

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose cotransporter 2 inhibitors (SGLT2is) are novel glucose-lowering therapies that are prominent in the most recent guidelines for the management of hyperglycaemia in type 2 diabetes mellitus (T2DM) and recommended as preferred second-line pharmacological therapies after metformin, alongside ongoing lifestyle management (predominantly diet and physical activity) [1]. They are particularly recommended when, in addition to glucose lowering, there is a compelling need to reduce body weight (BW) [1].
In large cardiovascular outcome trials, several GLP-1RAs (liraglutide, semaglutide, exenatide once-weekly, albiglutide and dulaglutide) have shown compelling cardiovascular protection in the form of reduced risk of major adverse cardiovascular events, along with some renal benefits [23]. A number of SGLT2is (canagliflozin, dapagliflozin, and empagliflozin) have also shown cardiovascular benefits and greater renal protection, in addition to reduced hospitalization for heart failure [456]. Both classes of therapy also elicit clinically relevant weight loss [1], with liraglutide gaining an independent license (at a higher dose of 3 mg) for use in obesity management. Importantly, the glucose-dependent mechanisms of action of both therapies mean that their beneficial effects come with low risk of hypoglycaemia, particularly when not used with sulphonylureas or insulin [1].
The dual effects of weight loss and improved glycaemic control associated with GLP-1RAs and SGLT2is are appealing. Obesity and T2DM are intrinsically linked, and each are associated with increased risk of multiple comorbidities [7]. Notably, however, previous studies demonstrate that when BW is reduced through dietary energy restriction, not all of the resulting weight loss can be attributed to fat mass (FM), with approximately 25% to 33% estimated to comprise of reductions in lean body mass (LBM) [89]. This is important because LBM (predominantly comprised of skeletal muscle) has several important functions. It acts as a primary site of glucose disposal (with lower skeletal muscle mass contributing to poorer glycaemic control [10]), and is a strong determinant of resting metabolic rate; and thus loss of skeletal muscle with weight loss may predispose individuals to a greater chance of weight regain [11].
Lower muscle mass and function, associated with impaired muscular strength and endurance, also result in a higher risk of falls, hospitalisation and physical frailty [1213]. The important association between T2DM and frailty is becoming increasingly recognised [14], with frailty up to five times more likely in individuals with T2DM compared to those without [14151617]. T2DM represents a state of accelerated metabolic ageing, and some of this frailty risk may be underpinned by an increased loss of LBM and function [181920].
Consequently, whilst weight loss is an important goal in the management of several obesity-associated comorbidities, including T2DM, and pharmacological therapies that support such weight loss are appealing, it is important to understand the impact of these therapies on body composition. The aim of this narrative review is to describe the effects of GLP-1RAs and SGLT2is upon body composition, with a particular focus on LBM and skeletal muscle.
DEFINITIONS AND MEASUREMENT OF BODY COMPOSITION
To interpret changes in body composition, it is important to understand the basic theory and appreciate the advantages and disadvantages of different measurement methods.
Broadly, body composition measurement divides the body into “compartments” on the basis of differing physical properties, which commonly include FM, fat free mass (FFM), LBM, skeletal muscle mass, bone mineral content and total body water (TBW). Definitions of these terms are provided in Table 1.
Direct methods of body composition include computed tomography (CT) and magnetic resonance imaging (MRI) [21]. Whilst these techniques have the highest accuracy, they are also expensive, and not widely used in clinical practice. More common measures, which estimate body composition indirectly, include bioelectrical impedance analysis (BIA), air displacement plethysmography (ADP) and dual-energy X-ray absorptiometry (DXA).
BIA uses a small alternating current to measure body impedance. Estimates of body composition are provided through in-built equations based on assumed impedance of different biological tissues [22]. BIA is quick, easy and relatively inexpensive, but less precise than other available methods and influenced by factors such as hydration status.
ADP provides an estimate of body composition by combining body volume, measured using the displacement of air within a sealed measurement chamber, with BW to calculate body density. Body density is then used to estimate body composition using pre-defined formulae [23]. ADP is relatively quick to perform and non-invasive, but requires operation by trained personnel to avoid undue error.
