

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
As imaging technology has advanced, the incidence of differentiated thyroid carcinoma (DTC) diagnosis has increased. Most DTCs are microcarcinomas, defined as cancers 1 cm or less in size [12]. The traditional treatment for DTC is total thyroidectomy (TT) followed by radioactive iodine (RAI) ablation and thyrotropin (TSH) suppression [3]. The goals of RAI ablation after TT are to remove remnant thyroid tissues, including microscopic thyroid cancer; to allow for the evaluation of the evidence for metastatic disease using whole-body scanning; to enable risk stratification and TSH suppression therapy; and to allow for the thyroglobulin level to be used as a predictor of recurrence [14]. However, RAI ablation may cause fatigue, edema, sialadenitis, xerostomia, second primary malignancies, and other side effects [4]. According to the American Thyroid Association risk stratification guidelines, low-risk DTCs and papillary thyroid microcarcinomas (PTMCs) generally have excellent prognoses [56], and the role of RAI ablation in the treatment of PTMCs and low-risk DTCs is controversial [178].
Assessing the quality of life (QoL) in patients with thyroid cancer might be helpful in determining appropriate treatment strategies, especially RAI therapy [91011]. Several studies have evaluated QoL in patients with DTC [9101213]. The prognoses of patients with DTC were excellent, but their QoL was poor compared with that of the general population [101214]. RAI therapy may be the reason for this poor QoL in DTC survivors. To the best of our knowledge, no studies have compared QoL between patients who underwent TT alone and those who underwent TT with RAI. Therefore, this study aimed to compare QoL parameters between patients with PTMC who underwent TT alone and those who underwent TT with RAI ablation.
METHODS
Patients
Patients with PTMC who underwent TT with/without RAI remnant ablation between June 2016 and October 2017 were prospectively enrolled in this cross-sectional study. During their regular visits, study was fully explained and written consent was obtained. Patients then completed questionnaires, described below. Patients who were previously diagnosed with psychiatric disorders, rheumatologic disorders, and other cancers were excluded. Furthermore, patients with uncontrolled chronic, those requiring three or more medications for hypertension control, and those requiring insulin injection for diabetes control were excluded. We collected demographic characteristics such as age, sex, marital status, education level, employment status, and socioeconomic status that can affect QoL. Medical records and clinical laboratory data such as serum TSH level at the time of questionnaire completion were reviewed and collected. The study protocol was approved by the Institutional Review Board of Asan Medical Center (study number: 2016-0606) and was registered with the Clinical Research Information Service at the Korea Centers for Disease Control and Prevention (KCT0001986) [9].
The RAI dose
RAI remnant ablation was conducted according to Asan Medical Center protocols. PTMC without extrathyroidal extension (ETE) and cervical lymph node (LN) metastasis (pathologically N0) could be observed without RAI or treated with 30 mCi of RAI. PTMC with microscopic ETE and N0 was treated with 30 mCi of RAI. PTMC with central cervical LN metastasis (pathologically N1a) was treated with 80 mCi of RAI.
Questionnaires
To assess QoL, all patients completed three questionnaires: the 12-item short-form health survey (SF-12), thyroid cancer-specific quality of life (THYCA-QoL) questionnaire, and fear of progression (FoP) questionnaire. The SF-12 (v2.0) is a well-validated short-form of SF-36 that consists of 12 questions that provide an eight-dimensional profile of health status, including physical functioning, role limitations due to physical health, role limitations due to emotional problems, general health, vitality, bodily pain, social functioning, and mental health. Answers were combined and weighted to produce Mental and Physical Component Summary scores using the Quality Metric Health Outcomes Scoring Software version 5.0 (QualityMetric, Lincoln, RI, USA) (range, 0 to 100). Lower scores indicated a worse health status [15]. The THYCA-QoL is the first THYCA-QoL questionnaire and contains 24 items that assess symptoms from thyroid cancer or its treatment. Each item was scored on a four-point response scale ranging from 1, “not at all” to 4, “very much.” Each score was converted into scores on seven multi-symptom scales and six single-symptom scales. A lower score indicated lesser complaints caused by that symptom [1617]. FoP evaluates anxiety and fear of disease progression using a 43-item questionnaire. Each item belongs to five subcategories: affective reactions (13 items), partnership/family (seven items), work (seven items), loss of autonomy (seven items), and coping with anxiety (nine items). In all subcategories except coping with anxiety, a higher score indicated more anxiety about disease progression. Conversely, in the coping with anxiety subcategory, a higher score indicated better coping [18].
