

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometrial cancer (EC) is the third most common gynecologic cancer in Korea. Its incidence and mortality are increasing gradually, with more than 1,700 new cases are diagnosed and approximately 250 related deaths occurring annually [12]. Treatment of EC with hysterectomy including bilateral salpingo-oophorectomy in premenopausal women can cause estrogen deficiency symptoms such as hot flashes, sleep disturbance, depressive mood, vaginal atrophy, dyspareunia, and urinary tract symptoms. Such menopausal symptoms may considerably affect greatly the quality of life after cancer treatment.
To our knowledge, while no scientific data is available to demonstrate the detrimental effect of hormone therapy (HT) in EC survivors, HT administration has traditionally been contraindicated in EC survivors because of concerns regarding recurrence. It has been assumed that estrogen promotes EC recurrence and, hastens metastases. However, some investigators have reported that HT has had no negative effect on recurrence and overall survival (OS) after EC treatment, although the sample sizes have not been large enough to explain the effect of HT on EC recurrence in most studies [3456].
Drospirenone (DRSP) is a novel progestin with a chemical structure resembling that of 17 α-spironolactone. DRSP in humans has been shown to act as a progesterone receptor (PR) agonist, a mineralocorticoid receptor and an androgen receptor antagonist, while exerting no effect on glucocorticoid or estrogen receptors (ERs) [7]. In addition, the use of 2 mg DRSP with 1 mg 17β-estradiol (E2) (DRSP/E2) as a low dose, continuous combination hormone replacement therapy induces menopausal symptom relief, and has positive actions on metabolism and improves the lipid profile [8]. The combination of DRSP and E2 is also effective in protecting against endometrial hyperplasia [9].
In the present study, we retrospectively evaluated the oncologic safety of DRSP/E2 in EC survivors who underwent surgical oophorectomy.
MATERIALS AND METHODS
The study proposal was finalized and approved by the Institutional Review Boards of each institution (GBIRB2017-230). This study was a retrospective observational matched case-control study. The study group consisted of all EC patients who had undergone primary surgical treatment at the Department of Obstetrics and Gynecology, Gachon University Gil Medical Center, Incheon, Korea, at the Department of Obstetrics and Gynecology, Ehwa Womans University Mokdong Hospital, Seoul, Korea and at the Department of Obstetrics and Gynecology, Kyoung-Hee University Hospital, Seoul, Korea between March 2006 and December 2014. All the patient underwent complete surgical staging with total hysterectomy, bilateral salpingo-oophorectomy, retroperitoneal lymph node dissection and peritoneal washing cytology. Postoperative adjuvant treatment was administered according to the institution's policy and the surgeon's preference, with reference to the pathological diagnosis. The tumor stage and histologic diagnosis of each patient were classified under International Federation of Gynecology and Obstetrics (FIGO) 2009 criteria and the World Health Organization histologic type classification system, respectively. The tumors were graded as well-differentiated (G1), moderately-differentiated (G2), or poorly differentiated (G3).
Study patients were defined as those undergoing DRSP/E2 (Angeliq®; Berlex, Berlin, Germany) treatment who had been diagnosed with stage I/II EC and with an endometrioid histologic type diagnosis. Control patients were defined as those not undergoing. For each study patient, 2 controls (those not undergoing HT) were randomly chosen from each unit's database. The control group was matched with a priority order of operation date and stage. Exclusion criteria were as follows: patients having undergone incomplete surgical staging, those with stage III/IV EC, those classified as non-endometrioid histologic type, patients with inadequate medical records, and patients who had previously been treated with HT.
Data regarding study patients and controls were obtained using electronic patient medical records, and data on the following parameters were collected: age, parity, body mass index (BMI), status of menopause at the time of diagnosis, stage, grade, status of lymphovascular space invasion (LVSI), largest tumor diameter, preoperative cancer antigen 125 (CA 125) level, hormone receptor status, adjuvant treatment modality, use of HT, date of recurrence or death, site of recurrence and last follow-up date.
All HT users received Angeliq® to relieve their climacteric symptoms after surgery (study patients). The HT users started on one tablet of Angeliq® daily within 8 weeks after surgical treatment. The median duration of HT use was 59.7 months (range, 23–124 months). Medication such as calcium supplements, antidepressants and antihypertensives were permitted, but other hormonal agents such as estrogen, progesterone and other selective ER modulators were not permitted. The patients were followed up once every 3 months for the first 2 years after treatment, and once every 6 months thereafter. A computed tomography scan was performed every 6 to 12 months or when clinically indicated. Mammography and breast ultrasonography were undertaken every 12 months.
