

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The etiologic organism of scrub typhus is an Orientia tsutsugamushi, which is an obligate intracellular bacterium belonging to the family Rickettsiaceae. Scrub typhus is caused by bites of O. tsutsugamushi-infected chiggers and is a seasonal disease occurring mainly during autumn in Korea. Scrub typhus may be considered as one of agricultural work-related zoonosis in rural areas in Korea. The incidence of scrub typhus increases with age. It was known that the peak incidence of scrub typhus was 40.17 per 100,000 persons in those aged 63.3 years old [123]. The proportion of elderly population has been increasing in rural areas, where accessibility to healthcare facilities is relatively poor. In addition, the elderly are vulnerable to scrub typhus, and the incidence of the complications such as cardiovascular disease, acute kidney injury and CNS dysfunction are expected to be high. In elderly patients with scrub typhus, it is very important for physicians to detect complications at the initial presentation. Severe complications of scrub typhus include pneumonia, acute respiratory distress syndrome, myocarditis, hepatic failure, gastrointestinal bleeding, acute kidney injury, encephalitis, and shock, and may cause death. If effective treatment is unavailable or delayed, mortality rates have been reported as high as 30% [456]. The purpose of this study was to identify the risk factors for the prediction of the severe clinical course of scrub typhus and to investigate the differences in the clinical and laboratory findings of hospitalized elderly and non-elderly patients with scrub typhus.
MATERIALS AND METHODS
1. Study design
This study was conducted retrospectively by reviewing the medical records of patients diagnosed with scrub typhus in a university-affiliated hospital. We collected and analyzed the clinical data of scrub typhus patients (18 years of age or older) admitted to St. Vincent's Hospital from January 2001 to December 2017. Patients with fever and typical manifestations of scrub typhus were included in this study. The Institutional Review Board (IRB) of the Catholic University St. Vincent's Hospital assessed and approved all of the study protocols. The requirement for written, informed consent from all patients was waived by the IRB.
2. Definitions
A case of scrub typhus was defined as the patient with 1) fever ≥37.8°C, 2) presence of eschar or positive serologic results, 3) at least one of headache, myalgia, profuse sweating, cough, conjunctival injection, lymphadenopathy, and maculopapular rash, 4) no evidence of any other infection, based on the modified World Health Organization (WHO) Recommended Surveillance Standards [4]. For the serologic test, a passive hemagglutination assay (PHA) or an indirect immunofluorescent antibody assay (IFA) was used. The positive result was defined as a titer ≥1:80 or as a 4-fold or more increase in the following sample [7]. Patients were categorized into elderly or non-elderly group by age, and we defined the elderly as 65 years of age or older people. Patients were also divided into severe and non-severe group according to the presence or absence of complications.
The complications were defined if it showed dysfunction of the following organ systems: 1) Cardiovascular system - presence of any of the following: systolic blood pressure <90 mmHg, myocarditis (defined as elevated creatine kinase-myocardial band isoenzyme above baseline), or abnormal cardiac arrhythmia with no previous history of atrial fibrillation, supraventricular tachycardia, or frequent premature ventricular tachycardia; 2) Respiratory system - presence of any of the following: presence of acute respiratory distress syndrome, defined as the ratio of partial pressure arterial oxygen and fraction of inspired oxygen (PaO2/FiO2) <200 mmHg, with bilateral interstitial infiltration on chest film, or pneumonia with parenchymal lung lesion on chest radiograph; 3) Central nervous system - presence of any of the following: Glasgow Coma Scale ≤12 without other causes, seizure without other causes, or meningoencephalitis; 4) Hematological system - platelet count ≤20×109 /L; 5) Urinary system - presence of acute kidney injury, defined as creatinine ≥2 mg/dL or creatinine change of >0.5 mg/dL/day; 6) Gastrointestinal and hepatobiliary system - presence of any of the following: presence of hepatitis, defined as elevated aspartate aminotransferase (AST) and alanine aminotransferase (ALT) more than fivefold normal levels or increase in serum total bilirubin >2 mg/dL, or gastrointestinal bleeding [478].
3. Data collection
We gathered data about age, gender, underlying disorders, clinical symptoms, physical examination findings, laboratory values, the defervescent time, the length of hospital stay and complications by analyzing the medical records of patients.
4. Clinical outcome measures
Clinical outcome assessments included the defervescent time, the length of hospital stay, clinical cure or failure. The defervescent time was defined as the interval between the time at which the first dose of doxycycline was administered and the time at which the temperature first decreased to <37.5°C and was maintained for ≥24 hours without antipyretics. Clinical cure was defined as the resolution of fever within 5 days after the start of doxycycline therapy. Clinical failure was defined as the persistence of fever without any identifiable cause [9].
