

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thyroid hormones play important roles in the regulation of energy metabolism [1]. Hyperthyroidism causes accelerated energy metabolism and consequent weight loss despite hyperphagia [2]. In hypothyroidism, metabolism decreases, resulting in weight gain and decreased appetite. Several studies have evaluated the relationship between thyroid function and insulin resistance (IR) [34]. It is well established that thyroid hormones affect insulin action [5]. Although hyperthyroidism has been consistently found to induce IR, studies regarding the effects of hypothyroidism on insulin sensitivity have produced inconsistent results [678].
Adipocytokines are well known to play a crucial role in the regulation of energy metabolism, feeding, body weight, and insulin sensitivity [9]. Thyroid hormones influence energy metabolism and insulin sensitivity via their interaction with adipocytokines and gut hormones [1011]. Patients with thyroid dysfunction exhibit changes in body weight and insulin sensitivity as well as in adipose tissue metabolism and production of adipocytokines [12]. Altering the circulating levels of ghrelin and leptin influences energy balance and appetite, and they are involved in the development of IR [1314]. Ghrelin is an enteric hormone that exerts its effects on appetite stimulation, energy homeostasis, and, possibly, IR [15]. Several studies have reported that serum ghrelin concentrations are lower in patients with hyperthyroidism than in control groups, whereas serum ghrelin concentrations in hypothyroidism exhibit inconsistent results, being either unaltered or increased [1617]. Leptin has been suggested to be essential for regulation of food intake, body weight, glucose metabolism, and insulin sensitivity [18]. Serum leptin levels are positively correlated with body mass index (BMI), percentage of body fat, and IR indices such as homeostasis model assessment of insulin resistance (HOMA-IR) [19]. Thyroid hormones and leptin affect each other reciprocally, and may regulate body composition and metabolism through complex mechanisms.
The purposes of this study were to evaluate differences in serum ghrelin, leptin, and insulin concentrations according to thyroid hormone levels, and to investigate correlations between IR and anthropometric parameters.
METHODS
Subjects
Thyroid dysfunction patients and euthyroid patients without diabetes mellitus were recruited from the Endocrinology Clinic of the Soonchunhyang University College of Medicine in Bucheon, Korea from September 2011 to June 2012. Patients were evaluated at the time of diagnosis of hyperthyroidism or hypothyroidism. Hypothyroidism was diagnosed by low serum free thyroxine (FT4) and elevated serum thyrotropin (TSH). Hyperthyroidism was diagnosed by elevated serum FT4 and/or triiodothyronine, and suppressed serum TSH, in addition to a determination of increased thyroid uptake or thyroid stimulating antibody. Normal thyroid function was diagnosed by both normal FT4 and TSH. Hypothyroidism was diagnosed on the basis of laboratory findings, low FT4, and elevated serum TSH concentrations.
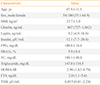
The general characteristics of the study patients are presented in Table 1. Of 154 patients, 100 (64.9%) were women. The mean age of all subjects was 47.9 years, and the mean BMI was 23.7 kg/m2. The participants consisted of 57 hyperthyroid patients (34 women, 23 men), 61 euthyroid patients (42 women, 19 men), and 36 hypothyroid patients (24 women, 12 men). The etiology of hyperthyroidism was Graves' disease. The etiology of hypothyroidism was chronic autoimmune thyroiditis (Hashimoto's thyroiditis, n=33) and thyroidectomy (n=3). Euthyroid subjects consisted of patients admitted for work-up due to thyroid nodules. The study was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine.
Measurements
Height and weight were measured to the nearest 1.0 cm and 1.0 kg. BMI was calculated as body weight (kg) divided by height squared (m2). Blood samples were taken after overnight fasting at the time of diagnosis. FT4 and TSH were measured by radioimmunological determination kit (CIS Bio, Codolet, France). HbA1c was measured by ion-exchange high-performance liquid chromatography (Bio-Rad, Hercules, CA, USA). Serum insulin was measured using an immunoradiometric assay kit. Sera were separated and stored at -80℃ until analyzed. Serum leptin and ghrelin levels were measured using commercially available radioimmunoassay kits (Millipore, Billerica, MA, USA).