DXA remains a prominent and preferred technique in clinical trials, balancing a high level of accuracy with comparatively lower costs than MRI and CT. DXA provides whole-body and regional estimates of FM, FFM, LBM, and bone mineral content [21]; using a small safe dose of radiation. It is relatively quick and provides much greater accuracy than BIA.
METHODS
We searched for published studies reporting data on the effects of GLP-1RAs and SGLT2is on body composition using the online database, PubMed, from inception to August 2019, using search terms related to GLP-1RAs, SGLT2is, weight loss and body composition. We included studies using DXA, BIA, ADP, MRI, or CT to measure body composition in any human study population before and after 2 or more weeks of GLP-1RA and/or SGLT2i therapy. Where appropriate, the following assumptions were used during data extraction:
(1) Where data were reported for mean total BW and mean body fat percentage, we estimated mean FM as; BW divided by 100, multiplied by body fat percentage.
(2) Where mean BW and mean FM were available (including when FM was estimated as above) we estimated FFM as; BW minus FM.
We used FFM to cautiously infer changes in LBM, with recognition of their subtle differences as outlined in Table 1. Due to variation in techniques used and methods of reporting, we did not sum different body compartments to estimate total LBM, FFM or BW change.
RESULTS
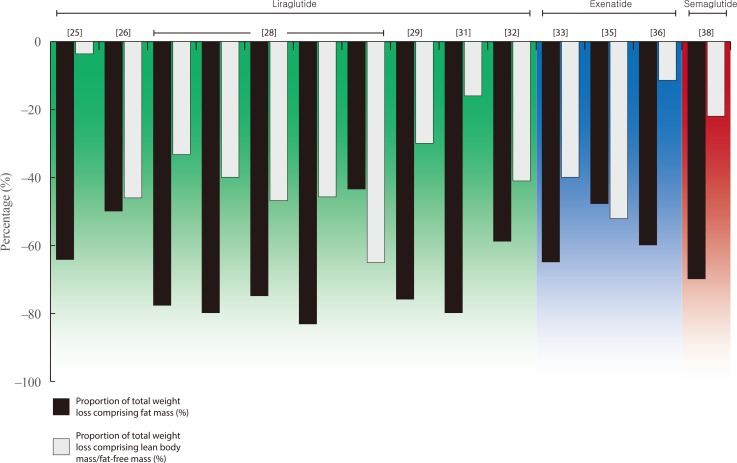
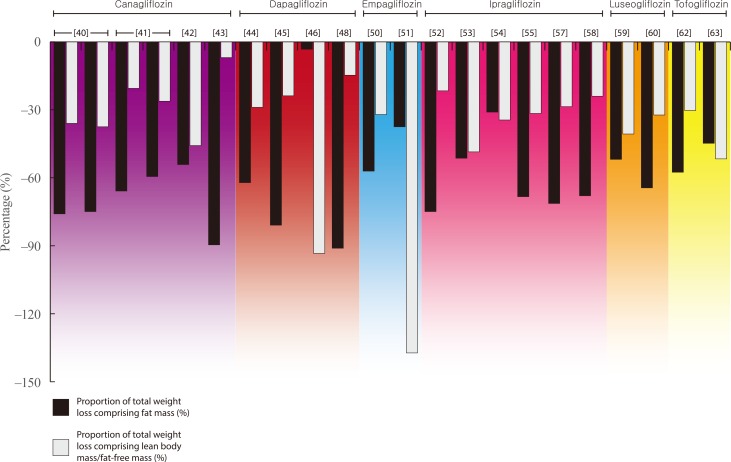
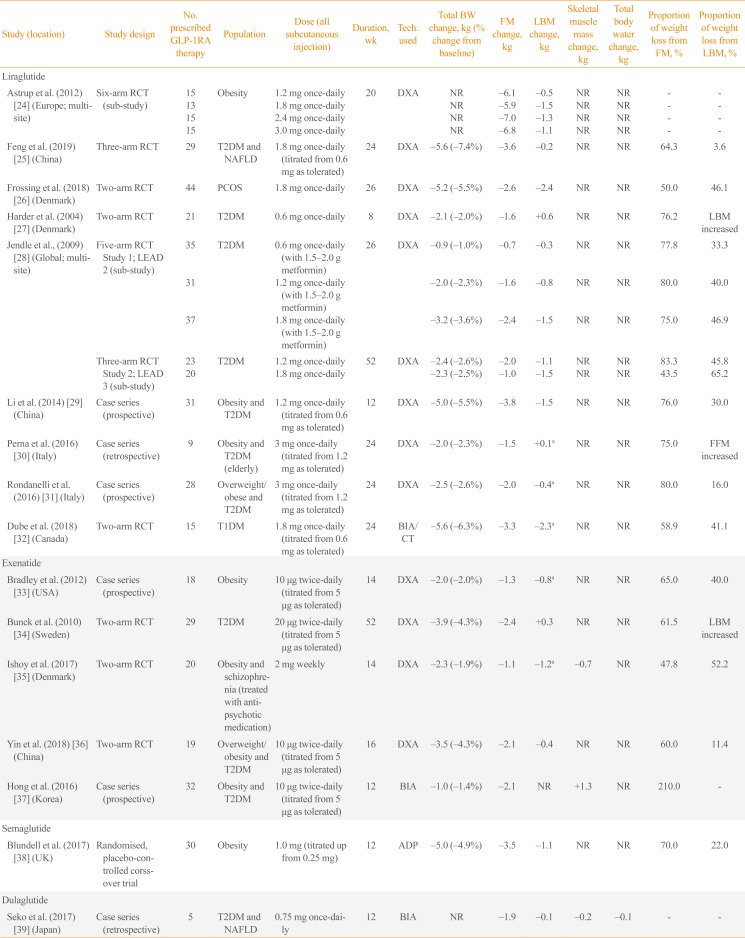
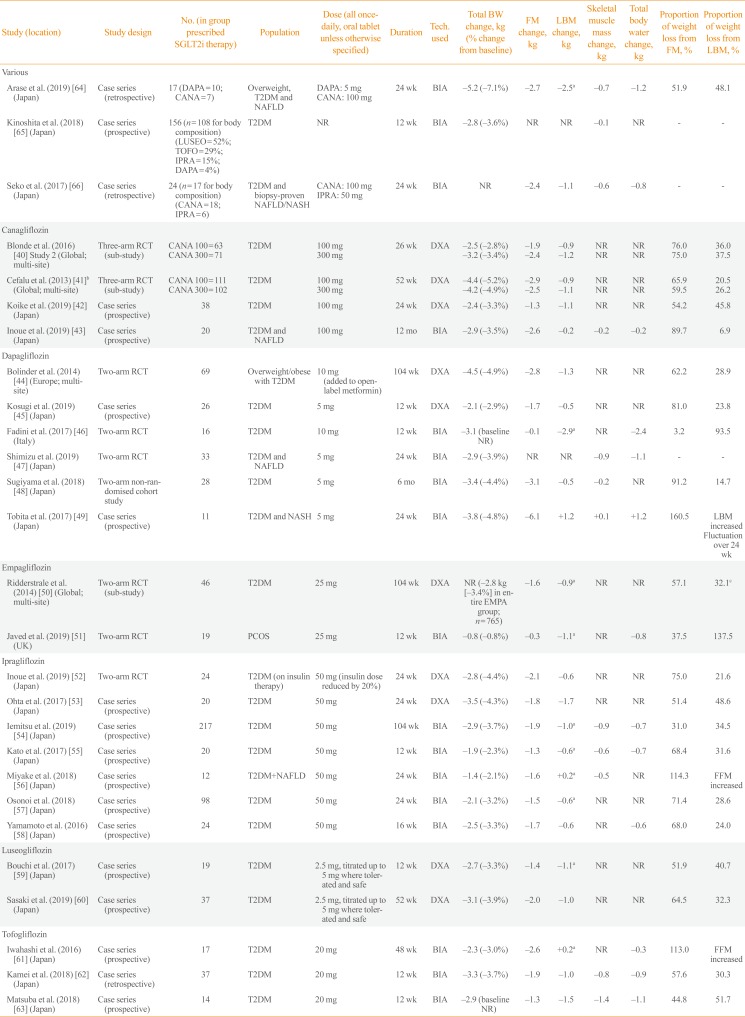
Details of all eligible studies identified in our search can be found in Tables 2,3,4 [242526272829303132333435363738394041424344454647484950515253545556575859606162636465666768]. The following paragraphs provide an overview of the findings for each individual therapy within both drug classes. For ease of reading, medication doses are not included in text unless providing specific context or comparison. Figs. 1, 2 present the relative proportion of weight loss that could be attributed to FM and LBM/FFM with GLP-1RA and SGLT2i therapy, respectively. Our literature search yielded no data for lixisenatide, albiglutide, or ertugliflozin.
