

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity is a growing health problem that contributes to numerous life-threatening or disabling disorders, including heart disease, stroke, type 2 diabetes mellitus (T2DM), degenerative joint disease, obstructive sleep apnea, and certain type of cancers. In particular, morbid obesity (body mass index [BMI] ≥40, or >35 with significant medical problems caused by or made worse by weight as defined by both the National Institute for Health and Care Excellence and the National Institutes of Health, Bethesda, MD, USA) is associated with twice the mortality of the general population. There is also a considerable strain on healthcare resources and society as a whole, with the costs set to rise. Thus, morbid obesity has led to the development of therapies aimed at weight loss.
The treatment options for morbid obesity are lifestyle changes, pharmacotherapy, and surgery. The long-term effects of diet, exercise, and medical therapy on weight have been shown to be largely ineffective at managing morbid obesity. With respect to durable weight reduction, bariatric surgery is the most effective and longest-lasting treatment for morbid obesity, with the greatest chance for amelioration and even resolution of obesity-associated complications. Recent evidence shows that bariatric surgery for morbid obesity is associated with decreased overall mortality (Table 1) [1].
Comorbidity resolution after bariatric surgery occurs in 75% to 90% of cases, particularly for insulin resistance, hypertension, and respiratory disorders [2345]. According to Christou et al. [6], the relative risks of developing cardiovascular, endocrinological (including diabetes), musculoskeletal, genitourinary, psychiatric, respiratory, and hematological disorders were markedly reduced after bariatric surgery. Further, the relative risk of developing cancer in the surgical cohort was 0.21 after bariatric surgery compared with morbidly obese patients who did not undergo operations over a 5-year period.
Diabetic remission after bariatric surgery has resulted in the inclusion of bariatric surgery as a treatment modality for T2DM by the International Diabetes Taskforce. This is why several surgical procedures have been proposed, with all of them leading to a long duration of body weight loss [7].
HISTORY OF BARIATRIC SURGERY IN KOREA
During the past decade, obesity has substantially increased in Korea, leading to dramatic increases in complications such as T2DM. According to Organisation for Economic Co-operation and Development (OECD) Health Data 2014 [8], the overall prevalence of obesity (BMI ≥25.0 kg/m2) in Korean adults is 31.8% (32.4% in men and 29.4% in women). The prevalence of obesity in adults and children has increased rapidly from the 1990s through the beginning of the new millennium and is steadily increasing in parallel with Korea's rapid socioeconomic progress.
With the development of laparoscopic surgery, bariatric surgery has entered the realm of minimally invasive surgery and Dr. Kim WW performed a laparoscopic sleeve gastrectomy for the first time in 2003, which led to the introduction of bariatric surgery in Korea. In the same year, Dr. Kim EK, Dr. Lee SK, and Dr. Choi SH performed Roux-en-Y gastric bypasses (RYGB), followed by a mini-gastric bypass performed by Dr. Hur KY. After approval of the LAP-BAND (Apollo Endosurgery Inc, Austin, TX, USA) by the Korean Food and Drug Administration, adjustable gastric banding (AGB) was introduced by Dr. Kim EK in 2004. In 2009, duodenojejunal bypass for diabetic control was performed by Dr. Kim EK and Dr. Heo YS. Subsequently, Dr. Park DJ introduced robot-assisted RYGB in 2011. In 2005, Prof. Choi YB took part in the Korean Society for the Study of Obesity as a chairman of a bariatric surgery committee composed of physicians, endocrinologists, and family physicians to communicate and exchange opinions regarding bariatric surgery for morbidly obese patients. The Korean Study Group of Bariatric Surgery was formed in 2009 and developed into the Korean Society of Metabolic and Bariatric Surgery (KSMBS) in 2010. In April 2010, the Inaugural Assembly of KSMBS was held in Seoul, and KSMBS began full-scale activities. In 2012, KSMBS was approved as a member of the Korean Surgical Society and became a member of the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). In April 2015, the IFSO-APC was hosted by KSMBS and raised the status of KSMBS to a higher level [9].
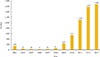
Since the first case of bariatric surgery (laparoscopic sleeve gastrectomy) in 2003, the numbers have substantially increased as well as the type of procedures over the year (from 139 cases in 2003 to 1,686 cases in 2013) (Figs. 1, 2, 3). The number of hospitals practicing bariatric surgery increased from three in 2003 to 29 in 2013 (Fig. 4).
The number of centers performing ≥50 procedures/year has remained stable (5 to 6 since 2010). Conversely, the number of hospitals performing fewer than 10 cases/year has rapidly increased. The procedures that are now accepted as standard include: Lap banding, Lap sleeve gastrectomy (SG), Lap RYGB, biliopancreatic division (BPD), Lap mini-gastric bypass, Lap duodenal switch, and duodenal-jejunal bypass. In 2013, 74% of all procedures were performed in private hospitals, and the most frequent operation was AGB (72%), which has dramatically increased since 2010, followed by SG (14.0%) and RYGB (11.0%) (Fig. 5).