IR was calculated using HOMA-IR, by the formula: [fasting insulin (µIU/mL)×fasting blood glucose (mmol/L)]/22.5.
Statistical analysis
Statistical analysis was performed using SPSS version 18 (SPSS Inc., Chicago, IL, USA). Data are reported as means±standard deviation for variables that are normally distributed, as median (interquartile range) for variables that are not normally distributed, or as number of participants (percentages). In the case of non-normally distributed outcome variables, log transformations were applied before statistical testing and subsequently back-transformed. Subjects were divided into three groups, by thyroid function (hyperthyroidism, euthyroidism, and hypothyroidism). We compared the concentrations of ghrelin, leptin, and insulin, and their relation with IR and clinical variables among groups differing in thyroid function using one-way analysis of variance. Between groups, comparisons were performed using post hoc tests through Tukey's honestly significant difference. Pearson correlation analysis was used to analyze correlations between ghrelin, leptin, insulin, thyroid hormones, and clinical variables, including HOMA-IR, in each group. Two-tailed P values <0.05 were considered statistically significant.
RESULTS
Plasma levels of ghrelin, leptin, insulin, and other clinical variables according to thyroid function
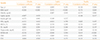
The participants were divided into three groups (57 hyperthyroid patients, 36 hypothyroid patients, and 61 euthyroid patients as a control group). Table 2 shows the differences in the mean levels of ghrelin, leptin, and insulin, and clinical variables, including HOMA-IR, according to thyroid function. There were no differences among the three groups in the mean concentrations of ghrelin (P=0.091) or leptin (P=0.968). There were no significant differences in insulin levels between the groups with thyroid dysfunction and the control group (P=0.06), although hyperthyroid patients showed borderline statistically significant higher levels of insulin than did euthyroid subjects according to a post hoc test (26.4 µIU/mL vs. 16.1 µIU/mL, P=0.057). Regarding IR evaluated by HOMA-IR index, the mean levels in the hyperthyroid group were highest among those of the three groups (hyperthyroid vs. euthyroid vs. hypothyroid, 6.7 vs. 3.8 vs. 4.4, P=0.068). We could not find any significant differences in glucose (P=0.57), HbA1c (P=0.98), total cholesterol (P=0.54), or BMI (P=0.85) among the three groups.
Bivariate correlations between plasma ghrelin, leptin, and insulin, and TSH, free thyroxin, and clinical variables
Bivariate correlations between ghrelin, leptin, and insulin, and thyroid hormones and clinical variables are shown in Table 3. Plasma levels of ghrelin were significantly negatively correlated with age (r=0.253, P=0.002), insulin (r=-0.273, P=0.001), glucose (r=-0.221, P=0.022), BMI (r=-0.306, P<0.001) and HOMA-IR (r=-0.236, P=0.007). Plasma levels of leptin showed significant positive correlation with BMI (r=0.351, P<0.001) and triglyceride (r=0.428, P=0.021). Plasma insulin levels were positively correlated with BMI (r=0.173, P=0.045). Plasma ghrelin levels were not correlated with leptin (P=0.935). Leptin levels were also not correlated with insulin levels (P=0.217). There were no statistically significant correlations among thyroid hormone, TSH, ghrelin, leptin, and insulin.
TSH showed positive correlation with BMI (r=0.259, P=0.004) and total cholesterol (r=0.316, P=0.006) (data not shown). FT4 levels showed negative correlation with BMI (r=-0.215, P=0.019) and total cholesterol (r=-0.358, p=0.002), and positive correlation with glucose (r=0.249, P=0.006) (data not shown).
DISCUSSION
In our study, we found no differences in mean plasma levels of ghrelin, leptin, or insulin among the three groups (hyperthyroid, euthyroid, and hypothyroid). The hyperthyroid group was more insulin resistant than the euthyroid or hypothyroid group, although this was of statistically borderline significance.