Glucagon-like peptide-1 receptor agonists
We identified 17 studies (two within a single manuscript) reporting changes in body composition with liraglutide (n=10), exenatide (n=5), semaglutide (n=1), or dulaglutide (n=1). Thirteen of these studies used DXA to measure body composition, two used BIA alone, one used a combination of BIA and CT, and one used ADP.
Liraglutide
Four manuscripts, containing data from five studies, reported relative contributions of LBM/FFM to total weight loss with liraglutide therapy, ranging from 30% to 47% [26,28,29,32]. This included data from separate sub-studies contained within two phase 3 trials in the Liraglutide Effect and Action in Diabetes (LEAD) programme. In LEAD 2, there was a step-wise increase in the magnitude of both total weight loss (0.9, 2.0, and 3.2 kg) and the relative contribution of LBM (33%, 40%, and 47%) when liraglutide was prescribed at 0.6, 1.2, and 1.8 mg once-daily for 26 weeks [28]. In LEAD 3, 1.2 mg liraglutide elicited 2.4 kg weight loss after 52 weeks, with 46% comprising LBM. Liraglutide 1.8 mg resulted in a similar magnitude of weight loss at 52 weeks (2.3 kg) but the relative contribution of LBM was considerably higher (65.2%). Two further trials using DXA report similar results in individuals with obesity and T2DM (30% of 5.0 kg weight loss over 12 weeks) [29] and polycystic ovarian syndrome (PCOS; 46% of 5.2 kg weight loss over 26 weeks) [26]. Furthermore, a single study, using BIA, reported 5.6 kg weight loss after 24 weeks of liraglutide therapy in individuals with type 1 diabetes mellitus, of which 41% constituted LBM [32].
Conversely, two studies report a comparatively smaller contribution of LBM/FFM to total weight loss with 24 weeks liraglutide treatment in overweight/obese individuals with T2DM (16% of 2.5 kg weight loss with 3 mg once-daily), and those with T2DM and non-alcoholic fatty liver disease (NAFLD) (4% of 5.6 kg weight loss) [2531]. Furthermore, two studies report no change or marginal increases in LBM after 24 and 8 weeks of treatment, respectively [2730]. The final manuscript identified reductions in LBM in individuals undergoing liraglutide therapy at 1.2, 1.8, 2.4, and 3.0 mg for 20 weeks, but did not report total BW change for the subset of individuals undergoing body composition assessment [24].
Exenatide
We identified five studies examining the impact of exenatide on body composition, reporting similar, although more heterogeneous, findings than those for liraglutide. Two studies used DXA to assess changes in body composition with 14 weeks of exenatide treatment in individuals with obesity with or without schizophrenia. These studies reported a mean weight loss of 2.0 and 2.3 kg, respectively, of which the relative contribution of FFM to total weight loss was 40% and 52% [3335].
A separate study reported 3.5 kg weight loss after 16 weeks of treatment in individuals with overweight/obesity and T2DM and reported that 11.4% of weight loss comprised of LBM [36]. One further study reported a small increase (0.3 kg) in LBM after 52 weeks of treatment in individuals with T2DM [34]. The final study identified (utilising BIA to assess changes in body composition over 12 weeks in individuals with obesity and T2DM), did not report changes in LBM, but reported a loss of FM that was greater than the total weight loss induced by exenatide, and a 1.3 kg increase in skeletal muscle [37].
