

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetic kidney disease (DKD) is one of the major microvascular complications of type 2 diabetes and a leading cause of end-stage renal disease (ESRD) accounting for one-third of all patients initiating renal replacement therapy (RRT) worldwide [12]. DKD is clinically characterized by persistent albuminuria, progressive decline in renal function, and the development of ESRD [3]. In the development or progression of DKD, prolonged hyperglycemia plays a crucial role through an increase in intracellular glucose metabolism, advanced glycation end products, oxidative stress, and epigenetic reprogramming [4]. In this regard, intensive glucose control has been proven to be effective in preventing or delaying the development and progression of DKD [56]. However, the effects of individual antidiabetic drugs on the kidney have been reported to be different [7].
Dipeptidyl peptidase-4 (DPP-4) inhibitors are a class of antidiabetic agents that potentiate incretin action by reducing degradation of glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide [8]. DPP-4 inhibitors have been used safely in patients with chronic kidney disease, but their effects on renal outcomes are uncertain. Preclinical studies suggested pleiotropic effects of DPP-4 inhibition which might be beneficial to the kidney [8910]. However, in clinical trials, the effects of DPP-4 inhibitors on DKD were inconsistent. In the Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus (SAVOR)-Thrombolysis in Myocardial Infarction (TIMI) 53 trial, saxagliptin significantly reduced urine albumin-to-creatinine ratio (UACR) without affecting renal function [11]. On the other hand, in the Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS) trial, sitagliptin showed a small but early decline in estimated glomerular filtration rate (eGFR) which lasted for 48 months with no difference in changes of UACR [12]. It also should be noted that in those studies renal outcomes were neither primary nor secondary endpoints [1314]. In a study to assess albuminuria-lowering effect as a key efficacy outcome, linagliptin did not have beneficial effects on either albuminuria or renal function [15]. However, generalization of these results would be cautious in that the study comprised patients with relatively early stage of DKD. Indeed, in the SAVOR-TIMI 53 trial, the decrease in albuminuria was greater in patients with lower eGFR [11]. Therefore, to clarify the renal effects of DPP-4 inhibitors, additional method is needed to integrate the results and complement the limitations of individual randomized controlled trials (RCTs), even if they did not initially evaluate renal outcomes.
In the present study, we performed a systematic review and meta-analysis of RCTs to investigate the effects of DPP-4 inhibitors on individual renal outcomes including ESRD compared with placebo or other antidiabetic agents in patients with type 2 diabetes.
METHODS
We conducted the systematic review and meta-analysis based on a prespecified protocol developed by authors (Appendix 1) and reported the results according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement (Supplemental Table S1) [16].
Search strategy and study selection
We searched MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials to identify relevant RCTs published in full-text articles from inception to September 2017 with no restriction of language. The search terms used for DPP-4 inhibitors were DPP-4 inhibitor or DPP-4 inhibitor or alogliptin or anagliptin or evogliptin or gemigliptin or linagliptin or omarigliptin or saxagliptin or sitagliptin or teneligliptin or trelagliptin or vildagliptin.
We included RCTs comparing DPP-4 inhibitors with placebo or other antidiabetic agents in patients with type 2 diabetes. The eligible studies were at least 12 weeks of study duration and reported one or more renal outcomes including changes in UACR or eGFR, and the development of microalbuminuria, macroalbuminuria, doubling of serum creatinine levels, renal failure, ESRD, RRT, dialysis, or kidney transplantation. Pooled analysis for multiple RCTs was also included when it provided additional information on renal outcomes which had not been reported in the original publications. After removing duplicate publications, we screened titles and abstracts, and thoroughly reviewed full-text articles according to inclusion and exclusion criteria.
Data extraction
Two authors (S.K. and N.H.K.) independently extracted data from included studies according to the standardized protocol (Appendix 1). Prespecified outcomes of interests were changes in UACR and eGFR, the development of microalbuminuria (UACR >30 mg/g) and macroalbuminuria (UACR >300 mg/g), regression of albuminuria (defined as the development of normoalbuminuria from microalbuminuria or macroalbuminuria; development of microalbuminuria from macroalbuminuria), and incident ESRD. Any discrepancies were resolved by consensus among the authors (S.K., N.H.K., and S.H.). For continuous variables, mean changes from baseline and their standard deviations were extracted from both intervention (DPP-4 inhibitors) and control (placebo or other antidiabetic agents) groups as summary measures. In a study which reported changes in UACR according to eGFR categories [11], we extracted pooled mean differences between groups. When only mean difference between groups and its P value was reported, we derived the standard error of the mean difference from the test statistic [17]. For dichotomous variables, we extracted the number of patients reporting each renal outcome. In addition, we obtained information about the first author, publication year, number and mean age of randomized participants, duration of follow-up, intervention and comparison treatment, and background antidiabetic agents. For multiple-dose studies, we combined the different dose groups of the same drug into a single group. For three-arm studies, we split a common arm into two groups and considered each pairwise comparison separately.
