

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Up to one-third of people with diabetes develop a diabetic foot ulceration (DFU) during their lifetime and over 50% of these ulcerations become infected [1]. Diabetic foot infections (DFIs) are associated with major morbidity, increasing mortality, high costs, increased risk of lower extremity amputation (LEA), and reduced quality of life [2]. In 2014, about 4.8 million Koreans (13.7%) aged 30 years or older suffered from diabetes and nearly one-quarter of Korean adults had prediabetes [3]. A 2011 study on the prevalence and treatment modality of diabetic foot disease (DFD) in Korea performed using data from the Health Insurance Review and Assessment (HIRA) service database revealed a DFD prevalence of 2.9% among 3,763,445 diabetic patients over 19 years of age; 96.4% of patients with DFD received local wound care alone, 2.6% received lower extremity revascularization, and 1.2% received major LEA [4]. Another Korean study on the epidemiology and economic burden of DFD revealed that the incidence (new onset in 2003) of total DFD was 1.2% among 3,911,647 diabetic patients and these patients had very high relative risks for foot amputation (11.7) and ulcer (9.7), higher medical cost, and longer hospital stay, compared with those of non-diabetic patients [5].
DFIs arise mainly from skin ulceration associated with loss of protective sensation (peripheral neuropathy), altered foot architecture, and some forms of trauma[6]. Various types of microorganisms colonize and proliferate on the wounds, which serve as a point of entry, causing tissue damage and resulting in an inflammatory response that is characterized as a clinical infection [6]. These infections can spread contiguously to deep tissues and cause osteomyelitis if they reach bones [6]. Some degree of peripheral arterial disease (PAD) is present in most patients with DFIs and ischemia can lead to necrosis and further failure of the integrity of the surrounding tissue [7]. DFIs together with PAD is a significant predictive factor for LEA [8].
Because DFU is frequently chronic and well-contaminated with a number of microorganisms, it is very important to properly obtain and process the specimens from infected wounds in order to identify the true pathogens and their antimicrobial susceptibilities and, thus, select an appropriate antimicrobial therapy. Staphylococcus aureus and Pseudomonas aeruginosa are important causative microorganisms in DFIs. The distributions of these causative organisms differ geographically and according to the illness duration, prior antibiotic use, and the relevance of nosocomial infections [9]. Recently, the use of inappropriate antibiotics has become a problem for multi-drug resistant bacteria, making the selection of antibiotics difficult [10].
For the successful treatment of DFIs, the administration of antimicrobial agents alone is insufficient without accompanying proper wound care. Nevertheless, the choice of appropriate empirical antibiotics is important to reduce treatment failure, the likelihood of antimicrobial resistance, adverse events, and costs. Guidelines for the choice of empirical antibiotics for DFIs were published by the Infectious Disease Society of America (IDSA) in 2012 and the International Working Group on the Diabetic Foot (IWGDF) in 2016 [611]. Although a Korean guideline for the treatment of diabetic foot, which includes a chapter for DFIs, was published in 2014, there is no mention of specific microbial epidemiology and antimicrobial treatment [12]. For this reason, the IDSA and IWGDF guidelines are still widely used for the treatment of DFIs in Korea. We reviewed articles on the microbiology and antimicrobial therapy of DFIs published in Korea and discussed how to apply these international guidelines to Korean patients with DFIs.