Semaglutide
The only study administering semaglutide reported 5.0 kg weight loss after 12 weeks of treatment in individuals with obesity [38]. Of this weight loss, 20% was estimated, using ADP, to consist of LBM.
Dulaglutide
A single study of dulaglutide reported data from a case series of five individuals assessed before and after 12 weeks of treatment, using BIA [39]. This manuscript did not report total weight loss, but outlined 0.1 and 0.2 kg loss of LBM and skeletal muscle, respectively, in comparison to 1.9 kg loss of FM.
Sodium-glucose cotransporter 2 inhibitors
We identified 27 studies examining changes in body composition with SGLT2i therapy (canagliflozin=4, dapagliflozin=6, empagliflozin=2, ipragliflozin=7, luseogliflozin=2, tofogliflozin=3, and various=3). Compared to the studies identified for GLP-1RAs, there was much greater use of BIA (17 studies), with the remaining 10 using DXA.
Canagliflozin
The most robust evidence of body composition changes with SGLT2i comes from a pair of randomised controlled trials (RCTs) reporting data on the effects of canagliflozin on DXA-derived body composition in individuals with T2DM [4041]. After 26 weeks, canagliflozin resulted in 2.5 and 3.2 kg weight loss at 100 and 300 mg, respectively, with the relative contribution of weight loss attributed to LBM being 36.0% and 37.5% [40]. At 52 weeks, the magnitude of weight loss was numerically greater than at 26 weeks and similar with both doses (−4.4 and −4.2 kg), but the relative contribution attributed to LBM was lower (20.5% and 26.2%, respectively) [41]. A third study using DXA, resulted in 2.4 kg weight loss in individuals with T2DM, of which almost 46% was LBM [42].
A single study, using BIA to assess body composition changes over a longer period of time (1 year), reported the contribution of LBM to a total 2.9 kg weight loss in individuals with T2DM and NAFLD to be lower than the studies above, at just 6.9% [43].
Dapagliflozin
Two studies report changes in body composition with dapagliflozin therapy using DXA, providing similar findings to those for canagliflozin. In a sub-study contained within a large multi-site RCT, total weight loss after 104 weeks of dapagliflozin therapy in 69 participants with overweight/obesity and T2DM was 4.5 kg, of which 28.9% consisted of LBM [45]. A smaller, shorter study reported a lower magnitude of weight loss over 12 weeks (2.1 kg) but with a similar relative contribution of LBM (23.8%) [45].
Three further studies, using BIA, show heterogeneous findings. In a non-randomised trial in which 50 individuals with T2DM were prescribed dapagliflozin or non-SGLT2i therapies for 6 months, the dapagliflozin group lost a mean 3.4 kg of BW, of which 15% constituted LBM [48]. In contrast, a 12-week RCT reported that almost all (94%) of the 3.1 kg weight loss elicited with dapagliflozin was LBM [46], whilst a small cohort study in 11 individuals with T2DM and nonalcoholic steatohepatitis, reported a 1.2 kg increase in LBM after 24 weeks of treatment, despite 3.8 kg weight loss [49].
Empagliflozin
Only two studies report the impact of empagliflozin on body composition. One of these provides DXA-derived data from a sub-study nested within the global EMPA-REG H2H-SU trial; a randomised head-to-head trial conducted as part of the empagliflozin phase 3 programme, which compared empagliflozin with the sulphonylurea glimepiride as second line therapy alongside metformin in individuals with T2DM [50]. Using the weight loss observed in the entire population after 104 weeks (2.8 kg), it was estimated that approximately one-third (32.1%) of weight loss elicited in this trial comprised of FFM.
A separate study using BIA to assess changes with empagliflozin in women with PCOS reported a loss of FFM (1.1 kg) which was greater than the total weight loss elicited (0.8 kg) [51].
Ipragliflozin
Of the seven studies identified for ipragliflozin, six reported that the contribution of LBM/FFM to total weight loss elicited ranged from 22% to 49% [525354555759]. All of these studies were in individuals with T2DM, and included two studies using DXA, reporting 22% and 49% of 2.8 and 3.5 kg of weight loss over 24 weeks, respectively. The remaining four used BIA and in the largest and longest of these studies (n=217; 104 weeks of treatment), the proportion of weight loss attributed to FFM was approximately one-third (34.5%) [54].
