

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
As a result of the development of combination antiretroviral therapy (ART), human immunodeficiency virus (HIV) infection is now a chronic disease rather than an acute infectious disease. The importance of early diagnosis and care of age-related non-communicable diseases (NCDs) in HIV-infected patients has recently been emphasized [1234]. Although ART has significantly decreased the mortality rate from HIV infection, the prevalence of major NCDs, including metabolic, cardiovascular, kidney, and bone-related complications, has increased owing to increased survival of chronically HIV-infected patients [5678] According to a modeling study, the prevalence of NCDs in this population is expected to increase from 29% in 2010 to 84% in 2030 [4]. Renal insufficiency is one of the important NCDs and is independently associated with morbidity and mortality in HIV patients [91011]. After the first report of HIV-associated nephropathy (HIVAN) in 1984 [12], there have been several research studies on the association between HIV infection and development of renal dysfunction HIV infection is not only an independent risk factor for acute kidney injury (AKI) [13], but also a potential risk factor of chronic renal insufficiency due to harmful complex mechanisms including direct viral cell injury, chronic inflammation, aging, co-infections, and use of nephrotoxic drugs [81415]. Traditional risk factors for renal insufficiency are age, hypertension (HTN), and diabetes mellitus (DM) [816]. In HIV patients, additional HIV-related factors including low CD4 counts, high viral load, hepatitis C virus (HCV) co-infection, and ART (mainly tenofovir, indinavir, and lopinavir/ritonavir) may also be potential risk factors [781417]. The prevalence of renal insufficiency in HIV patients varies among studies owing to differences in the studied populations, historic periods, and settings as well as the estimated glomerular filtration rate (eGFR) equations used to evaluate renal function [81819]. Furthermore, there are very few published studies about renal insufficiency in HIV-infected patients in Asia, especially in South Korea. Therefore, we investigated the prevalence and risk factors of renal insufficiency in HIV-infected patients in South Korea.
Materials and Methods
1. Study design and populations
The Korea HIV/AIDS Cohort Study is a multicenter prospective cohort study with ongoing enrollment of HIV-infected patients from 19 hospitals in South Korea. At the time of registration, the enrolled participants are interviewed by a trained clinical researcher and baseline information on clinical and epidemiological data is collected using a standardized protocol [20]. Information on medical history, physical findings, and laboratory findings, including immunological and virological status, is collected every 6 months. This was a cross-sectional point prevalence study. We performed a case–control study with 1,218 HIV-infected patients older than 18 years who were enrolled from December 2006 to July 2013. To evaluate the prevalence and risk factors of renal insufficiency, we investigated baseline data at the time of registration in the Korea HIV/AIDS Cohort Study.
2. Collected data
Infection with HIV was screened using enzyme immunoassays and confirmed by western blot analysis. Renal insufficiency was defined as an eGFR <60 mL/min/1.73 m2 at the time of registration. Using serum creatinine levels, eGFR was calculated using the simplified modification of diet in renal disease (MDRD) equation [21]. The eGFR results were stratified according to the National Kidney Foundation Kidney Disease Outcome Quality Initiative (NKF-K/DOQI) staging system [22]. All of the patients classified in stages 3 through 5 (i.e., with eGFR <60 mL/min/1.73 m2) were considered to have renal insufficiency. Creatinine was measured using isotope dilution mass spectrometry traceable calibration. End-stage renal disease (ESRD) was defined as eGFR <15 mL/min/1.73 m2 and/or treatment with renal replacement therapy. The collected data included sex, age, body mass index (BMI), time since diagnosis with HIV infection, opportunistic infection, co-infection with hepatitis B virus (HBV, defined as a positive hepatitis B surface antigen test), co-infection with HCV (defined as positive anti-HCV serology), DM (defined as a fasting plasma glucose ≥126 mg/dL or the use of antidiabetic drugs), HTN (defined as systolic blood pressure (BP) ≥140 mmHg and/or diastolic BP ≥90 mmHg and/or use of antihypertensive therapy), cardiovascular disease (CVD, defined as a history of any of the following: coronary heart disease, cerebrovascular disease, peripheral arterial disease), coronary heart disease (defined as a history of angioplasty, coronary artery bypass grafts, myocardial infarction, or angina), cerebrovascular disease (history of transient ischemic attack, stroke, or carotid endarterectomy), peripheral vascular disease (defined as a history of claudication, ischemic limb loss and/or ulceration, or a peripheral revascularization procedure), route of transmission, CD4 cell count, HIV viral load, ART history, and serum chemistry at study enrollment. We excluded patients who were not Korean or had a lack of sufficient data. In cases when eGFR was not known, the absence of a significant factor such as HTN, DM, and BMI or an unknown ART history were excluded from the analysis.