Assessment of study quality and risk of bias
The Cochrane Risk of Bias Tool was used to assess study quality and risk of bias. Two independent authors (S.K. and N.H.K.) reviewed included studies and judged the risk of bias as adequate (low risk of bias), unclear (unclear risk of bias), or inadequate (high risk of bias) from each of six domains: sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and other sources of bias [18]. Any discrepancies were resolved by the authors (S.K., N.H.K., and S.H.).
Statistical analysis
Standardized mean differences (SMDs) were used for changes in UACR since the results were reported in different scales for this outcome [19]. Hedges' g was used for the estimate of SMDs to take the small number of studies into account [20]. Weighted mean differences (WMDs) and 95% confidence intervals (CIs) were calculated for changes in eGFR. The SMDs were additionally considered for changes in eGFR. Relative risks (RRs) and 95% CIs were calculated to assess effect size for the development of microalbuminuria and macroalbuminuria, regression of albuminuria, and incident ESRD. In the meta-analysis, we calculated a combined estimate and its 95% CI using a random-effects model. Cochran's Q test was used for testing statistical heterogeneity and the I2 statistic was used to measure the degree of heterogeneity [19]. The I2 statistics of 0% to 40%, 30% to 60%, 50% to 90%, and 75% to 100% was regarded as not important, moderate, substantial, and considerable heterogeneity, respectively [19]. We used the funnel plot and Egger's test to address reporting bias for the renal outcome with sufficient number of studies for the exploration [2122]. In prespecified subgroup analysis, we evaluated changes in UACR according to sodium-glucose cotransporter 2 (SGLT2) inhibitors versus non-SGLT2 inhibitors in the control group. All statistical analyses were conducted using STATA version 12 (Stata Corp LLC, College Station, TX, USA). For treatment effects and test for heterogeneity, P<0.05 and P<0.10 were regarded as statistically significant, respectively.
RESULTS
Characteristics of included studies
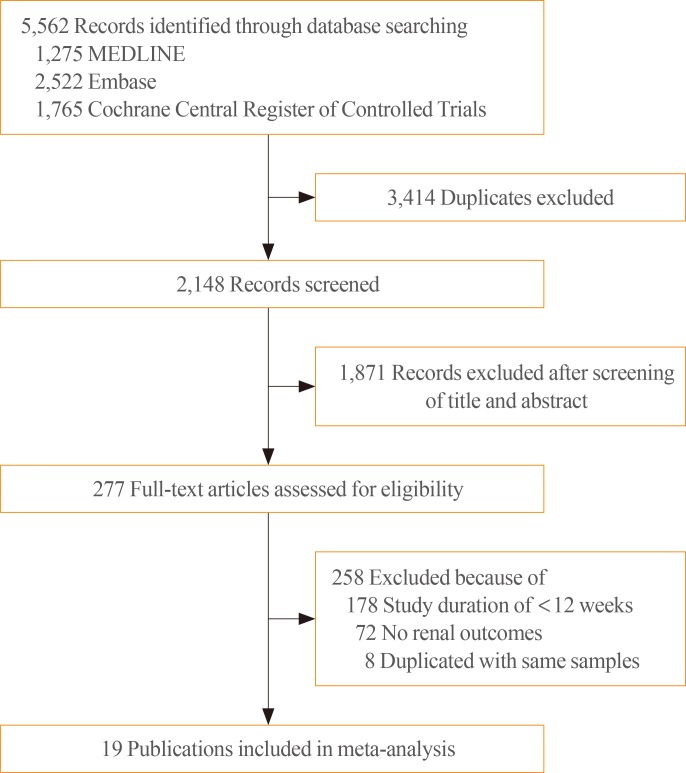
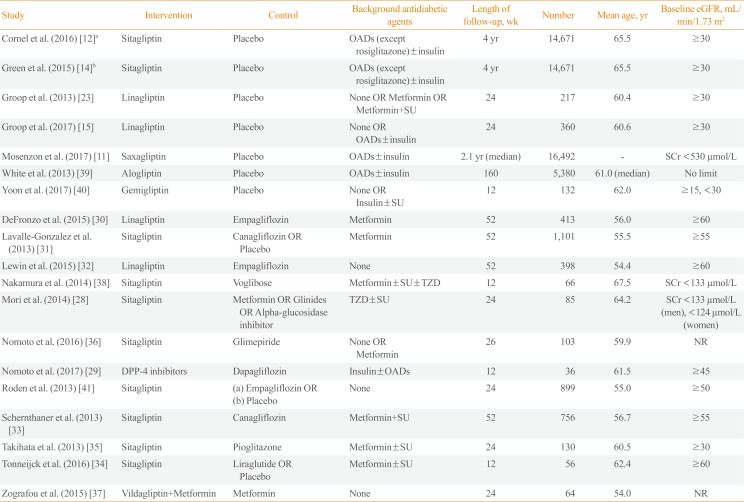
