

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thyroid carcinoma is the most common endocrine malignancy [1]. Although the treatment of choice has been conventional open thyroidectomy (OT), this method inevitably results in neck scars due to the anatomical location of the thyroid gland. To avoid cosmetically undesirable outcomes, various remote approaches have been utilized for patients with low risk of recurrence, the two most common techniques being the transaxillary approach (TAA) and bilateral axillo-breast approach (BABA).
In the TAA, the patient's lesion-side arm is raised over the head, and a 5- to 6-cm vertical skin incision is made in the axilla. Surgical instruments are inserted through a subcutaneous skin flap running from the axilla to the anterior neck, with surgery continuing from the lateral side (Fig. 1) [2]. In contrast, BABA uses two 0.8-cm-sized axillar incisions and two circumareolar incisions, measuring 0.8-cm on the left and 1.2-cm on the right side. The 1.2-cm circumareolar incision is used as a camera port and can be moved to the left side if the surgeon prefers [3]. Both the TAA and BABA techniques were originally developed for endoscopic surgery, but they have been generally replaced by robotic surgery since the adoption of the Da Vinci robotic system in 2007. Robotic surgery has advantages over endoscopic surgery, including superior field of view, ergonomic improvement, and learning curve [4,5]. The merits of the robotic system, including high-definition three-dimensional imaging, high degree of freedom of motion, and a tremor filtering system, have increased the popularity of robotic thyroidectomy (RT).
Despite many studies reporting that RT is effective and safe in patients with thyroid cancer, not all thyroid surgeons advocate RT. RT has several disadvantages, including being costly, technically demanding, and requiring advanced training [6]. To date, however, no randomized controlled study has compared RT with OT. This review of previously published studies compares the outcomes of RT with those of OT.
COSMETIC OUTCOMES OF ROBOTIC THYROIDECTOMY
The most important motivation for patients to choose RT is the absence of neck scarring. For example, a prospective questionnaire study of 41 patients who underwent RT and 43 patients who underwent OT evaluated cosmetic satisfaction 3 months postoperatively [7]. In a second study, cosmetic satisfaction was assessed after 1 day, 1 week, and 1 or 3 months in 75 patients who underwent RT and 226 who underwent OT [8]. In both studies, cosmetic satisfaction was greater in the RT than in the OT group at all recorded time points. Cosmetic satisfaction in patients who underwent modified radical neck dissection (MRND) was also higher in the RT than in the OT group [9]. Thus, the cosmetic benefits of RT seem to be established.
POSTOPERATIVE PAIN AFTER ROBOTIC THYROIDECTOMY
Since RT requires the formation of a larger skin flap than OT, concerns have arisen that postoperative neck and chest pain may be greater after RT. Contrary to this assumption, levels of pain were similar after RT and OT. For example, a questionnaire evaluation of patients 24 hours after thyroidectomy found no significant difference in pain after RT and OT [7]. Another study evaluating pain on a visual analogue scale 30 minutes, 4 hours, and 1, 2, 3, and 10 days after RT or OT found no difference in analgesic use, with the pain score being lower in the RT group than in the OT group at 1 and 2 days after surgery [10]. An evaluation of neck and chest pain found that neck pain was similar in the RT and OT groups, although anterior chest pain was significantly greater in the RT group [8]. However, chest pain score in the RT group was lower than neck pain score in both groups.
SURGICAL SAFETY
Recurrent laryngeal nerve injury
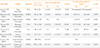
Table 1 shows the incidence of transient and permanent recurrent laryngeal nerve injury (RLNI) who underwent robotic or OT. Most of the studies defined transient RLNI as hoarseness or vocal cord palsy persisting less than 6 months. Six studies comparing RT with OT found similar rates of transient/permanent RLNI [7,8,11,12,13,14]. The incidence of transient RLNI in patients who underwent RT varied from 0% to 20%, with most studies reporting a rate less than 15%. Permanent RLNI was observed in only 0.2% to 0.3% of the patients [4,15,16,17,18], a rate comparable to that of open surgery [19].
Hypoparathyroidism
Although the definition of hypoparathyroidism differs among studies, it is generally based on parathyroid hormone, calcium level, or on hypocalcemic symptoms (Table 2). In most studies, a diagnosis of permanent hypoparathyroidism required the condition to last more than 6 months. In six studies comparing RT and OT [7,8,11,13,14,17], the incidence of permanent hypoparathyroidism was similar in the two groups, although one study [17] reported a higher rate of transient hypocalcemia in the RT group.
Other complications
Other rare complications are described in Table 3. Unique complications associated only with RT included brachial injury and skin flap perforation, although their incidence was only 0.1% in the study with the largest patient population [18]. Bleeding is considered a major complication of both RT and OT, but hematomas requiring reoperation were uncommon in the RT group [4,8,12,18].