Microbiology
1. Specimen collection
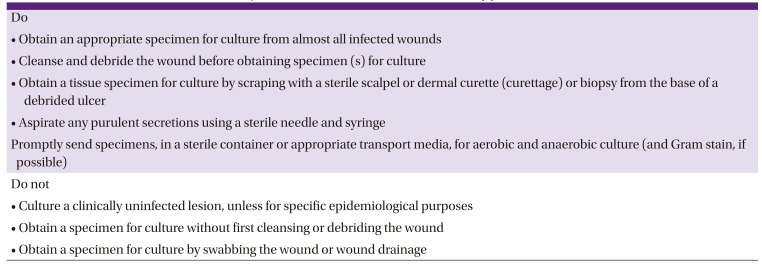
Bacterial culture is not recommended for clinically uninfected wounds except when necessary to determine the presence of multi-drug resistant microorganisms and isolate patients [611]. Because most mild acute infections in patients who have not recently been treated with antibiotics are caused only by aerobic Gram-positive cocci, predominantly S. aureus and/or, to a lesser degree, β-hemolytic streptococci, wound cultures may be unnecessary in these infections [713]. In order to increase the sensitivity of the culture results, it is recommended that samples be taken before empirical antimicrobial therapy or, when antimicrobials are already used, after they could be discontinued for several days and samples collected if the patients are stable [611]. Increasing duration of preoperative antibiotic exposure has been associated with less frequent growth of streptococci and anaerobes and more frequent culture-negative results [14]. Swab specimens are not recommended for culture because of less accurate results; however, aseptically obtained deep tissues are recommended [1516]. The culture results from superficial swab and deep tissue specimens differ [1718]. In particular, the results of superficial swab culture and bone specimens did not correlate well in studies of diabetic foot osteomyelitis (DFO) [192021]. Repeat cultures are usually unnecessary unless the patient is not clinically responding to treatment or if the initial specimen was likely to be contaminated [11]. The IDSA provided recommendations for the collection of specimens for culture from diabetic foot wounds in 2012 (Table 1) [6]. Implementation of guidelines for obtaining specimens for culture from patients with DFIs is cost-saving due to a reduced microbiology laboratory workload, reduced prescription of extended-spectrum antibiotics, and improved quality in the management of DFIs [22].
Table 1
Recommendations for the collection of specimens for culture from diabetic foot wounds (adapted from reference [6])
2. Causative microorganisms
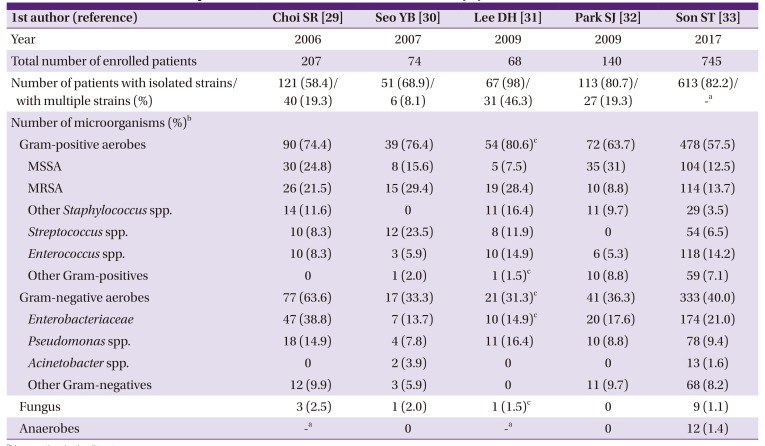
Skin commensals such as coagulase-negative staphylococci, Corynebacterium, or Micrococcus from swab cultures are not usually considered true pathogens, although they may grow repeatedly or from reliable specimens. In most centers, including Korea, S. aureus is the most frequently isolated, and perhaps most virulent pathogen, whether alone or in combination [11]. Aerobic Gram-positive cocci, especially S. aureus and Streptococcus species, are the predominant pathogens in DFIs and usually cause monomicrobial infection in previously untreated acute infections [91423]. Polymicrobial infections, which may include various types of aerobes such as S. aureus, Streptococcus, Enterococcus, Enterobacteriaceae, and Pseudomonas commonly appear in deep or chronic wounds [1124]. Polymicrobial infections caused by multi-drug resistant, aerobic Gram-negatives predominated in a tertiary care center in India and Pakistan [1025]. In contrast to Western countries, S. aureus is less prevalent and P. aeruginosa is more common in developing countries with warm climates, especially Asia and Africa [92627]. The reasons for this are not clear but may be related to environmental factors, footwear, personal hygiene, antimicrobial pre-treatment, or other factors [11]. In Korea, Gram-positive aerobes such as Staphylococcus, Streptococcus, and Enterococcus are more common than Gram-negative aerobes such as Enterobacteriaceae and Pseudomonas (Table 2). Among them, S. aureus is the most common pathogen, with a prevalence ranging from 26.2% to 46.3% (Table 2)[282930313233]. Anaerobes are predominantly seen in DFIs with ulcers that are deeper and more chronic and are associated with ischemia, necrosis, gangrene, or foul odor; however, their clinical significance is not yet clear [34]. Genetic (molecular) analysis can rapidly and reliably detect many more microorganisms (especially anaerobes) than conventional culture methods and is used for characterization, determination of virulence, and the potential antibiotic resistance of pathogens in patients with DFIs [353637]. Their role in improving the clinical care of patients with DFIs will become more significant with the use of metagenomics, transcriptomics, proteomics, and metabolomics [37].
