

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Infections caused by multidrug-resistant Gram-negative bacteria have been on the rise, so treatment of these infections has become a serious problem due to the absence of antibiotics effective for these bacteria [1]. Colistimethate sodium (CMS), which has been used in the past and has been rarely used for treatment due to nephrotoxicity, has been increasingly used again with the rising number of infections due to these multidrug-resistant gram-negative bacteria [23]. Acute kidney injuries (AKI) are the major adverse effects of administering CMS and are associated with increased mortality [456], especially in patients with severe infections [7].
Despite medical breakthroughs, the prevalence and mortality associated with acute renal impairment remain high. The most important factor in the increase of mortality due to AKI is the absence of biomarkers that can detect renal damage early in patients with AKI and such absence leads to delays in treatment [8]. Therefore, discovering early biomarkers that enable early detection of acute renal damage in patients receiving CMS treatment is necessary.
In current clinical practice, AKI is typically diagnosed by measuring serum creatinine. However, creatinine does not demonstrate actual changes in the renal function during rapid changes [9]. Serum creatinine often has a long half-life and often fails to accurately reflect renal function until a steady state is reached in a matter of days [1011]. Also, the concentration of creatinine is affected by several other causes besides glomerular filtration rate, for example catabolism, rhabomyolysis, certain antibiotics, hemodilution, and muscle mass [10].
Neutrophil gelatinase-associated lipocalin (NGAL) has been actively studied as a biomarker for the early detection of acute renal damage in place of creatinine [121314]. NGAL is a large glycosylated protein monomer synthesized in renal tubular epithelial cells. Following acute tubular damage of various causes, NGAL is greatly increased in the blood and urine [12]. Previous studies suggest that plasma NGAL level can predict the occurrence of AKI earlier than serum creatinine can in patients with sepsis or patients with burn [1516]. Previous studies suggest that plasma NGAL level can predict the occurrence of AKI earlier than serum creatinine can in patients with sepsis or patients with burn [1315].
Patients with suspected infections have a particularly high risk of developing AKI. If AKI can be discovered early, physicians will be able to avoid the risk factors that could cause additional damage and proceed with treatments to prevent the progression of renal damage.
We hypothesized that plasma NGAL level may be an early biomarker of AKI in CMS-treated patients. The objective of this study was to determine whether NGAL represents an early biomarker to predict AKI in CMS-treated patients.
Materials and Methods
1. Study setting and patients
This study was performed at Kangdong Sacred Heart Hospital, a 640-bed secondary-level university hospital located in Seoul, South Korea. This study was reviewed and approved by the Institutional Review Board of Kangdong Sacred Heart Hospital.
All patients aged ≥20 years who received intravenous CMS between March 1, 2014 and November 30, 2015 were eligible. We obtained written informed consent from every patient before enrollment. If the patients suffered from a confusional state or had cognitive impairment, informed consent was obtained from the patients’ family members or legal guardian. Patients were excluded if they received CMS for <72 hours, were on renal replacement therapy (RRT) prior to the CMS initiation, had a creatinine clearance ≤60 mL/min at CMS initiation, or did not have serum creatinine and NGAL measures for 7 days after CMS initiation. However, patients who did not complete the entire course of the study were eligible if they developed AKI during the therapy.
2. Study design
This was a prospective cohort study. From the viewpoint of treatment, the study was observational, without any deviation from standard practice. The indication for treatment was the responsibility of the medical staff assisting the patient, without any interference from the research team. Similarly, decisions to discontinue or reduce the dose of CMS were the prerogatives of the primary care team. The colistin preparation routinely used in our hospital (colistin sulfomethate sodium; Sam Chun Dang Pharm. Co., Ltd. Seoul, Korea) was administered to the patients by their treating physicians.The CMS used in this study was supplied as 150 mg of colistin base activity per vial. CMS dosing was driven by an institutional protocol, based on a dosing algorithm developed for critically ill patients [17]. The CMS dose was titrated to creatinine clearance (CrCl) and to a target steady-state concentration of 2.0 mg/L, according to the following equation: daily dose (colistin base, mg) = 2.0 × [(1.5 × CrCl) + 30] [17]. Loading doses were not recommended.
After written informed consent was obtained, blood samples for NGAL were obtained at baseline and at frequent intervals for 7 days after CMS initiation (at 8 hours after CMS initiation, every 8 hours for 3 days, and every 12 hours for 4 days). Serum creatinine was measured at baseline and routinely monitored at least once a day during the study period.