3. Statistical analysis
Correlations of various factors were compared according to renal function status. None of the continuous variables except for age followed a normal distribution, and therefore, median and interquartile range (IQR, Q1 – Q3) are presented after a median two-sample test was used to evaluate significance. When the categorical variables expected value are <5, the significant difference was confirmed using Fisher’s exact test. Student’s t-test was used for the other continuous variables and the Chi-square test was used for categorical variables. Regression analysis was used for the correlation analysis and the final model was constructed by using the stepwise selection variables option in the logistic regression procedure after simple logistic regression was performed for the variables with significant differences between the groups. The significance level for entry into the model was defined as 0.2. The clinically defined confounding variable, HTN, was excluded by the selection method. As there was an interaction between HTN and ART regimens, we presented adjusted odds ratios (aORs) using a stratified method. The explanatory power of the regression equation was presented as the adjusted max-rescaled r2 value. The cumulative number of subjects with renal insufficiency was shown. The statistical significance level was 5% (P value = 0.05). All statistical analyses were performed using the SAS statistical program version 9.3 (SAS Institute, Cary, NC, USA).
Results
1. Clinical characteristics of patients and risk factors associated with renal insufficiency
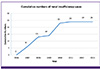
A total of 1,218 HIV patients were enrolled from December 2006 to July 2013. Owing to missing data and being non-Korean, 764 patients were excluded from analyses. We analyzed data from 454 patients (Fig. 1). Of 454 patients, only 24 showed renal insufficiency (eGFR <60 mL/min/1.73 m2), a prevalence of 5.3%. After excluding only the 128 patients with no eGFR data, 44 of 1,090 patients showed renal insufficiency (4.04%). According to the NKF-K/DOQI staging system, 271 patients (59.6%) had stage 1 (eGFR ≥90 mL/min/1.73 m2) and 160 (35.2%) had stage 2 (eGFR 60~89 mL/min/1.73 m2) kidney disease (Table 1). There was only one patient with ESRD (0.2%). The cumulative number of patients with renal insufficiency in Korean HIV-infected patients in our cohort for each year was demonstrated (Fig. 2).
Figure 1
Exclusion criteria of study population
HIV, human immunodeficiency virus; RNA, ribonucleic acid; ART, antiretroviral treatment.

Table 1
Distribution of the HIV/AIDS cohort of HIV-infected patients based on eGFR categories
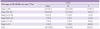
Figure 2
Cumulative numbers of renal insufficiency cases in Korean HIV-infected patients for each year of the study
We analyzed the distribution HIV-infected patients by eGFR and age (Table 2). We found that 23.8% of patients under 35 years of age did not have renal insufficiency. The mean age of patients with renal insufficiency was 52.8 ± 9.4 years, which was significantly older than patients with normal renal function (43.4 ± 11.8 years, P = 0.0002). When the data were analyzed according to age categories, the results remained significant with respect to more renal insufficiency in older patients. Sex and BMI were not significantly different in both groups. When BMI was categorized as IQR or classified according to the World Health Organization criteria, the renal insufficiency group tended to be more overweight, but this was not significant. Male sex was predominant in both groups (94.0% vs. 91.7%). Regarding the route of transmission, the proportion of homosexual transmission was lower and that of unknown route of transmission was significantly higher in the renal insufficiency group than that in the normal renal function group.