Table 2
Studies on causative microorganisms isolated from diabetic foot infections in Korea (modified from reference [64])
| 1st author (reference) | Choi SR [47] | Seo YB [65] | Lee DH [59] | Park SJ [48] | Son ST [66] | ||
|---|---|---|---|---|---|---|---|
| Year | 2006 | 2007 | 2009 | 2009 | 2017 | ||
| Total number of enrolled patients | 207 | 74 | 68 | 140 | 745 | ||
| Number of patients with isolated strains/with multiple strains (%) | 121 (58.4)/40 (19.3) | 51 (68.9)/6 (8.1) | 67 (98)/31 (46.3) | 113 (80.7)/27 (19.3) | 613 (82.2)/-a | ||
| Number of microorganisms (%)b | |||||||
| Gram-positive aerobes | 90 (74.4) | 39 (76.4) | 54 (80.6)c | 72 (63.7) | 478 (57.5) | ||
| MSSA | 30 (24.8) | 8 (15.6) | 5 (7.5) | 35 (31) | 104 (12.5) | ||
| MRSA | 26 (21.5) | 15 (29.4) | 19 (28.4) | 10 (8.8) | 114 (13.7) | ||
| Other Staphylococcus spp. | 14 (11.6) | 0 | 11 (16.4) | 11 (9.7) | 29 (3.5) | ||
| Streptococcus spp. | 10 (8.3) | 12 (23.5) | 8 (11.9) | 0 | 54 (6.5) | ||
| Enterococcus spp. | 10 (8.3) | 3 (5.9) | 10 (14.9) | 6 (5.3) | 118 (14.2) | ||
| Other Gram-positives | 0 | 1 (2.0) | 1 (1.5)c | 10 (8.8) | 59 (7.1) | ||
| Gram-negative aerobes | 77 (63.6) | 17 (33.3) | 21 (31.3)c | 41 (36.3) | 333 (40.0) | ||
| Enterobacteriaceae | 47 (38.8) | 7 (13.7) | 10 (14.9)c | 20 (17.6) | 174 (21.0) | ||
| Pseudomonas spp. | 18 (14.9) | 4 (7.8) | 11 (16.4) | 10 (8.8) | 78 (9.4) | ||
| Acinetobacter spp. | 0 | 2 (3.9) | 0 | 0 | 13 (1.6) | ||
| Other Gram-negatives | 12 (9.9) | 3 (5.9) | 0 | 11 (9.7) | 68 (8.2) | ||
| Fungus | 3 (2.5) | 1 (2.0) | 1 (1.5)c | 0 | 9 (1.1) | ||
| Anaerobes | -a | 0 | -a | 0 | 12 (1.4) | ||
3. Antimicrobial resistance
Methicillin-resistant S. aureus (MRSA) is more often isolated from patients who have recently received antibiotic therapy, have been previously hospitalized, have nasal carriage of MRSA or osteomyelitis, or have a long wound duration (≥4 weeks) [3839]. The majority of studies in the 1990s and 2000s reported a 15-30% prevalence of MRSA among patients with DFIs [38]. The burden of MRSA has dramatically increased in many countries since the late 1990s, but it has recently been declining globally, especially in high-income countries, concomitant with improved hospital infection control measures [40414243]. DFIs caused by MRSA have been thought to have worse outcomes; however, a recent review found that they did not differ from those of other pathogens [44]. Although the burden of MRSA in DFIs has been declining, antibiotic coverage targeted against MRSA remains unnecessarily high; therefore, antimicrobial stewardship programs for empiric MRSA coverage in DFIs are needed [45].