Statistics
R studio version 3.1.3 (R Foundation for Statistical Computing, Vienna, Austria) was used for data analysis. Continuous variables are presented as means and standard deviations or as medians and interquartile ranges (IQR). Categorical variables are presented as numbers with percentages. We used the t test and Wilcoxon's test to compare continuous variables and the chi-square test to compare categorical variables. Because serum TSH values only show normal distribution after log transformation, serum TSH values were log-transformed, and the geometric mean values were analyzed. All P values were two-sided, and a P value less than 0.05 was considered statistically significant [9].
RESULTS
Baseline characteristics
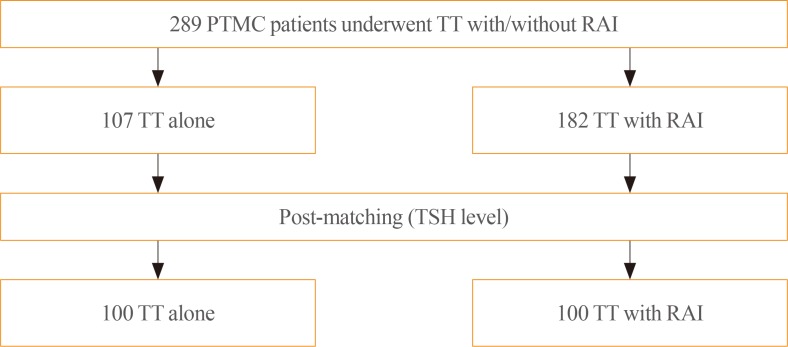
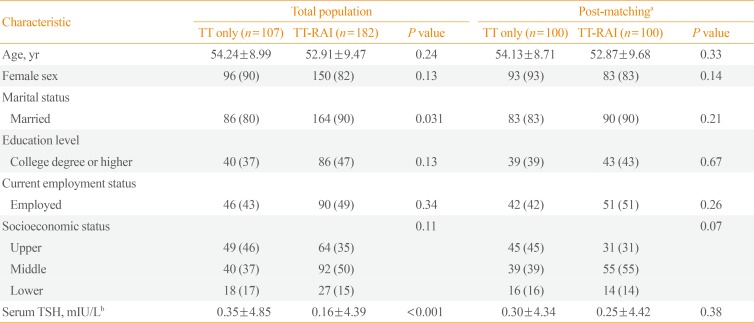
Baseline characteristics of 289 PTMC patients who underwent TT with/without RAI are shown in Table 1. Most patients (99%, n=287) underwent TT with central node dissection. The TT alone and TT with RAI groups included 107 and 182 patients, respectively. The median age of the patients was mid-50s, and most patients were female. No patients had structural disease at the time of questionnaire completion. The median time intervals between TT and questionnaire completion in the TT alone and TT with RAI groups were 3.5 years (IQR, 2.4 to 4.8) and 3.8 years (IQR, 2.9 to 4.5), respectively (P=0.66).