Fig. 1 shows study screening and selection process. Of 5,562 records identified through electronic database search, we included 23 eligible RCTs with 19 publications in the analysis. Two publications [1214] reported different outcomes from the same study [12] and both were included in the analysis. One publication [23] was a pooled analysis of four RCTs [24252627], and another one study was an open-label, prospective RCT [28]. DPP-4 inhibitors were not confined to a specific agent in one study as they were used as a control [29]. Characteristics of the studies are presented in Table 1 [11121415232829303132333435363738394041]. A total of 41,359 participants were randomly assigned to either intervention or control group. The number of participants in individual studies ranged from 36 to 16,492. The study duration of two studies lasted up to 4 years [1214], and one study reported results with a median duration of 2.1 years [11]. The remaining studies had 12 to 160 weeks of study duration. Baseline eGFR of participants was ≥60 mL/min/1.73 m2 in five studies [3031323334] and ≥30 mL/min/1.73 m2 in five studies [1214152335]. Two studies did not describe inclusion or exclusion criteria for baseline eGFR or serum creatinine levels [3637].
Assessment of study quality and risk of bias
Supplemental Fig. S1 summarizes the risk of bias assessment. We evaluated 23 RCTs published in 19 publications (Supplemental Table S2). Fourteen studies reported adequate random sequence generation and adequate allocation concealment. Nine studies did not state sequence generation [232426272829373839] and allocation concealment [232426272836373839]. Twenty-two studies reported adequate blinding of participants and personnel. One study was an open-label RCT [28], but classified as reporting adequate blinding because only objective findings were included in our study. One study did not describe blinding method [38]. Thirteen studies were judged as adequate for completeness of outcome data. Two studies did not clarify the number of participants in the analysis [2337], and eight studies reported incomplete outcome data because of losses to follow-up [1124262729303338]. Four studies [24252627] were integrated into one publication as a pooled analysis [23] and there was the possibility of selective reporting.
Changes in UACR and eGFR
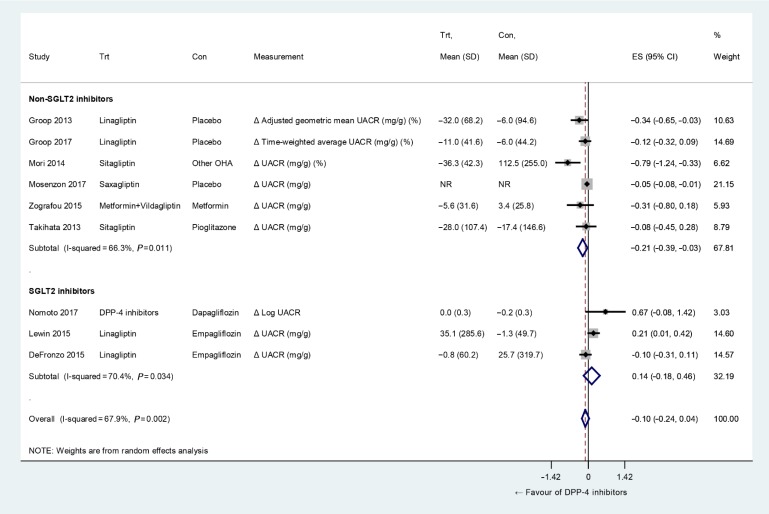