1. Statistical analysis
This study was designed as a retrospective, case-controlled study, and the case-control ratio was 1:2. To reduce selection bias, propensity score matching was performed. The study patient group was 1:1 matched according to age, FIGO stage, grade, BMI, and tumor diameter with the closest propensity patients who did not undergo HT. Propensity scores were calculated using a multivariate logistic regression model based on factors that demonstrated significant differences between the groups. Case-control differences were evaluated using the Student's t-test or the Mann-Whitney U test for continuous variables and the χ2 test for categorical variables. A Cox proportional hazards model was utilized for analysis of prognostic factors. Survival curves were generated using the Kaplan-Meier method. Comparison of survival curves was performed using the log-rank test. A 2-sided p-value of less than 0.05 was considered significant, with a 95% confidence interval (CI). The statistical analysis was performed using SPSS software for Windows (version 18.0; SPSS Inc., Chicago, IL, USA) and Web-based analysis with R version 3.1 (R Foundation for Statistical Computing, Vienna, Austria; http://www.r-meta.org:3838/betam3/).
RESULTS
1. Patient characteristics
During the study period, EC surgery was performed in 564 patients. Of these, 219 patients were eligible for inclusion. The exclusion criteria were as follows: 74 patients with an incomplete surgical staging operation, 69 patients with EC stage III to IV, 89 patients with non-endometrioid carcinoma, 15 EC patients synchronous with ovary cancer, and 98 patients with incomplete medical records. From a total of 219, 58 study patients were undergoing HT, and 116 patients (controls) were not undergoing HT. The median age was 47.7 years (range, 33–56 years) for the study group and 53.6 years (range, 20–75 years) for the control group; this difference was statistically significant (p<0.001). Compared with control patients, study patients had similar parity (p=0.71), lower BMI (p=0.03), similar number of dissected retroperitoneal lymph node (p=0.87) and were frequently premenopausal (p<0.001). The stage distribution was completely matched between 2 groups. The grade distribution was similar in both the HT and the non-HT groups (p=0.42). The status of LVSI was similar in both groups (p=0.23). The median tumor diameter was statistically larger in study group than in the control group (3.57 vs. 2.50 cm, respectively, p<0.001). The comparison of preoperative CA 125 level was similar in both group (p=0.89). In hormone receptor status, there was no statistical significant difference between the groups (p=0.07). Both groups received similar adjuvant therapy (p=0.80) (Table 1). After propensity score matching, compared with controls, study patients had a similar median age (p=0.06), similar median parity (p=0.26), similar BMI (p=0.56), completely matched stage (p=1.00) and grade (p=1.00), similar LVSI (p=0.42), similar tumor diameter (p=0.57), similar number of dissected retroperitoneal lymph node (p=0.87) and, similar preoperative CA 125 level (p=0.81). The hormone receptor status was statistically significantly more frequently positive in the study group than in the control group (p=0.03). Both groups received similar adjuvant therapy (p=0.06) (Table 1). To further investigate proper matching, we illustrate the distribution of the propensity score and histogram before and after propensity matching (Supplementary Figs. 1 and 2).
Table 1
Patient characteristics before and after propensity score matching
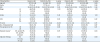
Data are presented as median (range) or number of patients (%).
BMI, body mass index; CA 125, cancer antigen 125; CTX, platinum based chemotherapy; ER, estrogen receptor; LVSI, lymphovascular space invasion; PR, progesterone receptor; RLN, retroperitoneal lymph node; RT, radiotherapy; TD, tumor diameter.
*The + and − signs mean positive and negative.
2. Treatment outcomes
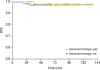
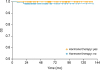
In the univariate analysis, only FIGO stage was significantly associated with disease-free survival (DFS). There was no clinico-pathological variable associated with OS in the univariate analysis (Table 2), and the same results were obtained after propensity score matching (Table 1). Although we performed multivariable Cox proportional hazards model analysis through adjusting for variables including stage, tumor diameter, receptor status, adjuvant therapy, preoperative CA 125, and HT, there was no significant factor identified in the multivariate analysis. After propensity score matching, there was no significant factor identified in the multivariate analysis. The median follow-up period was 64 months (range, 19–135 months) in the study group and 36 months (range, 8–137 months) in the control group. In case group, there was one recurrence and no death. Three recurrences and 3 deaths occurred in the control group. The difference in DFS rate was not significant (p=0.63, Fig. 1). There was no significant statistical difference in OS rate (p=0.32, Fig. 2). After propensity score matching, the median follow-up period 64 months (range, 19–135 months) and 36 months (range, 8–137 months) in the study group and in control group respectively. In the study group, there was one recurrence and no death. Two recurrences and 2 deaths occurred in control group. There was no significant statistical difference in DFS (p=0.47) and OS (p=0.15).
Table 2
Estimated 5-year survival according to prognostic factor: univariate analysis
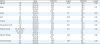
Data are presented as median (%) or number (%).
CTX, platinum based chemotherapy; ER+, estrogen receptor positive; ER−, estrogen receptor negative; LVSI, lymphovascular space invasion; PR+, progesterone receptor positive; PR−, progesterone receptor negative; RT, radiotherapy; TD, tumor diameter; 5YDFS, 5-year disease-free survival; 5YOVS, 5-year overall survival.