According to the largest recent study of DFIs in Korea, the prevalence of DFIs caused by MRSA was 13.7%, which was lower than those reported by three studies from the first decade of the 20th century (Table 2). Among the total pathogens of DFIs, the proportion of MRSA is decreasing, as in other countries; however, the methicillin resistance rate in S. aureus is still above 50% (Table 2). The reason for this is that most of the studies were conducted in tertiary referral hospitals and the patients included in these studies were more likely to have chronic DFIs with risk factors for MRSA. Recent nationwide retrospective studies in Korea including mainly community-acquired soft tissue infections such as cellulitis and community-acquired necrotizing fasciitis found that the proportion of MRSA was very low, ranging from 1.8% to 6.8% [46474849].
Multi-drug resistant (MDR) Gram-negative microorganisms, including extended-spectrum beta-lactamase (ESBL) or carbapenemase-producing Enterobacteriaceae and MDR non-fermenters, are becoming a serious concern in tertiary referral hospitals in developing countries [1025505152]. A recent study of Korean patients with DFIs revealed that the risk factors for Pseudomonas infection included smoking history and previous antibiotic use [39]. Two studies conducted in Korea reported antimicrobial susceptibility rates to Gram-negatives for imipenem, cefoperazone, piperacillin/tazobactam, aminoglycosides (gentamicin or amikacin), cefepime, and ciprofloxacin of 85.3-100%, 97.1%, 80.5-94.1% and 75.6%-94.1%, 91.4%, and 63.4%, respectively [2932].
Antimicrobial treatment
1. Severity assessment
Assessing the severity of DFIs is crucial in determining the need for hospitalization, the choice of empirical antibiotics (broad-spectrum intravenous antibiotics or narrow-spectrum oral antibiotics), and the potential necessity and timing of foot surgery and the possibility of amputation [5354]. The IDSA and IWGDF have established criteria to assess the severity of DFIs (Table 3) [611]. While mild infections are relatively easily treated, moderate infections may be limb-threatening and severe infections may be life-threatening [11]. Mild and severe infections are clearly defined, but moderate infections are very difficult to define clearly due to their wide range of wounds, which may be complicated, limb-threatening, and rapidly deteriorating [55].
Table 3
Infectious Diseases Society of America (IDSA) and International Working Group on the Diabetic Foot (IWGDF) classifications of diabetic foot infection (adopted from references [6711]).

aIschemia may increase the severity of any infection; the presence of critical ischemia often makes the infection severe. Systemic infection may manifest with other clinical findings such as hypotension, confusion, vomiting, or evidence of metabolic disturbances such as acidosis, severe hyperglycemia, and new-onset azotemia.
PaCO2, partial pressure of arterial carbon dioxide.
Diabetes can impair local and systemic responses to infection due to its effects on the vascular, nervous, and immune systems, potentially masking the typical clinical features and interfering with diagnosis [56]. Pain can be masked by peripheral neuropathy. Erythema or induration also may be reduced by peripheral artery disease, autonomic neuropathy, and diminished skin blood flow [7]. Because the improper functioning of leukocytes may make the typical inflammatory signs absent or blunted in DFIs, alternative signs (e.g., purulent and nonpurulent discharge, fetid odor, necrosis, undermining of wound edges, poor granulation tissue, and lack of wound healing) might be helpful in increasing the suspicion of infection [565758]. A deep space infection may be difficult to diagnose because of the lack of signs on the surface, but should be considered if there is evidence of systemic toxicity, inflammation distant from the skin wound, persistent infection, elevated levels of inflammatory markers despite appropriate therapy, worsening of previously well-controlled glycemia, or pain in a previously insensate foot [11].