5. Statistical analysis
Statistical analysis was done using SPSS version 21.0 (IBM Co., Armonk, NY, USA). Continuous data are expressed as median (interquartile range [IQR], 1Q to 3Q). The continuous variables between the two study groups were compared using the Mann-Whitney test. All categorical variables were compared using Chi-square test or Fisher's exact test. Logistic regression analysis was carried out, including variables with P <0.1 in univariate analysis. Multivariate logistic regression analysis was conducted to identify the independent variables of complicated scrub typhus and a longer hospitalization (≥10 days) in the patients. A P-value <0.05 was considered as statistically significant.
RESULTS
1. Demographic and clinical characteristics
The medical records of 851 patients from 2001 to 2017 were analyzed and total 710 patients were enrolled according to the diagnostic criteria. We retrospectively analyzed the 710 patients and divided these patients into two groups by severe or non-severe group according to the presence of complications or not. Of these, 230 patients (32.4%) were male, the median age of patients was 62.5 years (IQR, 52 to 71) and the number of elderly patients was 312 (43.9%). The number of patients with severe scrub typhus was 168 (23.7%) and the most common complication of severe scrub typhus was hepatic dysfunction (77, 10.8%) followed by pneumonia (51, 7.2%), acute kidney injury (35, 4.9%) and shock (17, 2.4%). Hematologic dysfunction (Platelet ≤20×109 /L) was not observed in this study (Table 1). All patients who were enrolled in this study received doxycycline treatment and survived without sequelae, although the length of hospital stay and the defervescent time after administration of antimicrobial agent were significantly longer in severe group.
Table 1
Types of complications in patients with severe scrub typhus

2. Comparison of demographic and clinical characteristics between severe and non-severe scrub typhus patients
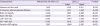
There were no significant differences in sex and age between severe and non-severe scrub typhus groups, but the length of hospital stay and the defervescent time after treatment were significantly longer in severe scrub typhus group. In addition, underlying diseases such as diabetes mellitus and cardiovascular disease were more common in severe group. In the clinical symptoms and signs, the frequency of rash in non-severe group was higher than in severe group. However, there was no significant difference in eschar, headache, nausea or vomiting, cough, dyspnea and conjunctival injection between two groups. In the laboratory result, there were significant differences in several factors between two groups. In the severe scrub typhus group, the levels of initial platelet (normal: 150 - 450×109/L) and serum albumin (normal: 3.3 - 5.2 g/dL) were lower and the level of blood urea nitrogen (BUN) (normal: 8.0 - 23.0 mg/dL), creatinine (normal: 0.5 - 1.2 mg/dL), aspartate aminotransferase (AST) (normal: <50 IU/L), alanine aminotransferase (ALT) (normal: <50 IU/L), C-reactive protein (CRP) (normal: 0 - 0.3 mg/dL), adenosine deaminase (ADA) (normal: 7.0 - 20.0 IU/L), lactate dehydrogenase (LDH) (normal: 140 - 271 U/L), alkaline phosphatase (ALP) (normal: 30 - 120 IU/L) and ferritin (normal: 10 - 260 ng/mL) in the blood were higher than those of non-severe group (Table 2). Multivariate logistic regression analysis showed that BUN ≥20 mg/dL (odds ratio [OR] = 3.038, 95% confidence interval [CI] = 1.891 - 4.897), ADA ≥100 IU/L (OR = 2.207, 95% CI =1.171 - 4.160), pulmonary edema or pleural effusion (OR = 2.145, 95% CI = 1.312 - 3.507), LDH ≥500 U/L (OR = 2.180, 95% CI = 1.440 - 3.300), ALP ≥400 IU/L (OR = 2.130, 95% CI = 1.410 - 3.216), ferritin ≥500 ng/mL (OR = 1.547, 95% CI = 1.040 - 2.301) and absence of skin rash (OR = 1.697, 95% CI = 1.103 - 2.611) were independently associated with severe scrub typhus patients (Table 3).
Table 2
Clinical characteristics and laboratory finding of severe and non-severe scrub typhus patients

WBC, white blood cell; AST, aspartate aminotransferase; ALT, alanine aminotransferase; BUN, blood urea nitrogen; Tx, treatment; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; ADA, adenosine deaminase; LDH, lactate dehydrogenase; ALP, alkaline phosphatase; GTP, gamma-glutamyl transpeptidase.
aValues are presented as median (interquartile range).
bValues are presented as number (%).
cMann-Whitney U test.
dPearson chi-square test or Fisher exact test.