3. Laboratory methods
Venous whole blood was collected in tubes containing ethylenediaminetetraacetic acid (EDTA) as an anticoagulant, and the samples were processed within an hour of drawing the blood. All plasma NGAL measurements were performed using a Triage platform on a 9-assay fluorescent microfluidic protein chip. The Triage NGAL test (Alere Medical Inc., San Diego, CA, USA), a point-of-care system designed for bedside use, has an on-board algorithm capable of reporting a test result within 15 to 20 minutes. Briefly, EDTA-anticoagulated whole blood was supplied to the assay device, which contains an NGAL specific monoclonal antibody conjugated to a fluorescent nanoparticle. The specimen moves through an integrated filter to separate cells from plasma. The plasma then reconstitutes the fluorescent antibody conjugated detection nanoparticles and flows down the diagnostic lane via capillary action. The device is then inserted into the Triage Meter, a portable fluorescence spectrometer. Quantitative measurements of NGAL concentration are displayed on the meter screen and printout after approximately 15 minutes. The plasma NGAL lower and upper limit of detection was 15 ng/mL and 3,000 ng/mL, respectively [18].
4. Study variables and definitions
Clinical data were extracted from the patients’ medical records and entered into a database. The following information was collected: dates of administration and CMS prescription; underlying diseases; site of infection; causative bacteria; concomitant nephrotoxic drugs (radiocontrast agents, non-steroidal anti-inflammatory drugs (NSAIDs), vancomycin and aminoglycosies); Acute Physiology and Chronic Health Evaluation (APACHE) II score at the beginning CMS treatment; presence of sepsis; and serial serum creatinine levels. Baseline estimated glomerular filtration rate (GFR) was calculated by the abbreviated Modification of Diet in Renal Disease equation.
Severe sepsis, septic shock, and type of infection were defined according to standardized criteria. The severity of comorbid conditions was classified by the McCabe classification [19].
AKI was defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria as follows: an absolute increase in the serum creatinine level by 0.3 mg/dL within 48 hours or an increase in the serum creatinine level to 1.5 times the baseline level which is known or presumed to have occurred within the prior 7 days [20]. AKI was staged according to KDIGO as follows: stage 1, defined as an absolute increase in the serum creatinine level to ≥0.3 mg/dL or an increase in the serum creatinine level to 1.5 – 1.9 times the baseline level; stage 2, an increase in the serum creatinine level to 2.0 – 2.9 times the baseline level; and stage 3, an increase in the serum creatinine level to ≥3.0 times the baseline level or the initiation of dialysis. AKI was assessed daily until the end of CMS therapy. The definition of AKI in terms of plasma NGAL has not yet been defined.
5. Outcomes
The primary study object was to determine whether AKI could be detected earlier based on plasma NGAL levels compared with the conventional serum creatinine criteria. The sensitivity, specificity, and diagnostic accuracy of plasma NGAL values for detecting AKI caused by CMS were evaluated.
6. Statistical analysis
A linear mixed model was used to analyze repeated measures of plasma NGAL levels. A two-sample t test or Mann-Whitney rank sum test was used to compare continuous variables, and the chi-square or Fisher’s exact test was used to compare categorical variables. Pearson’s correlation test was conducted to evaluate the relationship between plasma NGAL level and other clinical characteristics. To measure the sensitivity and specificity of plasma NGAL measurements at different cutoff values, a conventional receiver operating characteristic (ROC) curve was generated, and the area under the curve (AUC) was calculated to quantify the accuracy of NGAL as a biomarker. The cutoff values were selected to maximize the sensitivity and specificity of NGAL. An AUC of 0.5 is considered to be no better than expected by chance, whereas as a value of 1.0 signifies a perfect biomarker. Univariate and multivariate multiple logistic regression analyses were conducted to assess predictors of AKI. All reported P values were two-tailed, and a P <0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
1. Patient population
Between March 2014 and November 2015, 109 patients were treated with CMS because of various infections. Of these patients, 86 patients were excluded (nine underwent RRT prior to CMS, 15 had creatinine clearance ≤60 mL/min, one was aged <18 years, 16 received CMS treatment for <72 hours, and 45 did not provide informed consent); therefore, 23 patients met the inclusion criteria. Their mean age was 61.3 ± 16.1 years, and 65.2% were male. The characteristics of the study patients at the start of CMS treatment are shown in Table 1. The prevalence of neurologic disease was 47.8%, 34.8% of patients had diabetes, and 30.4% had a malignancy. Patients were treated for pneumonia (52.2%), soft tissue and bone infection (21.7%), and catheter-related blood stream infection (13.0%). At baseline, the plasma NGAL level (mean ± SD) was 233.0 ± 135.4 ng/mL; in five patients, the baseline plasma NGAL level was above 300 ng/mL. The baseline leukocyte level was 14198.7 ± 6544.7/mm3. The mean APACHE II score was 18.2 ± 6.7. No relationship was detected between the APACHE II score and basal plasma NGAL level (Pearson’s correlation coefficient -0.070, P = 0.750). In addition, there was no relationship between the basal leukocyte level and basal plasma NGAL level (Pearson’s correlation coefficient -0.242, P = 0.267). Colistin was administered to the patients in accordance with the aforementioned equation while taking their GFR and BSA into consideration. The mean daily administered colistin dose was 328.65 ± 87.40 mg/day, without a significant difference between the groups (Table 1).