In the final study identified, 24 weeks of treatment with ipragliflozin resulted in a loss of FM that was greater than the total weight loss in individuals with T2DM and NAFLD, inferring a small gain (0.2 kg) in FFM [56].
Luseogliflozin
Two studies examining the effects of luseogliflozin on body composition using DXA report similar findings to those outlined above. Both studies were in individuals with T2DM, reporting that 12 and 52 weeks of luseogliflozin therapy elicited 2.7 and 3.1 kg weight loss, respectively. Of this weight loss, 41% and 32% could be attributed to a loss of FFM/LBM [5960].
Tofogliflozin
Three similar studies, each utilising BIA, report data regarding the impact of tofogliflozin in individuals with T2DM. Two assessed changes over 12 weeks, reporting 3.3 and 2.9 kg weight loss, of which 30% and 52%, respectively, could be attributed to LBM [6263]. The third study reported 2.3 kg weight loss in 17 individuals with T2DM despite an estimated 0.2 kg increase in FFM [61].
Various
Three cohort studies (two retrospective, one prospective) report data from participants prescribed SGLT2i therapy, with variation in the exact agent prescribed [646566]. Each utilised BIA to assess body composition, but only one study reported changes in both total BW and FFM. In this study, almost half (48%) of the 5.2 kg weight loss elicited by dapagliflozin (n=10) or canagliflozin (n=7), in individuals with overweight/obesity, T2DM and NAFLD, could be attributed to FFM [64].
Dual therapy of GLP-1RAs and SGLT2is in combination
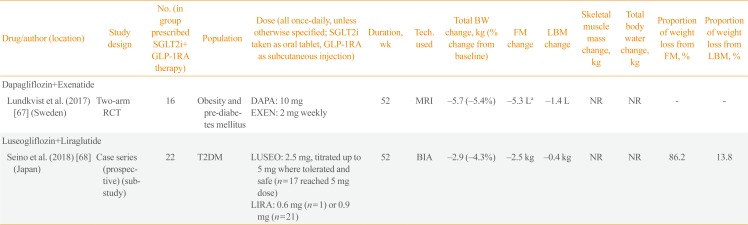
We identified two studies reporting the effect of GLP-1RAs and SGLT2is in combination. In the first, individuals with obesity and pre-diabetes mellitus were randomised to dapagliflozin-plus-exenatide or placebo for 24 weeks, with an open-label extension (during which all participants underwent combined therapy) for a further 28 weeks [67]. Weight loss after 52 weeks was 5.7 kg, with MRI demonstrating reductions in both adipose tissue and lean tissue volumes (5.3 and 1.4 L, respectively). The second study, using BIA, reported 2.9 kg weight loss after 52 weeks of treatment with luseogliflozin-plus-liraglutide, in individuals with T2DM, of which 14% comprised of LBM [68].
CONCLUSIONS
Our review demonstrates that, in most circumstances, the weight loss associated with GLP-1RA and/or SGLT2i therapy comprises predominantly of a reduction in FM. Within 53 groups of individuals prescribed GLP-1RA, SGLT2i or combined therapy, only five groups saw a loss of LBM, FFM, or skeletal muscle mass (depending on reporting) that was greater than FM lost. Thus, in most cases, body composition (i.e., the ratio of FM to FFM/LBM) was more favorable after treatment than before.
However, out of 43 groups in which it was possible to estimate the proportion of weight loss that could be attributed to LBM/FFM, in 27 groups this proportion of LBM lost ranged from 20% to 50%. Six groups saw a loss of LBM, FFM, or skeletal muscle but with a smaller relative contribution to total weight loss (0% to 19%), whilst another six reported an increase in LBM, FFM, or skeletal muscle mass. These results are in accordance with studies of diet-induced weight loss and bariatric surgery, which have reported similar proportions of LBM/FFM (approximately 25% to 40%) within total weight loss elicited [89697071].