Several studies have evaluated the relationship between thyroid function and insulin sensitivity, with conflicting results. In hyperthyroidism, the association with IR is well established. Increased plasma thyroid hormone levels impair the ability of insulin to suppress hepatic glucose production and to increase glucose uptake in peripheral tissues (mainly skeletal tissue) [520]. Hyperthyroidism is associated with increased activity of the sympathetic nervous system, which may influence glucose homeostasis and insulin sensitivity [21]. Our present study showed that hyperthyroid patients tend to have higher IR than do euthyroid subjects. This result is consistent with previous studies [56]. While hypothyroidism was associated with normal insulin sensitivity in some studies, other studies showed an association with IR [4782223]. This present study showed that IR in hypothyroidism patients was not different from that in euthyroid or hyperthyroid patients. Harris et al. [22] reported that the sensitivity of glucose disposal to insulin in the forearm muscles of hypothyroid patients was normal. On the other hand, recent studies have reported that IR exists not only in overt hypothyroidism but also in subclinical hypothyroidism [47823].
Hypothyroid patients commonly have hypercholesterolemia and hypertriglyceridemia. Whereas, in hyperthyroidism, serum total cholesterol, and triglyceride levels are decreased [24]. These are well-known clinical phenomenon. However, results of our present study are not consistent with generally known features. Total cholesterol levels were not different among three groups and triglycerides levels were significantly higher in hyperthyroid group than other two groups. We found very high plasma triglyceride levels above 400 mg/dL (461, 629, and 652 mg/dL) in three subjects. All of them were hyperthyroidism. These cases may induce significant higher levels of triglyceride in patients with hyperthyroidism. Two patients were frequent alcohol drinker and one patient had no specific medical or social history. In addition, prevalence of taking of lipid lowering agents such as statin and fibrate was not different between groups. After excluding three cases, we reanalyzed triglyceride levels among three groups. The mean levels of triglyceride were statistically insignificant among three groups (P=0.676).
Ghrelin and leptin are two hormones that may have a significant impact on energy balance [14]. Studies on ghrelin and leptin levels in human thyroid dysfunction yielded highly variable data and inconsistent results. In our study, we did not find any significant differences with respect to mean plasma ghrelin concentrations among subjects with hyperthyroidism, with hypothyroidism, and with euthyroidism, although serum ghrelin concentrations in euthyroid subjects were insignificantly higher than in subjects with thyroid dysfunction. Ghrelin is an enteric, acylated 28-amino acid peptide hormone, and a ligand of growth hormone secretagogue receptor [25]. Ghrelin is understood to increase food intake and body weight under conditions such as decreased food intake [14]. Hyperthyroidism generally causes weight loss despite increased caloric intake, and induces negative energy balance. Therefore, it would be expected that serum ghrelin levels would be high in hyperthyroidism, as a response meant to restore energy balance. However, several studies have found lower serum ghrelin levels in subjects with hyperthyroidism than in euthyroid participants [16172627]. These reported that the decreased ghrelin levels became normalized after treatment of hyperthyroidism. There are several suggested hypotheses for lower ghrelin levels observed in hyperthyroidism. In a hyperthyroid state, IR and compensatory hyperinsulinemia is induced [567]. Although there has been a contradictory report [28], previous studies have shown that insulin may inhibit ghrelin secretion [162628]. Moreover, Broglio et al. [29] and Tong et al. [30] showed that acute administration of ghrelin induced an inhibitory effect on insulin secretion. Amini et al. [31] investigated the association between circulating ghrelin and IR in a large population-based study. High circulating ghrelin is associated with lower IR in the general population, except among postmenopausal women. We found a significant negative correlation between plasma ghrelin and insulin levels and HOMA-IR. In addition, ghrelin had a significant negative correlation with BMI and glucose. Our results are in agreement with a previous study [16]. Another possible explanation is that there may be an increased metabolic clearance rate effect in the hyperthyroid state, as has been shown for other hormones [3233]. As well, it is known that hyperthyroidism is associated with increased activity of the sympathetic nervous system and with abnormalities in the growth hormone/insulin-like growth factor 1 axis, which may affect glucose homeostasis, insulin sensitivity, and ghrelin levels [34].
