-duration-matched; subjects were included if their delta FS [progression rate was calculated as ratio, 48-ALSFRS-R score at "time of inclusion"/duration from onset to inclusion (month)] was between 0.3 and 1.3.
The efficacy of extended rhEPO treatment was evaluated by comparing the mean changes in the ALSFRS-R scores between the controls and the rhEPO group during the first (0-3 months) and second-half (4-6 months) periods. During the trial, the subjects in the rhEPO group were asked about adverse events, and routine laboratory tests (as described for study I) were carried out.
Statistical analysis
In study I, as a pilot study, the Wilcoxon signed rank test was used to compare the mean changes in the ALSFRS-R scores during the three periods (lead-in, treatment, and follow-up). In study II, the baseline demographic and clinical characteristics were compared between the two groups using the Mann-Whitney U-test for continuous variables and the chi-square test for categorical variables. A statistically significant change in the ALSFRS-R score between the two groups was determined using the Mann-Whitney U-test. Wilcoxon signed-rank tests were used to assess changes in the laboratory safety parameters.
All reported probability values were two-tailed, and the cutoff for statistical significance was set at p<0.05. Statistical Analysis System (SAS) 9.2 (SAS Institute Inc., Cary, NC, USA) was used for all of the statistical analyses.
Results
Study I (single-arm safety study)
The 26 participants included 17 males, and 8 participants had bulbar onset. Their ages ranged from 39 to 73 years (mean=55.2 years), and the mean ALSFRS-R score at 0 months (i.e., immediately before the rhEPO injection) was 34.0 (range, 23-45 points; Supplementary Table 1).
No serious adverse events were noted. There were no significant changes in the patients' laboratory test results or ECG findings. One subject developed a transient palpitation immediately after receiving the second rhEPO dose that lasted for 3 hours, but there were no other significant ECG findings.
Changes in the ALSFRS-R scores were analyzed. The over-all rate of decline in the ALSFRS-R score decreased during the treatment period (2.6±1.8 vs. 3.7±2.6, mean±SD p=0.02) (Fig. 2A), but reverted to 3.5±2.0 during the follow-up period.
Of the initial 15 subjects who were monitored weekly to evaluate the immediate responses and safety, 2 subjects could not be followed weekly because of travel problems. Among the remaining 13 subjects, 7 experienced subjective functional improvement and an increased sense of well-being that commenced on the second day post-injection. Three subjects exhibited improvements in upper- and lower-limb function (range of motion and motor strength); in addition, two subjects had improved bulbar function and two subjects had improved bulbar and limb function. These changes increased the mean ALSFRS-R score by 1.14 points and appeared to be more pronounced during the first 2 weeks post-rhEPO injection (Fig. 3); however, the effect was not statistically significant. Decreases in fasciculation and drooling, as well as improved respiration, sleep, and muscle tone were also noted. The remaining six subjects did not experience any improvement in ALSFRS-R score, despite reporting improved muscle tone and fasciculation. No acute or chronic serious adverse events were noted in any of the 13 patients.
Study II (controlled extended study)
Sixty ALS subjects were recruited for study II. Three patients (one in the rhEPO group and two in the control group) withdrew prematurely due to travel problems, and another subject in the rhEPO group was excluded because the hemoglobin level had increased to more than 15% above baseline, without other adverse events. Hence, 56 subjects completed the study.
The subjects in the experimental and control groups were matched for age and symptom duration, and their baseline characteristics, such as the symptom duration, delta FS, area of onset, body weight, and use of riluzole, were similar (Table 1). The mean ALSFRS-R scores in the two groups were comparable at baseline, but the mean decrement of ALSFRS-R scores was significantly less in the rhEPO group than in the control group (Fig. 2B). This slowing effect of the disease progression rate continued during the first and second 3 month periods (for months 0-3, 1.8±1.7 vs. 3.1±2.3, p=0.03; for months 4-6, 2.1±2.2 vs. 3.5±2.3, p=0.02).
There were no serious adverse events in the rhEPO group. Two subjects experienced mild headaches, which resolved spontaneously within 2 days. Blood pressure, hemoglobin and platelet counts did not increase in response to the rhEPO injections; other laboratory results also remained within the normal ranges (see follow-up items for safety assessment in Supplementary Table 2).
Discussion
The administration of a monthly high-dose (35,000 IU) intravenous infusion of rhEPO was safe and feasible in ALS patients. Our results suggest that further studies are warranted to confirm the efficacy of this treatment and to investigate different dose schedules via long-term follow-up.