There were no clear differences between GLP-1RAs and SGLT2is in the magnitude of weight loss that could be attributed to LBM/FFM. However, it should be noted that the number of studies identified for each class of therapy was relatively small, and these were divided further between multiple therapies within each class. There was also heterogeneity of findings within each drug class and within individual therapies. Reasons for this heterogeneity may include (1) the specific therapy used, (2) the dose or duration of treatment, (3) concomitant therapies alongside GLP-1RA or SGLT2i treatment (e.g., if examined as monotherapy or dual-therapy with other glucose-lowering therapies such as metformin), (4) the clinical diagnoses, background medication usage (i.e., use of sulphonylureas or insulin) and other baseline characteristics of the study population, (5) the technique used to assess body composition (including standardisation procedures prior to measurement), and (6) natural inter-individual variation in responses to weight loss. There are no clear patterns within the data collected in this review, including treatment type, dose or duration and the technique used.
Although the benefits of weight loss in obesity-associated chronic metabolic disease are well established [7273], these favorable outcomes may be limited by losses in LBM, particularly if this constitutes skeletal muscle. Of the studies identified in this review, 12 reported changes in either LBM or FFM, along with changes in skeletal muscle. In seven of these studies, the loss of skeletal muscle comprised between 55% and 100% of the LBM/FFM lost. In one it was twice as great [40], whilst another reported a loss of skeletal muscle despite an increase in FFM [56]. The mechanism of action of SGLT2i, inducing polyuria alongside glycosuria, means that SGLT2i therapy is also associated with fluid loss [1]. Reductions in TBW may impact on body composition measurement, and it could be speculated that reductions in FFM/LBM with weight loss may reflect reductions in water content. Of the 27 studies identified reporting changes in body composition with SGLT2i therapy, 13 reported changes in TBW, 12 of which reported losses; ranging from 0.2 to 2.4 kg (7% to 100% of total weight loss). It is imperative to stress; however, that water is contained within both adipose- and non-adipose tissues [74], and all of the studies reporting TBW in this review utilised BIA. TBW, as provided by BIA, does not allow distinction between water contained in, and thus lost from, different body compartments (i.e., FM or FFM/LBM). No studies reported change in TBW with GLP-1RA or combination therapy.
Consequently, although yielding a more favorable body composition, the potential LBM and skeletal muscle loss associated with weight loss induced by GLP-1RAs and SGLT2is warrants attention. A more rapid decline in skeletal muscle and consequential increased risk of sarcopenia is concerning, particularly as individuals prescribed these therapies are usually already vulnerable to an increased risk of physical frailty (i.e., those with T2DM and/or obesity) [75]. In turn, strategies to preserve or increase skeletal muscle and physical function in these individuals (e.g., through structured exercise training), are of importance. It is also important to state that the absolute mass of skeletal muscle is not the only factor to consider, and improving muscular function (strength, endurance, flexibility etc.) remains critical to improve physical function and performance in tasks of daily living; to impact positively on an individual's quality of life.
Previous studies have shown that markers of physical function (including balance, grip strength, and gait speed) improve following diet-induced weight loss [97677], likely by reducing the biomechanical burden of moving around [78]. However, when diet and exercise are combined, improvements in physical function are greater than that elicited by diet alone, which may be underpinned by preserved or improved skeletal muscle mass and function [979]. Whether the same results are observed when exercise is combined with weight loss elicited by GLP-1RAs and SGLT2i therapy is currently unknown, and requires testing in robust experimental research.
Collectively, the available evidence suggests that the initiation of GLP-1RA or SGLT2i therapy results in weight loss that is primarily derived of FM. However, this is accompanied by reductions in LBM which are not insignificant and should be considered in parallel to changes in FM and overall BW. Differences between therapies are currently unclear. A substantial proportion of LBM loss may be comprised of skeletal muscle, which may be clinically relevant, particularly in the populations to which these therapies are prescribed. Given the heterogeneity, a more consistent approach to measurement and reporting of body composition in future research would be beneficial. As the prevalence of obesity, physical inactivity and associated co-morbidities, including T2DM, continues to rise, it is imperative to explore strategies to preserve LBM and improve physical function, and particularly their interaction with glucose-lowering strategies that positively impact on weight loss.

 XML Download
XML Download