Table 1
Demographic and clinical characteristics of patients who received colistimethate sodium
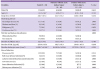
Patients were infected with Acinetobacter baumannii (16/23, 69.6%), Pseudomonas aeruginosa (5/23, 21.7%), and carbapenem-resistant Enterobacteriaceae (2/21, 8.7%). There were no differences in the causative organisms or infection sites between the two groups. Table 2 shows severity of the infection at the time of CMS treatment and the nephrotoxic agents concomitantly administered during the study period.
Table 2
Comorbid conditions of patients treated with colistimethate sodium
The most frequently used nephrotoxic agents were radiocontrast agent (30.4%) and vancomycin (13.0%). Three patients (13.0%) had severe sepsis and two patients (8.7%) had septic shock at the start of CMS treatment. The mean duration of CMS treatment in all patients was 8.35 ± 4.228. AKI occurred in 13 patients (56.5%). The patients were classified into AKI-incidence group and AKI-non-incidence group as defined. There was no notable difference in the demographic factor and the severity of infection between the two groups (Table 1, and 2).
2. Diagnosis of AKI using serum creatinine and plasma NGAL
According to our definitions of acute kidney injury, 13 patients (56.5%) developed AKI. The mean time to onset of AKI after CMS initiation was 78.15 ± 30.49 hours (median, 84 hours; range, 36–144). Analysis of AKI severity revealed that, in the patients with AKI, most (6/13) developed stage 1, four patients had stage 2, and 3 patients had stage 3 AKI. No patients required RRT. There were no significant differences in baseline estimated GFR between patients with AKI and patients without AKI (P = 0.789). Baseline creatinine levels were similar in both groups. Patients who presented with AKI on the fourth day showed distinctive elevation in creatinine concentration (P ≤0.05 for all other time points). The highest creatinine level measured in patients treated with CMS was 3 mg/dL.
During the 7-day study period, plasma NGAL was measured 355 times for prediction of AKI in 23 patients. There was no statistical difference in the baseline NGAL values between the two groups regardless of the occurrence of AKI (Table 1). At baseline, plasma NGAL was 264.0 ± 167.3 ng / mL in patients with AKI and 192.7 ± 65.3 ng / mL in patients without AKI (P = 0.218). Among the 5 patients with baseline NGAL levels exceeding 300 ng/mL, one belonged to the non-AKI group whereas the remaining 4 belonged to the AKI group.
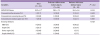
The significant difference of mean plasma NGAL level between patients with AKI and without AKI were shown from 56 hours after CMS treatment (Fig. 1). A multivariate analysis was conducted with the factors that can influence NGAL levels or AKI occurrence in addition to CMS. As severe sepsis and septic shock were found to influence NGAL levels in other studies, APACHE II score was included in the regression model [21]. Moreover, as the severity of infection, age, and nephrotoxic drugs can influence the occurrence of AKI, they were included in the regression analysis. Table 3 shows the results of multivariate analysis. The plasma NGAL level was significantly different between the two groups and was predictive of AKI 56 hours past from CMS treatment initiation even when calibration was done (adjusted odds ratio = 1.012, 95% confidence interval [CI], 1.001 to 1.024, P = 0.035).
Figure 1
Mean plasma NGAL level during 7 days of treatment with intravenous CMS. All values are expressed as the mean ± two times standard error.
CMS, colistimethate sodium; Cr, creatinine; NGAL, neutrophil gelatinase-associated lipocalin.