2. Antibiotics administration
Clinicians often prescribe antibiotics expecting that they will prevent infection and promote wound healing, even if diabetic foot ulcers are not infected; however, there is no evidence to support this assumption [59]. Overuse of antibiotics increases the incidence of adverse events, antibiotic resistance, and cost. Therefore, it is recommended that antibiotics not be prescribed for clinically uninfected wounds to prevent infection or promote wound healing. When classic signs of infection (erythema, edema, heat, pain, and purulent discharge) are not clear due to ischemia and neuropathy in diabetic foot wounds, secondary signs of infection such as serous exudate, delayed healing, friable granulation tissue, discolored granulation tissue, foul odor, pocketing of the wound base, and wound breakdown can be taken as an evidence of infection [60]. In these unusual cases, it may be appropriate to administer a brief course, culture-directed antibiotic and observe the therapeutic response [6].
Empirical antibiotics are initially selected based on the clinical features, disease severity, and local antimicrobial resistance patterns in the patients with DFIs. Narrow-spectrum oral antibiotics can be administered for mild infections and broad-spectrum parenteral antibiotics administered for to severe infections. Oral or parenteral antibiotics can be administered for moderate infections according to the patient’s circumstances. An empiric regimen should always include antibiotics active against standard strains of Staphylococccus and Streptococcus species and, in some specific situations, include antibiotics active against Gram-negative rods, MRSA, Pseudomonas, MDR pathogens, and anaerobes. It is not clear if any one systemic antibiotics treatment is better than others in resolving infection or in terms of safety, except that tigecycline is significantly less effective and associated with more adverse effects than ertapenem (± vancomycin) [61]. The lists of empirical antibiotics are summarized in Table 4, which refers to the IDSA and IWGDF guidelines and considers the situations in Korea.
Table 4
Antibiotic recommendations for the empirical treatment of diabetic foot infections.
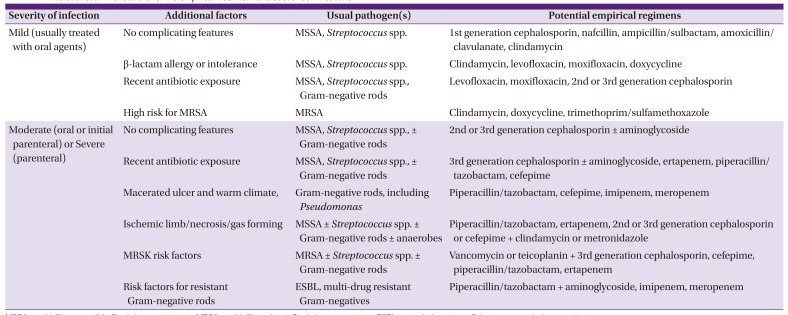
Because the resistance rate against ampicillin/sulbactam in Escherichia coli and Klebsiella pneumoniae bacteremia in the emergency department of a Korean secondary care hospital was 45.8%, ampicillin/sulbactam and amoxicillin/clavulanate were excluded from the empirical antimicrobial agents against Gram-negative rods [62]. In addition, ciprofloxacin was also excluded from the empirical antibiotics because the susceptibility to ciprofloxacin in Gram-negative rods was low, only 63.4% in Korean patients with DFIs, and it is better to reduce the likelihood of resistance and reserve it as a useful definite oral antimicrobial agent [30]. Because the susceptibilities of aminoglycosides in Korean patients with DFIs are acceptable (75.6%-94.1%), aminoglycosides can be prescribed against resistant Gram-negative rods together with other baseline agents such as piperacillin/tazobactam or 3rd generation cephalosporins on the caution of renal toxicity.