The reasons behind the increase in AGB procedures likely include its technical ease, low rate of complications, and good results in a short-term period. With regard to hospital type, 95% of procedures in private hospital are AGB, while 72% of procedures in university hospitals are SG and RYGB. For patients with diabetes, gastric bypass procedures (RYGB and mini-gastric bypass) were performed in 52% of cases [1011].
Presently, AGB has shown a great decline due to ineffective weight loss, increasing long-term complications, and concern about the rate of band removal (approximately half of patients had to have their band removed) [1213]. Bearing in mind that the most prevalent procedure was ABG, it is likely that band removal will increase steadily in Korea.
In October 2014, a popular Korean rock singer died as a result of medical malpractice. He underwent an operation for intestinal obstruction, following an AGB procedure 5 years earlier by a private doctor. After the accident, the rate of AGB and other bariatric procedures rapidly decreased.
UNIQUE FEATURES OF BARIATRIC SURGERY IN KOREA
Compared to the USA, there are several different factors to be aware of regarding bariatric surgery in Korea [14].
A lack of understanding about morbid obesity and bariatric and metabolic surgery
A large proportion of doctors, the public, and government do not fully understand the necessity and effectiveness of bariatric surgery. They consider bariatric surgery to be an esthetic procedure and thus are unwilling to deal with complications following bariatric surgery. Therefore, many doctors (especially some endocrinologists and family practitioners) are reluctant to recommend bariatric surgery to morbidly obese patients.
It is well-known that bariatric surgery is not an esthetic surgery, and it is confined to patients with a BMI ≥40 or >35 in the presence of significant comorbidities.
The application of medical insurance
There are high costs associated with bariatric surgery due to operation fees, laparoscopic instruments, high-priced endogastrointestinal anastomosis, harmonic scalpels, etc. According to the Korean National Health Nutritional Survey in 2011, morbid obesity became an object of public concern, especially in low-income brackets in which it is difficult to obtain bariatric surgery due to poor economic conditions. It is thus necessary to prepare countermeasures, including a National Medical Insurance system, for such patients.
SURGERY FOR MORBID OBESITY
The ideal surgical intervention for morbid obesity should be effective, safe, and applicable to all patients. It must achieve considerable weight loss and the resolution of comorbidities. Low operative morbidity and mortality are also essential.
For the last decade, laparoscopic procedures have been used in a variety of general surgeries. With the advantages of short hospital stay and rapid return to normal activity, laparoscopic surgery has become the predominant technique in some areas of surgery and has also been used in weight loss surgery.
Current surgical practice can be divided by the mechanism of weight reduction: restrictive by decreasing the storage capacity of the stomach, malabsorptive through surgical bypass to exclude intestinal loops, or a combination of the two [315].
Restrictive procedures
Vertical banded gastroplasty
Originally described by Mason [16] in 1982, this procedure involves the placement of a 5-cm band around a gastric pouch created by stapling the gastric fundus. This procedure has an unacceptable complication rate (14%) [1718], which has led to its widespread disuse, and comparable or better results are achieved with either AGB or gastric bypass. This has led to a shift toward the use of the gastric band as the restrictive procedure of choice.
Adjustable gastric banding
Developed by Belachew et al. [19] in 1994, more than 300,000 gastric bands have been placed worldwide to date. It is the least invasive form of bariatric surgery. Laparoscopic AGB has proven to be fast, effective, and safe in the treatment of morbid obesity. It achieves a gradual controlled and adjustable reduction in weight with excellent results at 2 to 3 years. The technical ease with which the operation can be carried out and the high percentage of acceptance (due to low perioperative mortality, patient perception of it being less drastic, and reversibility) have resulted in it being the most commonly performed bariatric operation globally, despite the dismal long-term results reported by many [202122].
Sleeve gastrectomy
Gastric sleeve surgery is one of the newest procedures and is fast gaining popularity. The surgery makes the stomach smaller so individuals feel full faster. In this surgery, more than half of the stomach is removed, leaving a narrow vertical sleeve, or tube, that is about the size of a banana. Because part of the stomach has been removed, this procedure is not reversible. After surgery, the patient will need to make lifelong changes in eating habits that include eating smaller portions. However, this should not be a challenge because research shows that this surgery causes favorable changes in gut hormones that suppress hunger, reduce appetite, and improve satiety. Sometimes this surgery is performed as the first step prior to duodenal switch surgery if the patient needs to lose a significant amount of weight. With short-term weight loss not far inferior to that of gastric bypass and its better safety profile, this operation is rapidly becoming an attractive option for suitable patients. The fact that the duodenum is not bypassed can improve calcium and iron absorption but might also be a disadvantage because the effect on diabetes may not be as significant as that in gastric bypass. In addition, the remaining stomach can be evaluated with endoscopy, whereas the "defunctional" stomach remaining after a gastric bypass cannot generally be visualized [2324].