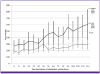
Table 3
Multivariate analysis of factors affecting acute kidney injury in patients receiving colistimethate sodium

The ROC curve method was performed to evaluate the diagnostic value of plasma NGAL for predicting AKI. The plasma NGAL level exceed 285 ng/mL at 56 hours after CMS treatment s was shown to be a powerful predictor of AKI, with an AUC of 0.796 (95% CI, 0.609 to 0.983; P = 0.017). Compared to serum creatinine, which takes 78 hours after initiation of CMS treatment for the prediction of AKI, plasma NGAL enables AKI prediction 22 hours earlier (P = 0.035).
3. Predictive value of plasma NGAL for AKI detection in CMS-treated patients
Sensitivity and specificity were highest when the cutoff value was 285 ng / mL among the plasma NGAL values measured at 56 hours after initiation of CMS treatment.
Using a cutoff plasma NGAL level of 285 ng/mL, 10 patients with AKI were detected (Fig 2). Using this cutoff, we found true-positive results in nine patients, false-positive results in one patient, false-negative results in three patients, and true-negative results in three patients. At 56 hours after initiation of CMS therapy, a cutoff value of 285 ng/mL had 69.2% sensitivity, 90.0% specificity, 90.0% positive predictive value, and 69.2% negative predictive value.

Discussion
In this study, we found that plasma NGAL could serve as a biomarker that can predict renal injury early in patients receiving CMS. This is reportedly the first study evaluating plasma NGAL in the clinical setting of potentially nephrotoxic colistin treatment.
The choice of therapeutic agents for the treatment of multidrug-resistant gram-negative bacteria, especially carbapenem-resistant Gram-negative bacteria has been very limited until now. CMS is currently an important antibiotic in the treatment of infections caused by these multidrug-resistant bacteria. However, the nephrotoxicity that occurs in the course of CMS administration remains a critical limitation and one of the important reasons for discontinuing administration [22]. Although the mechanism of CMS causing nephrotoxicity has not yet been determined, it is assumed that one of the essential mechanisms is acute tubular necrosis [22]. It is known that the nephrotoxicity occurring during the treatment of CMS is usually dose-dependent and is relieved by the rapid cessation of CMS and proper hydration following the detection of nephrotoxicity [68].
Evaluation of NGAL in these patients had potentially enormous significance, especially if we can make timely diagnoses and prevent the development AKI in this highly vulnerable patients group.
NGAL expression is included in injured epithelia; for example, concentrations are raised in the serum of patients with acute bacterial infection, in the sputum of those with asthma or chronic obstructive pulmonary disease, and in bronchial fluid from the emphysematous lung [23]. NGAL as new biomarkers that enable early diagnosis and prognostic stratification of AKI before serum creatinine increment have been developed to date. Several studies suggest that NGAL is a promising early biomarker of AKI [131524]. In several studies, NGAL level was found to be a predictor of AKI. However, as different studies have used different measurement timings or cutoff values for NGAL to predict AKI, no consensus has been reached on the cutoff value [13151621]. The cutoff value of NGAL varied widely form 150 ng/mL to 470 ng/mL [151621].
In this study, serum creatinine started to rise after 96 hours of CMS therapy in 5 out of 13 AKI patients. Thus, following the current AKI diagnostic criteria that is based on creatinine, AKI can be detected a few days after the kidney damage occurs.
We demonstrated that the plasma NGAL level was able to detect AKI earlier than serum creatinine in patients receiving CMS therapy. The plasma NGAL cutoff level of 285 ng/mL showed an AUC of 0.796 (95% CI, 0.609 to 0.983; P = 0.017) for the diagnosis AKI. Using NGAL as a biomarker for the early detection of AKI will enable the detection of deterioration in renal function a day earlier compared to the use of creatinine.
Our study has the following limitations. First, further research is needed to generalize the result of this study since it is a single-center study. The population used was small. Among 109 patients who received CMS treatment, only 23 patients were included in this study. The study is not free from selection bias as only 23 of the subjects participated in this study. Most of the 45 people who did not consent to participate did not do so because of the frequent tests required to measure NGAL levels. Moreover, some could not participate because they already received colistin therapy before participation in this study. Among the 23 participants, 18 were being treated at the intensive care unit at the time of participation. The infections in these patients were not less severe than those in the 45 patients who did not consent to participate. Patients with AKI were included in the study if NGAL measurements taken before the onset of AKI were available even if the NGAL levels were not measured for 7 days. This may have led to selection bias. Colistin administration was discontinued in 7 of the 13 patients with AKI. Plasma NGAL level was measured in all the 7 patients for 24 to 48 hours after the cessation of colistin administration. Thereafter, all the patients showed signs of recovery from AKI. As the purpose of this study was to evaluate the effectiveness of NGAL level as an early predictor of AKI, patients whose NGAL levels were measured until after the occurrence of AKI were included. A linear mixed model was used for the analysis to adjust for missing NGAL measurements.