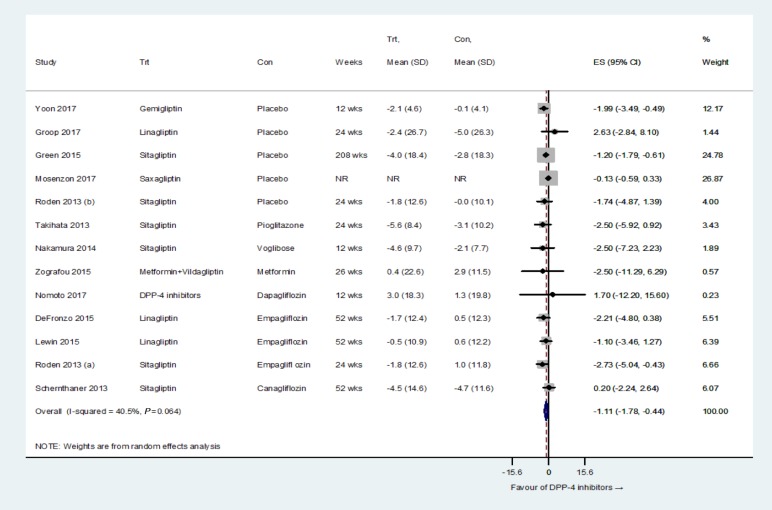
Fig. 2 shows changes in UACR of SGLT2 inhibitors compared with those of control. Overall changes in UACR were not significantly different between groups (P=0.150). The test for heterogeneity showed substantial heterogeneity across the studies (I2=67.9%, P=0.002), and this heterogeneity contributed to asymmetry in the funnel plot (Supplemental Fig. S2A). However, in the subgroup analysis according to the antidiabetic agent in the control group, DPP-4 inhibitors significantly lowered UACR compared with non-SGLT2 inhibitors (P=0.019). Meanwhile, DPP-4 inhibitors insignificantly increased UACR compared with SGLT2 inhibitors (P=0.389). This difference in UACR changes was not statistically significant between the two subgroups (P=0.105). Fig. 3 shows the comparison of changes in eGFR between DPP-4 inhibitors and controls. DPP-4 inhibitors showed a small but significant decline in eGFR compared with controls ([WMD, −1.11 mL/min/1.73 m2; 95% CI, −1.78 to −0.44; P=0.001], [SMD, −0.07; 95% CI, −0.12 to −0.02; P=0.009]). The test for heterogeneity showed moderate heterogeneity across the studies (I2=40.5%, P=0.064 on the test of WMD; I2=43.2%, P=0.048 on the test of SMD). The funnel plot was symmetrical, and Egger's test gave a P value of 0.191 (Supplemental Fig. S2B).
Development, progression, and regression of albuminuria
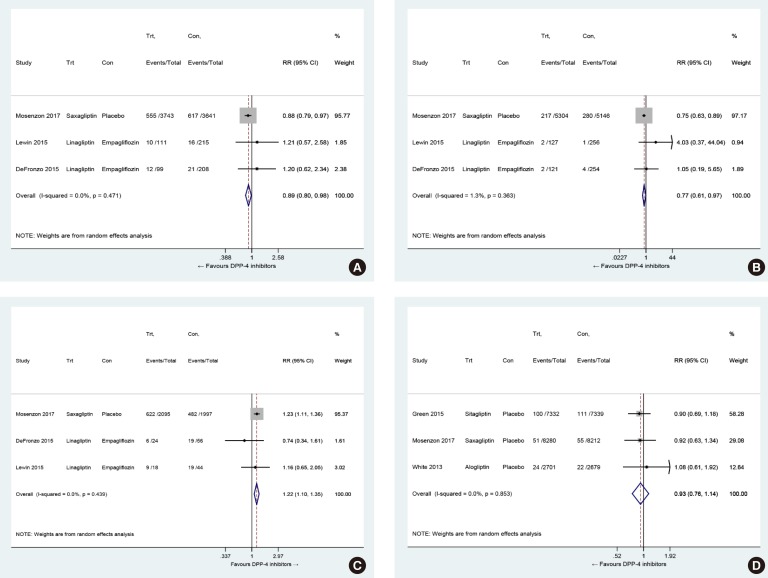
DPP-4 inhibitors significantly reduced the risk of developing microalbuminuria (RR, 0.89; 95% CI, 0.80 to 0.98; P=0.022) and macroalbuminuria (RR, 0.77; 95% CI, 0.61 to 0.97; P=0.027) compared with controls. However, the effects of DPP-4 inhibitors on incident albuminuria were mainly driven by one large trial (Supplemental Fig. S3) [11]. There was no heterogeneity across the studies on both microalbuminuria (I2=0.0%, P=0.471) and macroalbuminuria (I2=1.3%, P=0.363) (Fig. 4A, B). In addition, DPP-4 inhibitors were associated with significantly higher rates of regression of albuminuria compared with controls (RR, 1.22; 95% CI, 1.10 to 1.35; P<0.001) (Fig. 4C). There was no heterogeneity across the studies (I2=0.0%, P=0.439). The tests for funnel plot asymmetry were not performed on albuminuria because of the small number of studies [113032].