The dose of rhEPO was chosen on the basis of two previous human EPO trials.17,18 An rhEPO dose of 100,000 IU for 3 days in acute ischemic stroke had no ill effects;17 in acute myocardial infarction, 300 µg of darbepoetin alfa (as a single bolus intravenous infusion), which is equivalent to 60,000 IU of rhEPO, also did not lead to adverse hemodynamic or thrombotic events.18 The dose we employed (35,000 IU) corresponds to one-third of the maximal single dose of rhEPO (i.e., 1,800 IU/kg, 108000 IU in a 60-kg subject). However, due to concerns about the potential thrombotic and hypertensive effects of successive rhEPO treatments, we delivered 3 monthly injections to evaluate the safety in the first study and then extended the duration of the treatment period to 6 months in the second study. Despite its established tolerability and safety, rhEPO is known to have serious adverse effects, including reactive polycythemia,20 thrombocythemia,21 malignant hypertension,22 and thrombotic events.23 However, most complications have been attributed to elevated hematocrit and platelet counts and occur mainly during chronic rhEPO treatment.18
As shown in Fig. 2A (study I), the mean rate of decline of the ALSFRS-R score was significantly lower during the treatment period than during the lead-in period, and this beneficial effect disappeared after the discontinuation of EPO treatment. The results of study II were consistent with those of study I: the clinical progression of ALS was significantly delayed in the rhEPO group compared with the controls. We doubt that these outcomes were the result of increased oxygen delivery. As indicated by Supplementary Table 1 and 2, the successive monthly rhEPO infusions did not increase hemoglobin levels. Moreover, although the data were based on only a few patients, the functional improvements were first noted on day 2 after receiving rhEPO (Fig. 3); it is not feasible for a single bolus of rhEPO to increase the red cell mass within only 2 days.24 Thus, we suggest that rhEPO slows the disease progression via other mechanisms, such as anti-inflammation and anti-apoptotic actions, which have previously been demonstrated in animal models of ALS.13 EPO exhibits various cellular functions, including anti-oxidant,25 anti-inflammatory,26 anti-apoptotic, and neurotrophic effects.27 The cause of the neurodegeneration in ALS appears to be neuronal death following oxidative stress and inflammation, which suggests that EPO could be neuroprotective. In addition, previous studies have shown that EPO can prevent neuronal cell death in animal models of neurodegenerative disorders,26,28,29,30 including ALS.13,31
It is interesting that there was an immediate functional improvement in several subjects, although the presence of a placebo effect cannot be excluded. Since this improvement was maintained for 2 weeks, the interval between injections to 2-3 weeks may be decreased in subsequent studies. Although we did not collect data on the short-term immediate responses in all subjects, this information could help to identify the optimal responders to rhEPO. We were unable to establish the factors underlying the differences between the responders and the non-responders. Future studies should attempt to identify the key features of rhEPO responders versus non-responders since this would make it possible to selectively deliver rhEPO to this subgroup.
In contrast to a previous report,32 we demonstrated the potential efficacy of rhEPO in slowing the progression of ALS, although we cannot completely exclude observer bias; however, the second study enrolled a relatively large number of subjects and confirmed the efficacy of rhEPO using the ALSFRS-R scores. Furthermore, we blinded the scorers to the clinical history of the subjects in order to exclude observer bias. The discrepancy in the clinical results between the previous study32 and the present study might arise from differences between the study protocols; the statistical methods used to evaluate the efficacy were different, and that previous study included fewer subjects. The main limitations of our results were that the study did not have a blinded or randomized design and the lack of a placebo in study II. We plan to confirm the efficacy and safety of rhEPO by increasing the frequency of injections in subsequent studies. In addition, we will seek further evidence of the efficacy of this treatment through randomized, double-blind controlled studies and will assess its impact on survival via long-term follow up.
 : time to rhEPO injection,
: time to rhEPO injection,  : time to clinical assessment, ▵: time to measure ALSFRS-R to evaluate primary outcome. ALSFRS-R: amyotrophic lateral sclerosis Functional Rating Scale-Revised, rhEPO: recombinant human erythropoietin.
: time to clinical assessment, ▵: time to measure ALSFRS-R to evaluate primary outcome. ALSFRS-R: amyotrophic lateral sclerosis Functional Rating Scale-Revised, rhEPO: recombinant human erythropoietin.


 XML Download
XML Download