Table 3
Related factors for complicated scrub typhus by multiple logistic regression
3. Comparison of clinical outcomes of elderly and non-elderly scrub typhus patients
There was no significant difference in the incidence of severe scrub typhus between elderly and non-elderly patients. However, the proportion of patients with hepatic dysfunction was significantly higher in the non-elderly group, and the proportion of patients with acute kidney injury, respiratory dysfunction and cardiovascular dysfunction was significantly higher in the elderly group (Table 4). Between elderly and non-elderly scrub typhus groups, there were no significant differences in sex and the defervescent time after treatment, but the length of hospital stay (8 days, IQR 6-10 vs. 7 days, IQR 5-8, P <0.001) was significantly longer in elderly group. Underlying diseases such as diabetes mellitus (69/312, 22.1% vs. 33/398, 8.3%, P <0.001) and cardiovascular disease (147/312, 47.1% vs. 66/398, 16.6%, P <0.001) were also more common in elderly group. In the clinical symptoms and signs, the occurrence rates of rash and eschar were similar between the two groups, however the frequency of altered mental status (2.9% vs. 0.3%, P = 0.006) was higher in the elderly, and those of headache (35.9% vs. 53.0%, P <0.001), and splenomegaly (15.9% vs. 30.3%, P = 0.001) were higher in the non-elderly. In the laboratory results, the proportion of patients with abnormal liver function was significantly higher in non-elderly patients than in elderly patients. However, in elderly patients, the levels of serum BUN, creatinine, CRP and ADA were significantly higher and the level of serum albumin was significantly lower than those in non-elderly patients.
Table 4
Comparison of complications in elderly and non-elderly scrub typhus patients
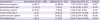
4. Clinical significance and risk factors of a prolonged hospitalization in scrub typhus patients
We divided the scrub typhus patients into two groups by the length of hospital stay (LOS): group 1, LOS ≥10 days (129 patients, 18.2%) and group 2, LOS <10 days (581 patients, 81.8%). In group 1, the proportion of the elderly patients and the patients with cardiovascular diseases were higher than those in group 2. In addition, the proportions of patients with hypoalbuminemia, hyperbilirubinemia, ADA ≥100 IU/L, ferritin ≥500 ng/mL and abnormal kidney function were also higher in group 1. Multiple logistic regression analysis for estimating independent variables on a longer hospitalization(≥10 days) demonstrated that absence of skin rash, pulmonary edema, pleural effusion, serum creatinine ≥1.5 mg/dL, total bilirubin ≥1.5 mg/dL, ADA≥100 IU/L and ferritin ≥500 ng/mL were significantly associated (Table 5).
Table 5
Factors related to a longer hospitalization (≥10 days) in scrub typhus

LOS, length of hospital stay; OR, odds ratio; CI, confidence interval; AST, aspartate aminotransferase; ALT, alanine aminotransferase; BUN, blood urea nitrogen; CRP, C-reactive protein; ADA, adenosine deaminase; LDH, lactate dehydrogenase; ALP, alkaline phosphatase; GTP, gamma-glutamyl transpeptidase.
aPearson chi-square test or Fisher exact test.
DISCUSSION
Scrub typhus is a seasonal disease that occurs mainly during the month of October and November in Korea. Common clinical manifestations of scrub typhus include fever, eschar, maculopapular rash, headache, myalgia, cough, nausea, vomiting, conjunctival injection, and dizziness. These clinical characteristics of scrub typhus are non-specific and similar to those of other febrile illnesses, making the diagnosis of scrub typhus difficult [56]. In recent years, several studies on early diagnosis and analyzing risk factors of scrub typhus were reported. The reported predictors of complicated scrub typhus include old age, absence of eschar, hypoalbuminemia (≤3.0g/dL), leukocytosis (>10,000/mm3), albuminuria and crepitation heard on auscultation [41011].