DISCUSSION
To the best of our knowledge, this is the first report on the oncologic safety of DRSP/E2 in EC survivors who have undergone surgical menopause. The surgical staging in EC induces surgical menopause in premenopausal patients. The most cumbersome acute menopausal symptoms involve hot flashes and signs of vaginal atrophy [10]. Although most EC patients are postmenopausal, approximately 25% of EC patients are premenopausal and are candidates for severe menopausal symptoms related to abrupt estrogen deprivation [11]. In addition, long-term surgical menopause has been associated with a significantly higher risk of osteoporosis and cardiovascular disease than natural menopause [1213]. Given the survival rate is good in early stage endometrioid type EC, quality of life and estrogen deficiency conditions should be considered, especially for young EC patients.
The use of HT in patients treated for EC is generally not recommended since most ECs are estrogen dependent, with 80% involving endometrioid adenocarcinoma [14]. Because of the mutagenic effect of estrogen on the endometrial tissue, HT had been contraindicated until retrospective reports were published pertaining to this issue. In previous retrospective trials, no increase in recurrence or death rate has been reported [315]. The concern that HT increases the risk of recurrence is mainly based on theoretical considerations. In a recent meta-analysis, of one randomized controlled trial (RCT) and 5 observational studies, comprising a total of 896 HT patients and 1,079 controls, no significant increased risk of recurrence was found in EC survivors using HT (19 recurrence) compared to the control group (64 recurrence) [6]. While results from different reports have shown that HT after EC surgery is likely to be safe, clinicians have still hesitated to use HT for EC patients.
In the present study, all the patients were treated with initial surgical staging procedure, and a unique hormonal therapy was initiated comprising 2 mg DRSP/1 mg E2 at the first postoperative visit, 8 weeks after surgery. After discussion regarding the benefits and risks of HT in EC survivors, HT was administered to patients who were experiencing severe climacteric symptoms. To overcome the limitation regarding a lack of randomization, the patients in the control group were assigned from a group of patients treated in the same period, and who had approximately the same clinical and histopathologic variables.
The 2017 North American Menopause Society (NAMS) position statement suggested that use of HT may be considered in symptomatic women with surgically treated, early stage EC (low risk, grades 1 and 2 endometrioid subtypes with negative ERs and PRs) if other options have not been effective, particularly in women with early surgical menopause who are at higher risk of health consequences related to estrogen loss [16]. However, HT may stimulate tumor growth in patients with more advanced disease, and a non-hormonal approach to management of menopausal symptoms is recommended. There are insufficient data to inform decision-making in the setting of non-endometrioid type EC. Current data, derived from retrospective studies and one RCT [17], suggest that recurrence and death rates are similar for women who have been treated for early stage, low risk EC where HT has been administered [1517].
Most studies regarding HT after EC treatment are retrospective and there has been only 1 RCT to date. According to published data, HT had no negative effect on recurrence and OS after EC treatment; however, but the sample size in most studies has not been sufficiently large to explain the effect of HT on EC recurrence. In 1 RCT, Barakat et al. [17] evaluated the effect of estrogen replacement therapy (ERT) on the recurrence rate and survival in patients with stage I or II EC. In their study, there was a 2.3% of recurrence rate, with 0.8% of disease-specific deaths in ERT user group compared with 1.9% recurrence and 0.6% disease specific death in the placebo group.
Several studies added progesterone to HT, based on findings that progesterone inhibits the stimulatory effect of estrogen on normal and hyperplastic endometrium [1819]. In the present study, we used Angeliq® (2 mg DRSP/1 mg E2) for control of the climacteric symptoms for patients treated for EC. We anticipated that DRSP would protect the proliferative effect of E2 for EC recurrence. In the present study, 1 patient who had a recurrence and no deaths occurred in the study patient group. In the control group, there were 3 recurrences and 3 deaths occurred.
It has been reported that patients whose tumors were positive for ER and/or PR have longer survival than patients whose carcinoma lacks the corresponding receptor [2021222324]. Therefore, we analyzed the clinical outcomes according to the hormone receptor status. There were 34 study patients and 85 controls who ER and/or PR positive. Clinical outcomes were not significantly different between the groups. Five-year DFSs were 96.2% and 96% in the study, and control patients, respectively (p=0.81).
In the present study, the median age was 47.7 years (range, 33–56 years) and 53.6 years (range, 20–85 years) for the study and control groups, respectively, and this difference was statistically significant (p<0.001). A significant number of patients may have been premenopausal in this study. Premenopausal women with EC often have low-grade, early-stage tumors that may be associated with better survival [2526]. Considering this, ovarian preservation in preference to bilateral salpingo-oophorectomy may be considered for very young premenopausal women with early-stage low-risk EC. Further studies regarding this issue are required.
The study limitations include the lack of randomization and the low patient numbers in the HT group. However, we unified the clinical and histopathologic variables in case-control matching to minimize bias. We performed propensity score matching to reduce selection bias and no significant factors were identified between the 2 groups.
In conclusion, while indication for the use of HT were restricted following the Women's Health Initiative (WHI) study, some patients still require HT. Both our study and previous literature show that postoperative HT with DRSP/E2 in EC survivors did not increase recurrence or death rate. Therefore, if patients have severe climacteric symptoms, it appears that HT may be administered to patients, in addition to close follow-up and examination.
 XML Download
XML Download