

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
The incidence of thyroid cancer is rapidly increasing. The aim of this study is to examine time trends in the characteristics of thyroid cancer and to determine the cause of the increase of thyroid cancer.
Methods
We evaluated 4,646 patients that underwent surgery at the Asan Medical Center for thyroid cancer between 1995 and 2006. Patients were evaluated concerning the histology, size of the primary tumor, sex, and age at the time of surgery.
Results
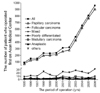
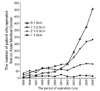
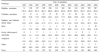
Surgically treated case of thyroid cancer increased from 91 in 1995 to 960 in 2006-a 10.5-fold increase during the 12-year period. Based on the histological categories, the proportion of papillary thyroid carcinomas (PTCs) increased from 79.1% to 94.5% during the 12-year period. According to the primary tumor size in the PTCs, the proportion of PTCs measuring 1 cm or smaller increased from 14% to 56% during the 12-year period. Whereas the proportion of PTCs measuring from 1 cm to 2 cm were similar (between 31% and 41% during the 12-year period), the proportion of PTC measuring from 2 cm to 4 cm decreased from 51% to 11% during the 12-year period. Thyroid cancer affected women more often than men by a ratio of 3.7. PTC was most common in patients in their forties, especially among women.
Conclusion
The increasing number of surgically treated cases of thyroid cancer is predominantly due to an increase of papillary thyroid cancer measuring 1 cm or less. These trends suggest that the increase in surgically treated cases of thyroid cancer reflects increased detection of occult thyroid cancer due to advances in medical surveillance of impalpable nodules rather than a true increase in the number of thyroid cancers.
Figures and Tables



References
1. Sherman SI. Thyroid carcinoma. Lancet. 2003. 361:501–511.
2. Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006. 295:2164–2167.
3. Leenhardt L, Grosclaude P, Cherie-Challine L. Increased incidence of thyroid carcinoma in france: a true epidemic or thyroid nodule management effects? Report from the French Thyroid Cancer Committee. Thyroid. 2004. 14:1056–1060.
4. Liu S, Semenciw R, Ugnat AM, Mao Y. Increasing thyroid cancer incidence in Canada, 1970-1996: time trends and age-period-cohort effects. Br J Cancer. 2001. 85:1335–1339.
5. Reynolds RM, Weir J, Stockton DL, Brewster DH, Sandeep TC, Strachan MW. Changing trends in incidence and mortality of thyroid cancer in Scotland. Clin Endocrinol (Oxf). 2005. 62:156–162.
6. Smailyte G, Miseikyte-Kaubriene E, Kurtinaitis J. Increasing thyroid cancer incidence in Lithuania in 1978-2003. BMC Cancer. 2006. 6:284.
7. Colonna M, Guizard AV, Schvartz C, Velten M, Raverdy N, Molinie F, Delafosse P, Franc B, Grosclaude P. A time trend analysis of papillary and follicular cancers as a function of tumour size: a study of data from six cancer registries in France (1983-2000). Eur J Cancer. 2007. 43:891–900.
8. Trimboli P, Ulisse S, Graziano FM, Marzullo A, Ruggieri M, Calvanese A, Piccirilli F, Cavaliere R, Fumarola A, D'Armiento M. Trend in thyroid carcinoma size, age at diagnosis, and histology in a retrospective study of 500 cases diagnosed over 20 years. Thyroid. 2006. 16:1151–1155.
9. Nikiforov YE. Radiation-induced thyroid cancer: what we have learned from Chernobyl. Endocr Pathol. 2006. 17:307–317.
10. Takahashi K, Eguchi H, Arihiro K, Ito R, Koyama K, Soda M, Cologne J, Hayashi Y, Nakata Y, Nakachi K, Hamatani K. The presence of BRAF point mutation in adult papillary thyroid carcinomas from atomic bomb survivors correlates with radiation dose. Mol Carcinog. 2007. 46:242–248.