Table 2
Distribution of the HIV/AIDS cohort of HIV-infected patients based on age

In the renal insufficiency group, 37.5% and 29.2% of patients had diabetes and HTN, and diabetes was significantly more common than in the normal renal function group (10.2% vs. 37.5%, P = 0.0007). The HBV and HCV co-infection rates were also not different between the two groups. The mean CD4 cell count was 400 (IQR 190–578) cells/mm3 and mean HIV viral load was 25 (IQR 20–75) copies/mL. The mean CD4 cell count and HIV viral load in the renal insufficiency group were not different from those in the normal renal function group.
All of the patients were receiving ART (100%), the majority with a protease inhibitor (PI)-based regimen, for an average duration of 29 (interquartile range [IQR] 5–67) months in the renal insufficiency group and 19 (IQR 4–45) months in the normal renal function group (not a statistically significant difference). No subjects in either group were taking tenofovir, and the proportion of patients taking indinavir was significantly higher in the renal insufficiency group than in the normal renal function group [33.3% (8/24) vs. 10.9% (47/430), P = 0.004], respectively. There was a significant correlation between use of a PI-based regimen and renal insufficiency, but it was not significant except for indinavir in a PI-based regimen. Therefore, it was interpreted that exposure to indinavir had a significant effect on correlation, which was considered in the univariate and multivariable analyses. Other PIs were not significantly correlated with renal insufficiency and are not presented separately (Table 3).
Table 3
Demographic and clinical variables in HIV-infected patients with and without renal insufficiency

aMean ± standard deviation
bFisher's exact test
cMedian (interquartile range)
dMedian two sample test
HIV, human immunodeficiency virus; BMI, body mass index; RNA, ribo nucleic acid; HBV, hepatitis B virus; HCV, hepatitis C virus; ART, antiretroviral treatment; PI, protease inhibitor; eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease.
In univariate analysis, older age (≥65 years) (P = 0.003), unknown transmission (P = 0.007), DM (P = 0.0002), and receiving PI-based ART with indinavir (P = 0.0022) were associated with renal insufficiency in HIV-infected patients. However, sex, other underlying diseases, baseline CD4 cell count, HIV RNA titer, HBV/HCV co-infection, and use of tenofovir were not associated with renal insufficiency (Table 4). In multivariable analysis, older age (≥65 years) [aOR 6.84, 95% confidence interval (CI) 1.71–27.34, P = 0.007], unknown transmission (aOR 6.42, 95% CI 1.83–22.55, P = 0.004), exposure to indinavir (aOR 3.52, 95% CI 1.32–9.35, P = 0.012), and DM (aOR 3.60, 95% CI 1.38–9.36, P = 0.009) were independent risk factors of renal insufficiency in HIV-infected patients (Table 4). In addition, as there was an interaction between HTN and ART regimens (interaction P-value = 0.0487), we performed an additional stratified multivariable analysis (Table 5). In patients with HTN, indinavir exposure (aOR 29.80, 95% CI 2.99–297.23, P = 0.004) and DM (aOR 8.64, 95% CI 1.12–66.50, P = 0.038) were significant risk factors of renal insufficiency. In patients without HTN, older age (≥65 years) (aOR 10.20, 95% CI 2.15 – 48.51, P = 0.004) and unknown route of transmission (aOR 5.92, 95% CI 1.36 – 25.72, P = 0.018) were significant risk factors. The explanatory power of the regression model verified by the adjusted max-rescaled R2 value was higher after performing the stratified analysis (Table 5).
