

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Burkitt lymphoma is a cancer of the lymphatic system that is a highly malignant, aggressive and rapidly growing B-cell neoplasm. Burkitt lymphoma can be divided into three main clinical variants: endemic, sporadic, and immunodeficiency-associated [1].
The endemic variant usually involves the facial bones, particularly the jaw, maxilla, and orbit, and, especially in young children, it is associated with Epstein-Barr virus (EBV) infection [2].
In comparison, the sporadic form tends to present in the lymphoid tissues of the gut, often presenting as masses in the Waldeyer ring or the terminal ileum, or even with involvement of abdominal organs with the most involvement of the distal ileum, cecum or mesentery [34] Cases of intestinal intussusception caused by Burkitt lymphoma are rarely reported [5].
Intussusception, the invagination of one portion of the intestine into another, rarely occurs after the first 5 years of life and is classically associated 25 with intense intermittent abdominal pain, vomiting, bloody mucoid diarrhea, and a palpable abdominal mass [678].
Intussusception may become an emergent medical concern if not treated early, as it eventually causes death if not reduced. Urgent diagnosis and reduction is required. In Korea, intussusception caused by Burkitt lymphoma in AIDS patients has not yet been reported. We report a case of multiple jejunal intussusception caused by Burkitt lymphoma in an AIDS patient.
CASE REPORT
A 42-year-old man was brought into our emergency department because of severe abdominal pain. His body temperature was 36.4°C, heart rate was 84 beats per minute, respiratory rate was 16 breaths per minute, and blood pressure was 130/90 mmHg. On physical examination, the abdomen was rigid and whole abdomen tenderness was observed.
Complete blood cell count revealed a white blood cell of 7,220/mm3 (neutrophil 57.5%), hemoglobin of 9.7 g/dL, and platelet count of 299,000/mm3. Chemistry analysis showed 25 IU/L aspartate aminotransferase, 21 IU/L alanine aminotransferase, 0.81 mg/dL total bilirubin, 6.4 g/dL total protein, 3.5 g/dL albumin, 8 mg/dL blood urea nitrogen, 0.65 mg/dL Cr, 97 mg/dL glucose, and 580 IU/L lactate dehydrogenase. The erythrocyte sedimentation rate and C-reactive protein level were 41 mm/hr and 6.84 mg/L, respectively. The patient had been diagnosed with HIV infection in 2010. In November, 2014, the patient’s CD4 (+) T-cell count was 355 cell/mm3 (CDC classification system: Stage 2), and HIV viral load was 156,000 copies/ml. Highly active antiretroviral therapy (HAART) was initiated in April 2015 with abacavir/lamivudine/darunavir/ritonavir. One week before visiting emergency room the patient complained of mild abdominal pain and an upper gastrointestinal endoscopy revealed acute gastric ulcer so a biopsy was performed. One week later, abdominal pain had still not subsided and he visited the emergency department. Plain abdomen X-ray and abdominopelvic computerized tomography (CT) scan were done to evaluate abdominal pain. Abdomen plain X-ray showed multiple air-fluid levels in the dilated loops in a typical configuration of a small bowel obstruction. The CT scan showed a bowel-within bowel configuration at multiple jejunal sites (Fig. 1). Gastrointestinal endoscopic biopsy was performed and the patient was diagnosed with Burkitt lymphoma. Intussusception was thought to be caused by Burkitt lymphoma. Therefore, the patient underwent an emergency operation, during which five intussusception points were found and small bowel segment resection was performed at three sites (Fig. 2). On the surgically resected specimen, the tumor mass involved the submucosa to the subserosa. A typical starry sky pattern was found. Tumor cells were immunoreactive for CD10, CD20, BCL6 and EBER. Ki67 was positive in more than 95% of tumor cells (Fig. 3). However, CD3, CD5, BCL2, Mum-1, ALK and TdT were negative. The patient was in good condition following the surgery.
Figure 1
Abdomen computed tomography scan showed target appearance in the jejunum with severe upstream dilatation of the small bowel (red arrow).
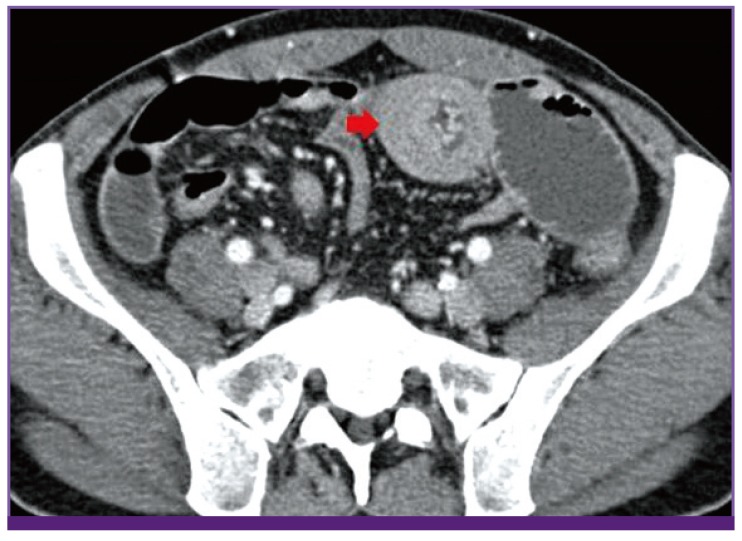
Figure 2
During operation, the intussusception point looked like a mass. Bowel movement and color were intact. Five intussusception points (black arrow) were found and small bowel segment resection was performed at three sites.