A recent Korean clinical guideline for the antibiotic treatment of community-acquired skin and soft tissue infection recommended that the use of antibiotics targeting MRSA in cellulitis may be considered in cases of previous MRSA infection/colonization or failed primary antibiotic treatment [63]. This guideline also recommended that empirical antibiotics targeting MRSA be considered in necrotizing fasciitis because of its serious progression and high mortality rate, although the prevalence of MRSA infection is low in Korea [63]. The prevalence of MRSA infection in Korean patients with DFIs is higher than that in community-onset cellulitis or necrotizing fasciitis because of the chronicity of diabetic foot problems. It is better to use oral empirical antibiotics targeting MRSA for mild and some moderate DFIs with risk factors for MRSA and parenteral empirical antibiotics targeting MRSA in severe infections with risk factors for MRSA. There is no reason to be reluctant to administer anti-MRSA empirical antibiotics for necrotizing fasciitis in DFIs as well. The IDSA also recommends empirical antibiotic regimens which covers MRSA in situations such as history of previous MRSA infection or colonization within the past year, high local prevalence of MRSA (perhaps 50% for a mild and 30% for a moderate infection), and a sufficiently severe infection that the failure of empirical antibiotics is not acceptable [6]. However, in Korea, we should be aware of the HIRA standard, in which linezolid and tigecycline are not reimbursed for prescription for empirical use and vancomycin or teicoplanin are approved only for severe infections in immunocompromised patients [64].
Empirical antibiotics can be continued or modified to definite antibiotics according to the culture results of specimens that appropriately obtained and handled, based on the clinical responses to the empirical regimen. If the patient is clinically improving and does not have a severe infection, the empiric antibiotics can be continued even if the antibiotic susceptibility results show that some or all of the isolated organisms are resistant to the agents prescribed [11]. Even if cultures yield multiple organisms, it may be sufficient to treat only the likeliest pathogens, such as S. aureus, Streptococcus species, and Enterobacteriaceae [3465]. Skin commensals such as coagulase-negative Staphylococci, Corynebacteria, or Bacillus spp. and low-virulence organisms such as Enterococci, can usually be ignored unless cultured from deep, aseptically collected tissue or infections involving osteosynthetic material or hardware [66]. However, if the infection is not responding, the empirical antibiotics should be modified to agents which have a broader spectrum and activity against all isolated organisms. If the infection worsens despite appropriate antimicrobial therapy, it is important to consider whether surgical intervention is necessary; whether fastidious infecting organisms were not recovered in culture, if patient compliance is suboptimal; or if serum levels, absorption, or metabolism of the prescribed antibiotics are inadequate [11].
One to two weeks of antimicrobial treatment are usually effective for mild infections; the treatment can be extended up to three weeks for moderate to severe infections if the infection is limited to soft tissue [611]. Antibiotics can be discontinued when the clinical signs and symptoms of infections have resolved, rather than continuing them until the wound is healed [55]. Routinely prescribing antibiotics for a fixed duration may result in an insufficient or, more often, unnecessarily prolonged course of therapy [6]. The duration of the antibiotics administration should be determined according to the clinical situation, such as the presence of osteomyelitis, perfusion impairment, or implanted foreign body or surgical procedures such as debridement, resection, or amputation. Efforts to shorten the duration of antibiotics for DFIs should be made in order to reduce the likelihood of antimicrobial resistance, adverse events, and cost.
Conclusion
The implementation of an antimicrobial stewardship program is suggested to reduce the inappropriate and unnecessary use of antibiotics in DFIs. However, the HIRA insurance standard needs to be rationally revised so that broad-spectrum antimicrobial agents can be used empirically for severe infections such as necrotizing fasciitis in DFIs. In Korea, nationwide studies are necessary and guidelines for DFIs should be developed.
 XML Download
XML Download