Table 4
Risk factors associated with renal insufficiency (<60 mL/min per 1.73 m2) in HIV-infected patients in logistic analysis

Table 5
Stratified multivariable analysis of independent risk factors associated with renal insufficiency in HIV-infected patients

Discussion
Our cross-sectional study shows the prevalence and associated risk factors of renal insufficiency in HIV-infected patients. Renal disease is increasingly becoming recognized as a major global health problem and is associated with a poor health outcome in HIV-infected patients. There is a growing concern that HIV significantly contributes to the prevalence of renal insufficiency worldwide [823]. Although the incidence of ESRD in HIV-infected individuals has decreased over time, HIV patients are still more likely than HIV-negative individuals to develop ESRD [24]. The incidence of renal insufficiency is increasing in HIV-infected patients living in Asian countries [25] as well as those in Western countries. The overall prevalence of chronic renal insufficiency among the general population in the United States is 13.1% and the reported prevalence in South Korea is 13.7% [2627]. As mentioned above, the prevalence of HIV-associated renal insufficiency varies geographically and also depends on the definition of renal insufficiency, ranging from 4.7% to 38% globally [19]. In North America and Europe, the reported prevalence of renal insufficiency (defined as eGFR <60 mL/min/1.73 m2) among HIV-infected patients ranges from 4.7% to 9.7% [2829]. However, if the renal insufficiency definition includes reduced eGFR and/or proteinuria, the rate increases to 15.5% [30]. Notably, regarding genetic factors, the prevalence of renal insufficiency in HIV-infected African populations seems to be higher, in the range of 3.5–48.5%, and related to polymorphisms in the apolipoprotein L1 (APOL1) gene that is related to a high risk for developing HIVAN [173132]. In a study in China, 16.8% of HIV-infected patients had chronic renal insufficiency (defined as eGFR <60 mL/min/1.73 m2 and/or proteinuria), but this study reported a prevalence of just decreased eGFR (<60 mL/min/1.73 m2) of 5.6% [25]. In addition, studies in Japan have reported renal insufficiency (defined as eGFR <60 mL/min/1.73 m2) prevalence rates from 6.7% to 9.7% [3334]. In a Korean chronic kidney disease (CKD) cohort study, using just decreased eGFR (<60 mL/min/1.73 m2) as a criterion, the prevalence was 5.0% [27]. Likewise, in our study, the prevalence of renal insufficiency in HIV-infected patients was 5.3%, which was similar in the general population in Korea and in other studies of HIV-infected patients [2735].However, there is a limitation that the definition of renal insufficiency was defined only as a reduction in eGFR (<60 mL/min/1.73 m2). If proteinuria was added to the definition as in other studies, the prevalence might have increased [30]. However, just a single eGFR value <60 mL/min/1.73 m2 was significantly associated with an increased mortality and cardiovascular risk [736]. Nevertheless, this study is meaningful as the first report to investigate the prevalence of renal insufficiency in Korean HIV-infected patients.
The prevalence of decreased eGFR in Korean HIV-infected patients was relatively low compared with that in an African HIV population, which may be related to the following reasons. Overall, a quarter of HIV-infected patients are co-infected with HCV, and HCV co-infection may cause specific immune complex-mediated kidney disease. In this regard, HCV co-infection is associated with a significant increase in the risk of HIV-related renal disease. [35] However, in this study, this factor did not show significance. In Korea, the prevalence of HCV co-infection is low, possibly because the number of intravenous drug users among HIV-infected patients is low [36]. Therefore, the influence of HCV is considered minimal and it was associated with a low prevalence of renal insufficiency in Korea. In addition, tenofovir is a well-known risk factor of CKD and is capable of inducing renal tubular injury [814]. Our study did not include patients taking tenofovir because tenofovir has been used in South Korea only since December 2012. Therefore, the non-use of tenofovir may have affected our results. In addition, HIVAN is more commonly diagnosed in patients of African descent and plays an important role in ESRD [30]. In South Korea, there have been only three case reports of HIV-associated glomerulonephritis to date [37], and therefore, the prevalence rate is not expected to be high. This may be associated with genetic factors of HIVAN development, but additional studies including renal biopsy are needed.