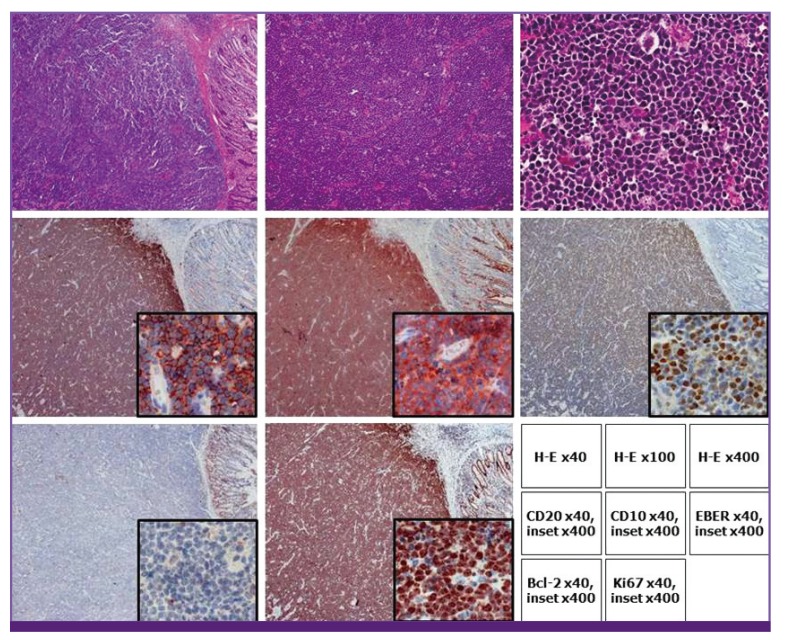
Figure 3
Low power view revealed a bluish mass involving the intestinal wall (H-E, x40).
Scattered benign histiocytes were present in the diffuse tumor cells, giving a “starry sky” pattern (H-E, ☓100). The tumor cells were medium-sized with similar nuclear size to that of histiocytes. The nuclei were round with finely clumped and dispersed chromatin (H-E, ☓400).
The tumor cells showed strong expression of CD20 and CD10. In situ hybridization revealed nuclear Epstein-Barr virus-encoded small RNA (EBER). The tumor cells were negative for bcl-2. Because the tumor had an extremely high proliferation fraction, nearly all of the cells were positive for Ki67.
DISCUSSION
Intussusceptions caused by gastrointestinal (GI) tract non-Hodgkin lymphoma are occasionally reported [59].
Intussusception is believed to initiate from any pathologic lesion of the bowel wall or irritant within the lumen that alters normal peristaltic activity and serves as a lead point that is able to initiate invagination of one segment of the bowel into another [1011]. GI tract non-Hodgkin lymphoma is a rare pathological lead point that can lead to intussusception in older children and in adults.
Non-Hodgkin lymphoma is an important AIDS-defining disease [12]. It is already known that non-Hodgkin lymphoma often occurs in the GI tract of AIDS patients [13]. However, intussusception caused by GI tract non-Hodgkin lymphoma in an AIDS patient has rarely been reported [141516]. Common points of previously reported casess were that AIDS patient complained severe abdominal pain with intestinal intussusception, subsequent emergency operation was performed. And biopsy finding was non-Hodgkin lymphoma. However, no such case has been reported in Korea.
Many diseases can cause abdominal pain in an AIDS patient. Opportunistic infections (Cytomegalovirus, Mycobacterium avium Complex) in severe immunodeficiency can cause abdominal pain. Pain may also be due to other more common etiologies seen in the general population (e.g., appendicitis, diverticulitis). The widespread adoption of ART has been associated with a number of drug-induced side effects, including pancreatitis and the lactic acidosis syndrome, both of which are associated with abdominal pain [1718]. Therefore, acute abdominal pain in an AIDS patient is not easy to diagnose. As in this case, intussusception caused by non-Hodgkin lymphoma can cause abdominal pain in an AIDS patient.
In conclusion, physicians should consider the possibility of intussusception caused by non- Hodgkin lymphoma when examining AIDS patients with acute abdominal pain.
Intussusception may become a medical emergency if not treated early, as it eventually causes death if not reduced. Therefore early diagnosis and differential diagnosis are important in AIDS patients with acute abdominal pain.
 XML Download
XML Download