Development of ESRD
DPP-4 inhibitors did not reduce the risk of developing ESRD in patients with type 2 diabetes compared with controls (RR, 0.93; 95% CI, 0.76 to 1.14; P=0.475) (Fig. 4D). There was no heterogeneity across the studies (I2=0.0%, P=0.853). Asymmetry in the funnel plot was not evaluated due to the small number of studies [113032].
DISCUSSION
In this systematic review and meta-analysis, we found that DPP-4 inhibitors had beneficial effects on renal outcomes mainly by reducing albuminuria compared to placebo or other antidiabetic agents in patients with type 2 diabetes. On the other hand, DPP-4 inhibitors treatment was associated with a small decline in eGFR compared with controls. The risk of ESRD was not different between groups.
The beneficial effects of DPP-4 inhibitors on albuminuria were consistently demonstrated by reducing the risk of development or progression of both microalbuminuria and macroalbuminuria. These favorable effects were largely driven by the SAVOR-TIMI 53 trial [11]. However, decreases in UACR observed in other clinical trials [2342] supported albuminuria-lowering effects of DPP-4 inhibitors in our meta-analysis. There are several lines of evidence that may explain the mechanism by which DPP-4 inhibitors improve albuminuria. Preclinical studies showed that DPP-4 inhibitors were beneficial to DKD by reducing oxidative stress, inflammation, and histopathologic changes in renal injury [43444546]. Interestingly, linagliptin ameliorated kidney fibrosis in streptozotocin-induced diabetic mice without altering blood glucose levels by inhibition of endothelial-to-mesenchymal transition and restoration of microRNA 29s [47]. An increase in stromal cell-derived factor-1α also contributed to antioxidative and antifibrotic effects of DPP-4 inhibitors [48]. Additionally, DPP-4 inhibitors induced natriuresis in patients with type 2 diabetes [49]. However, they exerted natriuretic effects mainly on distal renal tubule, not on proximal tubule as in SGLT2 inhibitors [4950]. Moreover, natriuretic response to DPP-4 inhibitor was blunted in diabetic mice [51]. Hence, DPP-4 inhibitors could reduce albuminuria through antioxidant, anti-inflammatory, and anti-fibrotic effects without significant changes in renal hemodynamics.
Intriguingly, the direction of treatment effects of DPP-4 inhibitors was different according to the antidiabetic agent in the control group. DPP-4 inhibitors significantly reduced UACR compared with controls other than SGLT2 inhibitors, but they had a tendency to increase UACR when compared with SGLT2 inhibitors. In the development of microalbuminuria and macroalbuminuria, the direction of treatment effects was consistent with changes in UACR, although it was limited due to the small number of studies. These findings suggest that SGLT2 inhibitors might be more effective than DPP-4 inhibitors in reducing albuminuria, which requires further investigation.
We also found that DPP-4 inhibitors marginally decreased eGFR compared with controls. A small decline in eGFR after DPP-4 inhibitor treatment has already been recognized in the TECOS trial [12]. However, it is uncertain that these small changes in eGFR have any clinical implications. Moreover, most of the studies in our meta-analysis had less than 52 weeks of follow-up, which was limited to observe their long-term effects. Different from changes in renal function, DPP-4 inhibitors tended to reduce the risk of ESRD compared with control in the pooled analysis of three large cardiovascular outcome trials, which might suggest favorable effects on the decline in renal function [111439]. In terms of reduction in the risk of ESRD, it has been suggested that DPP-4 inhibitors exerted beneficial effects on multiple risk factors for DKD including albuminuria [112328], inflammation [525354], and endothelial dysfunction [3855] besides glucose-lowering effects.
In line with our findings, the Cardiovascular Renal Microvascular Outcomes with Linagliptin in Patients with Type 2 Diabetes Mellitus (CARMELINA) study group recently announced that linagliptin significantly reduced the risk of albuminuria progression without affecting other renal outcomes including ESRD. The detailed results to be published soon are expected to help understand better the renal effects of DPP-4 inhibitors.
There are several limitations in the present study. First, renal outcomes were not evaluated as prespecified endpoints in most studies included in our meta-analysis. Second, about 40% of included studies had the possibility of selection bias or attrition bias. Third, the number of studies included in the analysis of incident albuminuria or ESRD are relatively small. Thus, the results of our meta-analysis should be interpreted cautiously.
In conclusion, our systematic review and meta-analysis demonstrated that DPP-4 inhibitors had renoprotective effects by reducing the risk of development or progression of albuminuria without affecting the risk of ESRD in patients with type 2 diabetes compared with placebo or other antidiabetic agents.
 XML Download
XML Download