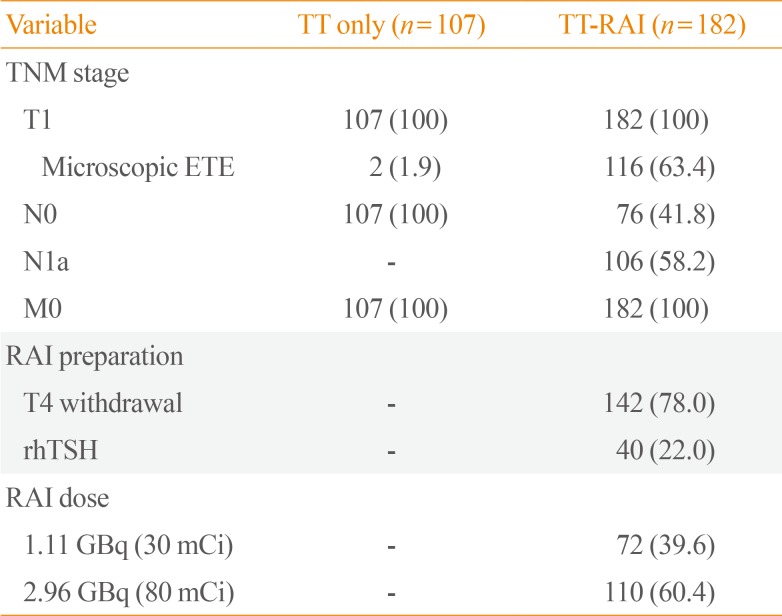
Table 2 shows the pathologic findings and the RAI dose that patients received. None of the patients in the TT alone group had cervical LN metastasis. In contrast, 106 patients (58%) in the TT and RAI group had cervical LN metastasis (pathologically N1a). In the TT and RAI group, 72 patients (40%) received 30 mCi of RAI and 110 (60%) received 80 mCi of RAI owing to the presence of microscopic ETE or cervical LN metastasis. The median dose of RAI was 80 mCi. In terms of preparation for RAI, 40 patients (22%) received recombinant human thyrotropin (rhTSH) rather than undergoing thyroid hormone withdrawal. The median interval between ablation and questionnaire completion was 3.7 years (IQR, 2.8 to 4.4). No patients underwent repeated RAI treatment.
Compared with patients in the TT alone group, those in the TT with RAI group were more frequently married (P=0.031) and exhibited lower serum TSH levels (P<0.001). After matching for TSH levels, the TT alone and TT with RAI groups each comprised 100 patients (Fig. 1). There were no significant differences in baseline characteristics between the two post-matching groups (Table 1).
No patients have subsequently presented with disease recurrence, and no deaths were reported as of the last follow-up date (November 31, 2019).
QoL analysis
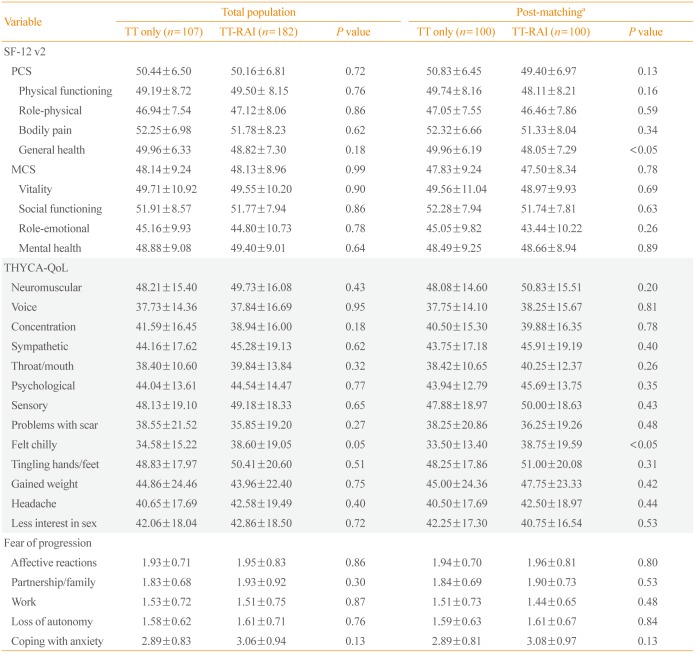
Scores for QoL parameters from the three questionnaires are shown in Table 3. Among the SF-12 parameters, the scores for general health in the TT alone and TT with RAI groups were significantly different between the TSH-matched cohorts (49.96 vs. 48.05, P=0.047), which suggested poorer health status in the TT with RAI group. The “felt chilly” parameter in the THYCA-QoL also showed a significant difference between the matched groups (P=0.023), which suggested more chilly feelings in patients in the TT with RAI group. There were no significant differences in FoP scores between the groups.