Our study identified older age and diabetes as risk factors of renal insufficiency in Korean HIV-infected patients. These factors are well-known risk factors associated with renal insufficiency in uninfected individuals and are also associated with renal insufficiency among HIV-infected patients [15253037]. In our findings, HTN and CVD were not associated with renal insufficiency. This may be due to the fact that the majority of patients with these conditions also had diabetes or due to a lack of power. In addition, a traditional CKD risk factor, BMI, was not significant in this study [38].
Exposure to indinavir was a significant risk factor with renal insufficiency in our study. Traditionally, PIs are regarded as a major risk factor for renal dysfunction in HIV-infected patients. PIs including indinavir have been associated with crystalluria, nephrolithiasis, acute or chronic interstitial nephritis, and renal insufficiency in previous studies [131439]. Especially, in patients with HTN, PI use was a significant risk factor of renal insufficiency in this study. Therefore, in hypertensive HIV-infected patients, indinavir should be used with caution. There was no statistically significant difference in ART duration, but it was estimated that the longer ART duration of the renal insufficiency group might have affected renal function. However, research for a longer period of time may show meaningful results.
In this study, we found that the prevalence of renal insufficiency was high in patients who did not disclose their sexual behavior or did not know the route of transmission at the initial diagnosis of HIV infection. This is probably an indicator of the patient’s adherence and self-management status. Therefore, patients with non-adherence may need closer monitoring for decreased renal function. However, because the number of patients in the renal insufficiency group was small in this study, it is possible that the effect of this factor is overestimated and will require additional research.
A high HIV RNA load and low CD4 cell count are also specific risks for renal insufficiency in HIV-infected patients [16253340], but these factors did not show significance in this study. Both groups in this study showed a low HIV RNA load and high CD4 cell count. Considering that these were baseline values at the time of study enrollment, most of the participating patients in the study had a good infection control status. Because all of the patients were receiving ART, these laboratory results did not reflect patient risk.
Our study has several limitations. First, because of the cross-sectional design of this study, we could not adequately assess the development and persistence of the decreased eGFR of <60 mL/min/1.73 m2. In addition, it was not possible to confirm whether the renal insufficiency occurred before or after exposure to ART. Second, we lacked data on proteinuria and albuminuria, which are significant indicators of renal dysfunction in HIV patients. In addition, the prevalence of renal insufficiency in this study could be underestimated because proteinuria was not included in the definition of renal insufficiency. Third, we used only the MDRD equation for eGFR; if results using the Cockcroft-Gault formula or CKD-EPI (Epidemiology Collaboration) equation were compared, the data would be more meaningful. Fourth, since our patients were predominantly Korean men who received care in a tertiary hospital, our results may not be generalized to female patients, patients without access to healthcare, or other racial groups not represented in this cohort. Fifth, a large proportion of the patients who initially enrolled were excluded due to lack of data. Eventually, only 37.3% of the patients were analyzed, and the prevalence of renal insufficiency differed from that in all enrolled patients (4.04% vs. 5.3%). Therefore, the results of this study may not be generalizable to all Korean HIV patients.
In Korea, the prevalence rate of HIV-infected individuals is still low, but the cumulative number with the aging of patients is increasing. In this large cohort study, the prevalence of renal insufficiency in HIV-infected patients in Korea was relatively similar to that in China, North America, and Europe, although the cumulative prevalence rate significantly increased, indicating that continuous monitoring and further research are required.
In conclusion, older age, DM, taking indinavir, and unknown transmission route (considered to reflect adherence) were independent risk factors of renal insufficiency. In the presence of HTN in HIV-infected patients, the risk of renal insufficiency was especially higher in patients with DM and in those taking indinavir. In addition, the risk of renal insufficiency is not clear for HTN itself, but it is interpreted that the risk increases when other factors are also present together. Therefore, we need careful examination and follow-up with respect to renal function when the above factors are present in HIV-infected patients. Furthermore, we also need closer monitoring of hypertensive HIV-infected patients who have DM or are taking indinavir. In addition, further studies of the incidence and risk factors of renal insufficiency during HIV infection using follow-up cohort data are needed.
 XML Download
XML Download