11. Lee JH, Lee ES, Kim YS. Clinicopathologic significance of BRAFV600E mutation in papillary carcinomas of the thyroid : a meta-analysis. Cancer. 2007. 110:38–46.
12. Chung JH, Hahm JR, Min YK, Lee MS, Lee MK, Kim KW, Nam SJ, Yang JH, Ree HJ. Detection of RET/PTC oncogene rearrangements in Korean papillary thyroid carcinomas. Thyroid. 1999. 9:1237–1243.
13. Park KY, Koh JM, Kim YI, Park HJ, Gong G, Hong SJ, Ahn IM. Prevalences of Gs alpha, ras, p53 mutations and ret/PTC rearrangement in differentiated thyroid tumours in a Korean population. Clin Endocrinol (Oxf). 1998. 49:317–323.
14. Verkooijen HM, Fioretta G, Pache JC, Franceschi S, Raymond L, Schubert H, Bouchardy C. Diagnostic changes as a reason for the increase in papillary thyroid cancer incidence in Geneva, Switzerland. Cancer Causes Control. 2003. 14:13–17.
15. Leenhardt L, Bernier MO, Boin-Pineau MH, Conte Devolx B, Marechaud R, Niccoli-Sire P, Nocaudie M, Orgiazzi J, Schlumberger M, Wemeau JL, Cherie-Challine L, De Vathaire F. Advances in diagnostic practices affect thyroid cancer incidence in France. Eur J Endocrinol. 2004. 150:133–139.
16. Nam-Goong IS, Kim HY, Gong G, Lee HK, Hong SJ, Kim WB, Shong YK. Ultrasonography-guided fine -needle aspiration of thyroid incidentaloma: correlation with pathological findings. Clin Endocrinol (Oxf). 2004. 60:21–28.
17. DeGroot LJ, Kaplan EL, McCormick M, Straus FH. Natural history, treatment, and course of papillary thyroid carcinoma. J Clin Endocrinol Metab. 1990. 71:414–424.
18. Harach HR, Franssila KO, Wasenius VM. Occult papillary carcinoma of the thyroid. A "normal" finding in Finland. A systematic autopsy study. Cancer. 1985. 56:531–538.
19. Noguchi S, Yamashita H, Murakami N, Nakayama I, Toda M, Kawamoto H. Small carcinomas of the thyroid. A long-term follow-up of 867 patients. Arch Surg. 1996. 131:187–191.
20. Solares CA, Penalonzo MA, Xu M, Orellana E. Occult papillary thyroid carcinoma in postmortem species: prevalence at autopsy. Am J Otolaryngol. 2005. 26:87–90.
21. Kovacs GL, Gonda G, Vadasz G, Ludmany E, Uhrin K, Gorombey Z, Kovacs L, Hubina E, Bodo M, Goth MI, Szabolcs I. Epidemiology of thyroid microcarcinoma found in autopsy series conducted in areas of different iodine intake. Thyroid. 2005. 15:152–157.
22. Wiest PW, Hartshorne MF, Inskip PD, Crooks LA, Vela BS, Telepak RJ, Williamson MR, Blumhardt R, Bauman JM, Tekkel M. Thyroid palpation versus high-resolution thyroid ultrasonography in the detection of nodules. J Ultrasound Med. 1998. 17:487–496.
23. Colonna M, Grosclaude P, Remontet L, Schvartz C, Mace-Lesech J, Velten M, Guizard A, Tretarre B, Buemi AV, Arveux P, Esteve J. Incidence of thyroid cancer in adults recorded by French cancer registries (1978-1997). Eur J Cancer. 2002. 38:1762–1768.
24. Memon A, Darif M, Al-Saleh K, Suresh A. Epidemiology of reproductive and hormonal factors in thyroid cancer: evidence from a case-control study in the Middle East. Int J Cancer. 2002. 97:82–89.
25. Suk JH, Kim TY, Kim MK, Kim WB, Kim HK, Jeon SH, Shong YK. Prevalence of ultrasonographically-detected thyroid nodules in adults without previous history of thyroid disease. J Kor Endocrinol Soc. 2006. 21:389–393.
 XML Download
XML Download