Sensory changes
Since RT requires the formation of a larger skin flap than OT, RT may be accompanied by sensory changes in the corresponding skin area. For example, an evaluation of cutaneous light-pressure thresholds in patients who underwent BABA RT found sensory changes in the anterior chest area; however, these became normalized 3 months after surgery [20]. Similar results were observed in patients who undewent TAA RT. Two studies prospectively comparing sensory changes in patients who underwent TAA RT and OT found that sensory changes in the anterior neck area were similar or more common in the OT group, whereas sensory changes in the anterior chest were more common in the RT group. Anterior chest discomfort in the RT group became comparable with that in the OT group 1.5 years after surgery [21]. Sensory changes, therefore, were considered fairly minor.
SURGICAL COMPLETENESS
Among the clinical parameters used to evaluate surgical completeness after thyroidectomy are the number of retrieved lymph nodes, stimulated thyroglobulin (sTg) concentration, and raidioactive iodine uptake (RAI) on whole body scans (WBS).
Lymph node retrieval
Since papillary thyroid carcinomas metastasize via the surrounding lymph nodes, central lymph node dissection is routinely performed in most centers in order to assure oncological safety. In most studies, the numbers of retrieved central lymph nodes were comparable during RT and OT (Table 4). In two studies [8,14], however, the absolute number of retrieved lymph nodes was lower in patients undergoing RT than OT (4.4±2.4 and 8.7±5.1, respectively), although the absolute numbers of the former were similar to those in other studies.
Stimulated thyroglobulin level
sTg level is measured before RAI treatment after elevating thyroid stimulating hormone (TSH) either by thyroid hormone withdrawal or by injection of recombinant human TSH (Thyrogen, Genzyme, Cambridge, MA, USA). Elevated sTg after total thyroidectomy suggests the presence of remnant thyroid tissue; therefore, low sTg is a good indicator of complete thyroid removal. Table 4 shows the results of sTg at the first RAI treatment after RT or OT. While four studies (three BABA, one TAA) reported similar sTg levels in these two groups [11,14,22,23], the other two studies (both TAA) reported that sTg was significantly higher in the RT than in the OT group [8,17]. However, in these two studies, sTg levels turned out to be similar after stage subclassification [17] or after the first RAI treatment [8].
Whole body scan
Remnant thyroid tissue can also be measured by thyroid uptake count ratio on WBS. For example, in one study, RAI uptake in the thyroid bed was higher in the RT than in the OT group when assessed by WBS [23]. The higher uptake in the RT group may have been due to the characteristics of TAA, in which removal of the contralateral thyroid gland is made difficult by the unilateral approach. However, RAI uptake was similar in the RT and OT groups at the second WBS after the first RAI treatment. In contrast, when BABA RT and OT were compared after propensity score matching to minimize selection bias, RAI uptake was similar at the first WBS in the two groups [22].
ROBOTIC THYROIDECTOMY IN CERTAIN DISEASES
Robotic thyroidectomy in Graves disease
Graves disease has been regarded as a contraindication for endoscopic thyroidectomy or RT because bleeding control is hampered by the narrow operative view, hypervascularity, and the large-sized thyroid gland. However, recent technical advances and accumulated experience have enabled RT in patients with Graves disease. Kwon et al. [24] reported successful RT in 30 patients with Graves disease, with a tolerable complication rate. In the study, one patient experienced permanent hypoparathyroidism, but none had major complications such as bleeding, open conversion, or permanent RLNI. The other retrospective study comparing RT and OT in Graves' disease patients [25], in which those with smaller-sized thyroid underwent RT, found no significant between-group differences in operation time, blood loss, or complication rate. RT might be performed safely in selected Graves' disease patients.
Robotic modified radical neck dissection in thyroid carcinoma patients
Robotic surgery has also been utilized for MRND [26]. Since extensive incision scars are inevitable in patients undergoing traditional MRND, robotic MRND may be a good alternative to avoid scarring. Both TAA and BABA have shown outcomes similar to open conventional MRND. For example, a similar number of lateral lymph nodes was retrieved following BABA robotic and open MRND, without causing hypocalcemia, RLNI, or bleeding [27]. In addition, a comparison of patients undergoing TAA or open MRND reported similar complication, surgical completeness, and recurrence rates [9].
CONCLUSIONS
RT offers better cosmetic satisfaction to patients than OT, and RT is as safe and effective as OT in thyroid cancer patients, with similar complication rates. RT also showed similar oncologic safety as OT, as assessed by lymph node harvest, complete removal of thyroid tissue, and RAI success rates. RT is a good alternative surgical modality for patients who wish to avoid neck scars.




 XML Download
XML Download