In the TT with RAI group, no significant differences in QoL scores were observed between patients prepared for treatment with thyroid hormone withdrawal versus those treated with rhTSH. There was also no significant difference in the QoL parameters according to the RAI dose (data not shown).
DISCUSSION
We evaluated QoL in PTMC patients who underwent TT with/without RAI using three well-validated questionnaires. After matching for TSH levels, patients who underwent TT with RAI presented lower scores for QoL parameters such as “general health” in the SF-12 and “felt chilly” in the THYCA-QoL, although their TSH level was within the reference range. These results suggested that RAI therapy could negatively affect QoL in patients with thyroid cancer. In low-risk DTC or PTMC, RAI remnant ablation has not been shown to benefit clinical outcomes [781920]. Therefore, weighing the risks and benefits of RAI is important. Because DTC has an excellent prognosis and DTC patients live for a long time, efforts to preserve QoL after treatment are needed. Our study suggests that RAI remnant ablation might cause harm in terms of QoL in patients with PTMC.
Previously, little was known about QoL in patients with DTC, especially with respect to RAI. QoL in patients with thyroid cancer is shown to be poorer than that in the general population [2122]. In a previous study that evaluated QoL using the SF-36 and other questionnaires, patients who underwent TT with RAI had lower social functioning and general health perception than healthy controls [23]. For RAI, patients need to stop hormone replacement for several weeks if they are not taking recombinant TSH. This can lead to physical and emotional instability in patients, and there is evidence of reduced glomerular filtration rate and liver enzyme elevation. With the use of recombinant TSH instead of hormone withdrawal, the discomfort and complications of hypothyroidism during the pre-ablation period are reduced [21]. However, RAI can cause multiorgan complications that can occur at various times [4]. Side effects related to the salivary glands, such as sialadenitis and xerostomia, were the most frequent complications of RAI. RAI also affected the eye and gastrointestinal systems in the early-to-intermediate phase of treatment. Although occurrences were rare, hematologic complications such as aplastic anemia and leukemia were severe. Reduced fertility was also one of the side effects [4]. These complications can occur at any time after RAI and can influence QoL. The reason the “general health” score was lower in the TT with RAI group than in the TT alone group was likely owing to various side effects of RAI. However, because TSH levels in the TT with RAI group were within the reference range, the exact reason for or pathogenesis of the high “felt chilly” score in the TT with RAI group remains unclear. Further research is needed to clarify this mechanism. In terms of the dose, RAI above 5.55 GBq (150 mCi) has been associated with worse QoL [11]. In the present study, the median dose of RAI was 2.96 GBq (80 mCi), but our results showed that even this lower dose of RAI could affect QoL. Therefore, the use of RAI in patients with low-risk DTC or PTMC should be carefully considered and should be decided according to individual risk stratification.
QoL impairment due to treatment may improve with time. One study showed that QoL impairment observed during the first year improved over time after treatment [24]. Another study showed that the QoL scores improved according to the duration of cure [23]. In the present study, we showed reduced QoL parameters in the TT with RAI group compared with those in the TT alone group, even after a median period of 3.7 years following initial treatment. This suggests that the effects of RAI remain for a long time. However, further larger prospective multicenter studies need to confirm these results.
There were some limitations in this study. First, this was a cross-sectional study, in which the questionnaires were conducted at one timepoint without follow-up. Therefore, it is hard to evaluate changes in QoL after treatment, and the results could be influenced by confounding factors. However, to minimize this, we attempted to match TSH levels in both groups, and there were no significant differences in baseline characteristics that could affect QoL. Second, the number of patients was small, which could affect the statistical power. Despite these limitations, this is the first study to demonstrate the effect of RAI on QoL by comparing the TT alone and TT with RAI groups.
In conclusion, patients with PTMC who underwent TT with RAI ablation experienced more health-related problems than those managed by TT alone. This effect was present even after a median period of 4 years since initial therapy and the maintenance of euthyroid status. These findings support the idea that RAI ablation should be carefully considered in patients with low-risk DTCs because it could negatively affect their QoL.
 XML Download
XML Download