Increased levels of ghrelin have been observed in hypothyroid patients, and these levels returned to normal upon L-thyroxine treatment [1735]. However, a study by Sadegholvad et al. [36] found that ghrelin levels did not change significantly in patients with hyperthyroidism or hypothyroidism following treatment. Moreover, the serum ghrelin levels of those patients were not different from those of the control group [36]. Studies by Tanda et al. [37] and Gimenez-Palop et al. [16] similarly found no correlations between changes in ghrelin levels and thyroid hormone levels. These results were consistent with those of our study. In this study, we observed a significant inverse correlation between ghrelin and age. The effect of age on plasma ghrelin levels is still unclear.
Leptin is a 167-amino acid anorexigenic hormone produced by adipocytes that regulates energy consumption and body weight [14]. A correlation between thyroid hormone and leptin has been demonstrated in several studies. Both thyroid hormones and leptin affect each other and may regulate body composition and metabolism by complex mechanisms. TSH stimulates leptin secretion by a direct effect on adipocytes, probably via TSH-receptors on the surface of adipocytes [38]. Serum thyroid hormones also seem to affect leptin levels.
However, in a study by Braclik et al. [17] on serum leptin concentrations among premenopausal women with hyperthyroidism, hypothyroidism, or no thyroid dysfunction, leptin levels were similar before and after treatment of their abnormal thyroid status. Furthermore, no correlation was observed between serum thyroid hormone concentrations and leptin levels [17]. This is consistent with our study's results.
Leptin is known to improve peripheral insulin sensitivity and modulate pancreatic β-cell function [33]. However, in disagreement with other studies, our study found no significant association between leptin levels and insulin levels or IR. In agreement with previous studies, however, we found a significant positive correlation between serum leptin levels and BMI and triglycerides [19].
Leptin has anorexic activity, but ghrelin has an orexic effect. Therefore, it has been postulated that leptin might affect plasma ghrelin levels through the suggested mechanism of suppression of ghrelin secretion. However, studies have found conflicting results. Tschop et al. reported that fasting plasma ghrelin levels are negatively correlated with plasma leptin levels, whereas fasting ghrelin and leptin levels were not correlated in another, obese population [394041]. No such study has been reported in thyroid dysfunction subjects. In this present study, we did not find any significant correlation between them according to thyroid function. We think that neither hormone has a direct influence on the other's levels.
The discrepancies between these results and those of previously reported studies on ghrelin, leptin, and insulin levels according to thyroid dysfunction could potentially be explained by differences in participants' characteristics, changes in energy expenditure and fat mass, degree and duration of thyroid dysfunction, and variability in the assays. In addition, published studies have revealed that there is a very wide range in concentrations of the above mentioned hormones in the population. The large standard deviation of hormone concentrations would require a very large sample size to achieve the statistical power necessary to detect an association among ghrelin, leptin, and thyroid dysfunction. This sample size factor could be an important factor, as previous studies may have been underpowered, and hence yielded discordant results.
There are several limitations to this study. First, we measured leptin, ghrelin, and insulin levels once. We did not compare hormone levels before and after treatment. Because we found no differences in mean serum hormone levels among the three groups at baseline, it may not be necessary to compare those levels before and after treatment. In spite of that, it would have provided more information about the relationships between leptin, ghrelin, insulin and thyroid function. Second, the sample size of our study was relatively small. However, many previous studies have consisted of approximately 100 to 200 subjects. A larger number of patients should be analyzed for the confirmation of our results. However, our study is meaningful in that this is the first study in Korean patients on the evaluation of serum concentrations of ghrelin, leptin, and insulin, and their correlation with IR according to thyroid hormonal state.
In conclusion, serum ghrelin, leptin, and insulin levels did not differ according to the state of thyroid function. Regarding IR, the mean levels of HOMA-IR in the hyperthyroid group were the highest among the three groups. Future studies with larger numbers of patients are required to establish a direct relationship between plasma ghrelin and leptin concentrations and the nature or severity of thyroid function.

 XML Download
XML Download