Malabsorptive procedures
Jejunoileal bypass
This was the first widely performed operation for obesity and did achieve sustained weight loss in 70% of patients [25]; however, the long-term complications of liver failure (10%), urolithiasis (29%), and renal failure (9%) have led to its abandonmen
Biliopancreatic bypass with or without duodenal switch procedure
BPD is often the procedure of choice for patients with a very high BMI (>60 kg/m2) due to its impressive weight loss profile. Its widespread use is limited by a more severe side effect profile and higher mortality compared with alternative procedures [2627]. Although few centers perform this procedure, BPD may have a role as part of a two-stage procedure, with an initial sleeve gastrectomy and follow-up BPD once a proportion of weight has been lost.
Combined restrictive and malabsorptive procedures
Roux-en-Y gastric bypass
Historically the most frequently performed weight-loss procedure in the United States, RYGB is the gold standard for surgery. The procedure uses a combination of restriction and malabsorption. The surgeon creates a smaller stomach pouch and attaches a Y-shaped section of the small intestine directly to the pouch. This permits food to bypass a large portion of the small intestine, which absorbs calories and nutrients. The smaller stomach pouch makes patients feel fuller sooner and so eat less food; the patient also absorbs fewer calories because the food bypasses a portion of the small intestine.
Gastric bypass achieves excellent initial weight reduction, with a mean excess weight loss (EWL) of nearly 70% at 1 year. A number of case series have shown that, after 3 years, 60% to 70% of patients can achieve >50% weight loss. Long-term results are good, with an average EWL of 60% at 5 years, but this decreases to around 50% at 8 to 10 years. Gastric bypass is also effective in the treatment of "super" obese patients with a BMI ≥60 kg/m2. As with all bariatric procedures, it carries a risk of failure, with 15% of patients failing to achieve or maintain an EWL >50% [2829303132].
A review in JAMA [3] showed that gastric bypass operations lead to more weight reduction, with patients losing an average of 66% of their excess weight, compared to just 45% in those who had gastric banding surgery. Nearly half of patients (48%) reported remission of diabetes 2 years following gastric bypass surgery, while just one-fifth or 17% of gastric banding patients experienced the same results. Nearly 120,000 bariatric procedures are performed each year in the United States, with gastric bypass accounting for nearly 47% of those procedures and gastric banding just 18%.
Mini (omega loop)-gastric bypass
A new development is the laparoscopic mini-gastric bypass procedure, a modification of the older loop gastrojejunostomy. The laparoscopic mini-gastric bypass procedure has been shown to achieve an EWL ≥70% at 2 years, equivalent to RYGB, but long-term data are not yet available [3334]. It is a simpler and easier laparoscopic procedure to perform than RYGB; however, long-term data are still needed to determine whether it can match RYGB in terms of sustained weight reduction and also whether there is an increased incidence of long-term complications such as biliary reflux, marginal ulceration, and reflux oesophagitis.
MECHANISM OF WEIGHT LOSS, DIABETES CONTROL, AND CHANGES IN FOOD CHOICES AFTER BARIATRIC SURGERY
It was formerly thought that bariatric surgery induced weight loss and improved T2DM control simply by restricting meal size and/or by macronutrient malabsorption. However, there is increasing evidence in literature that bariatric operations have profound effects on physiology by reducing hunger, increasing satiety, increasing energy expenditure and promoting healthies food preferences [35]. Moreover, some of these operations improve glucose homeostasis in patients with T2DM (by alternations in circulating gut hormones), independent of weight loss [36].
CONCLUSIONS
It is estimated that there are over 100,000 morbidly obese patients in Korea. We must accept that there is an obesity epidemic; that bariatric surgery is at this time the only reasonable therapy for treating morbid obesity (BMI ≥40 or >35 in the presence of significant comorbidities); and that, in addition to weight loss in relative safety, bariatric surgery ameliorates the medical, social, and economic comorbid conditions of morbid obesity. These outcomes provide for a longer and better life, and they are obtained in a cost-effective manner. In addition, diabetic remission from bariatric surgery has resulted in the inclusion of bariatric surgery by the International Diabetes Taskforce as a treatment modality for T2DM.
It is now time to expedite the inclusion of bariatric surgery as a treatment for morbid obesity by National Medical Insurance for low-income brackets. Also it is necessary to continue developing safe and appropriate bariatric surgical procedures for Asian patients and train qualified bariatric surgeons.





 XML Download
XML Download