Second, several critically ill patients were enrolled in the study (11 of patients were in the intensive care unit, among whom five had severe sepsis or septic shock). Plasma NGAL level is related to inflammation as well as kidney function [24]. Since NGAL tends to increase in patients with sepsis, this may have affected the outcome of the study [25]. According to studies conducted by Shapiro et al., the average plasma NGAL value of healthy individuals was approximately 150 ng/mL [15]. In the current study, the baseline plasma NGAL levewl, which was 233.0 ± 135.4 ng/mL, was higher than the mean observed in healthy adult [26]. NGAL levels can be influenced by the severity of infection and leukocyte levels [2124]. Other studies also showed that septic AKI patients had higher plasma NGAL levels than non-septic AKI patients [2127]. Some patients in this study also had baseline NGAL levels of >300 ng/mL. However, no significant difference in baseline NGAL level was found between the groups. The severity of infection and leukocyte count, which can influence the NGAL value, also did not differ between patients with AKI and patients without AKI. The groups did not differ in factors that can influence NGAL values. Moreover, plasma NGAL values did not have any correlation with APACHE II score or leukocyte level in this study.
Third, we used serum creatinine level as a diagnostic index of AKI and a variable to evaluate the value of plasma NGAL level in predicting AKI. This may have caused an incorporation bias and have caused the result to favor serum creatinine. However, it was shown in this study that NGAL enables early discovery of AKI better than creatinine. Fourth, only the plasma NGAL was used in this study. In the case of Plasma NGAL, the plasma concentration value is also affected by other factors aside from renal damage (e.g. bacterial infection) [28]. In the case of plasma NGAL, it is secreted in a dimeric form and can be detected not only in the kidney but also in other tissues such as epithelial cells, tumor cells and liver tissue [25]. For currently available plasma NGALs, the monomer form of NGAL, which rises in case of renal failure, cannot be distinguished from dimer forms that can be elevated by other causes. However, Schley et al showed that plasma NGAL had more diagnostic value than urine NGAL [29], and several studies suggest that plasma NGAL may be an early diagnostic marker of AKI [133031]. Fifth, this study was an observation study and the investigators were not involved in the treatment of patients. The total daily dose of CMS was determined based on hospital protocols. However, the dose frequency was determined by the patients’ primary care physicians. Therefore, some patients were given the medication three times a day whereas some patients received it twice a day. The plasma NGAL was measured at regular intervals starting from the initiation of treatment in this study. Thus, internal colistin concentration at the point of plasma NGAL measurement would have varied with the daily dose frequency. Internal colistin concentration would have affected the plasma NGAL value.
Our study has several strengths. The present study provides additional evidence of the utility of NGAL for AKI detection in CMS-treated patients. Other nephrotoxic injuries such as those caused by cardiovascular surgery or administration of radiocontrast agents are considered single events. However, administration of CMS is likely to cause repeated kidney injury. In this clinical setting, it is difficult to prove the predictive capacity of NGAL. In addition, in patients with acute bacterial infections, the ability of NGAL levels to predict the nephrotoxicity of vancomycin [24] or colistin [32], respectively, was compromised. A recent study performed in hemodynamically stable patients treated with amphotericin B showed only moderate diagnostic performance of NGAL for detecting AKI [33]. Finally, we used a rapid point-of-care platform to perform our assays, which facilitated NGAL testing in the general ward and intensive care unit. This technology may facilitate earlier diagnosis of AKI at the patients’ bedside during CMS treatment.
In conclusion, this preliminary investigation showed that AKI coccurance in patients receiving CMS treatment can be predicted earlier with plasma NGAL level than with serum creatinine level. We report the operating characteristics for the NGAL cutoff, these findings are meant to illustrative, and larger studies are required to establish the final cutoff to be used in clinical practice. These findings on CMS induced AKI could serve as a basis for the investigation of biomarkers in the early detection of drug nephrotoxicity in other clinical settings. Our preliminary results should not change the current clinical practice. Studies to evaluate a plasma NGAL oriented treatment strategy may result in a reduction of the incidence of CMS induced AKI in the future.
 XML Download
XML Download