In this study, we retrospectively analyzed 710 patients and divided them into two groups, severe or non-severe group, according to the presence of complications. The number of patients with severe scrub typhus was 168 (23.7%), and the most common complication of severe scrub typhus was hepatic dysfunction, which were different from the results of the previous study reported by Kim et al in Korea. This difference may be due to disparity in epidemiologic feature of each study such as job and life style of patients, the proportion of the elderly, and prevalent O. tsutsugamushi genotypes in the geographic region of each study [11]. In this study, there was no significant difference in the proportion of the elderly and absence of eschar between severe and non-severe groups, unlike the results of previous reports. However, there was a significant difference in the proportion of patients with skin rash between two groups, and the absence of skin rash was independently associated with severe scrub typhus by multivariate logistic regression analysis. In scrub typhus patients without rash, the diagnosis and treatment of scrub typhus can be delayed, which may increase the incidence of complicated scrub typhus. Therefore, in epidemic areas during prevalent seasons physicians should consider the possibility of scrub typhus even in patients with undifferentiated fever without skin rash.
In the laboratory result of scrub typhus patients, the median level of serum ADA activity in scrub typhus patients was 67 IU/L (IQR 54.9 to 81.1), which was significantly higher than normal range, as known diagnostic value of ADA in scrub typhus [1213]. It has been reported that the serum ADA activity is increased in diseases associated with cellular system stimulation such as typhoid fever, tuberculosis and infectious mononucleosis and enhance the proliferation and differentiation of T-cell [14]. However, there was no report to reveal definitely that serum ADA activity was associated with disease severity of scrub typhus. In this study, the serum ADA activity more than 100 IU/L was associated with scrub typhus with complications by multiple logistic regression analysis. Therefore, the serum ADA activity is expected to be useful for predicting the severity of scrub typhus. In this study, the quantitative level of serum ferritin was also shown to be associated with disease severity of scrub typhus. Ferritin is one of the acute phase proteins involved in viral- and bacterial-induced inflammation. Recently, several studies reported that the elevated level of serum ferritin was strongly associated with disease severity in Dengue virus or Epstein Barr virus infection [151617]. However, it was not known that the increased level of serum ferritin was associated with severity of scrub typhus.
It was already known that ADA and ferritin stimulate several immune cells and induce the secretion of various cytokines [181920]. Kaljas et al. reported that ADA regulates the level of TNF-alpha secreted by activated monocytes by controlling the concentration of extracellular adenosine [2122] and Kim et al reported that serum TNF-alpha level was higher in the severe scrub typhus group than those in the mild group and TNF-alpha level can be used to predict the severity of scrub typhus [10]. Because these immune responses of the host with infectious disease can affect the clinical course of the disease, we may predict the severity of scrub typhus by measuring the level of serum ADA and ferritin in scrub typhus patients. In future, more researches on the immune responses associated with ADA and ferritin are required to clarify the role of the cellular immune response in scrub typhus patients.
In a meta-analysis of 89 studies (19,644 patients with scrub typhus), old age(>65 years) in scrub typhus was related to fatal outcome [23]. In this study, the incidence of severe scrub typhus was not significantly different between the elderly and non-elderly patients, however the types of complication were significantly different. In the younger patients, hepatic dysfunction involved with macrophage infection was mainly present, and the occurrence of splenomegaly was also significantly more frequent than in the elderly group. However, cardiovascular, pulmonary, CNS and renal dysfunction involved with endothelial infection occurred more frequently in the elderly group [24]. This result can be associated with underlying diseases of each group. In elderly group, diabetes mellitus and cardiovascular diseases were more common than in non-elderly patients, but chronic hepatic diseases were more common in non-elderly patients. In this study, it was found that old age as 65 years or more was one of the risk factors associated with a longer hospitalization for more than 10 days. Furthermore, multivariate analysis indicated that pulmonary edema or pleural effusion, total bilirubin ≥1.5 mg/dL, creatinine ≥1.5 mg/dL, ADA ≥100 IU/L, Ferritin ≥500 ng/mL and absence of skin rash were independently associated with a longer hospitalization (≥10 days) of scrub typhus patients. Most of them were similar to risk factors for disease severity of scrub typhus.
This study includes some limitations. First, this study was limited due to its retrospective design. Second, the risk factors of mortality could not be assessed, because there were no deaths among enrolled patients according to the diagnostic criteria. Third, more standard diagnostic methods such as PCR or culture were not available in this hospital. However, the diagnosis of scrub typhus was based on guideline as recommended by the World Health Organization, and all of the patients were clinically confirmed by an infectious disease specialist.
In conclusions, absence of skin rash, the elevated serum ADA and ferritin levels were identified as the predictive factors of complicated scrub typhus in this study. Therefore, these predictors could be useful for the early diagnosis of complicated scrub typhus. Further studies on ADA and ferritin may provide a better understanding of the immune response in scrub typhus patients.
 XML Download
XML Download